

Abstract
Background: Radiofrequency thermal ablation (RFA) has been demonstrated to be useful for the treatment of liver neoplasms. The study aimed to evaluate the feasibility and safety of the combination of transarterial chemoembolization (TACE) and RFA, performed simultaneously to treat primary and secondary liver neoplasms. Patients and Methods: From July 2006 to October 2007, 34 patients (21 with HCC and 13 with liver metastases) underwent 37 sessions of treatment. The schedule consisted of: induction TACE (with epirubicin, mitomycin C and lipiodol, or with doxorubicin/irinotecan loaded on microspheres), percutaneous RFA and second TACE. Monopolar RFA was used on 52 nodules, whereas the bipolar multiprobe technique was used in 6 cases. Results: The treatment was well tolerated, with moderate hepatic and hematological toxicity. In total 51 nodules were evaluable for response, with technical success in 45/51 cases (88%). Conclusion: Combined TACE plus RFA is feasible and safe; the preliminary data make it a promising procedure with regard to efficacy and support further investigation.
- Transarterial chemoembolization (TACE)
- radiofrequency thermal ablation (RFA)
- liver neoplasms
Hepatocellular carcinoma (HCC) is one of the most common malignancies, and its incidence is increasing worldwide (1-2). Despite improvements in surveillance and diagnosis, treatments are still a challenge, due to co-existing cyrrhosis with variable liver function that could limit the eligibility of these patients for therapeutical options. Furthermore, the liver is the most common metastatic site from various primary neoplasms and, even if now improved with modern drugs, the outcome of these patients is still unsatisfactory.
Recent reports have highlighted the usefulness of integrated therapies in order to improve the locoregional treatment of primary and secondary liver malignancies. Radiofrequency thermal ablation (RFA) has been demonstrated to be effective for treating focal malignancies in the liver (3-8) as well as in other organs (9-13), with a minimally invasive approach; nevertheless, its usefulness is limited by the size of lesions, resulting in a high rate of local recurrences, particularly for larger tumors (14-16).
RFA procedures need to achieve complete and homogeneous necrosis of the neoplasm as well as a safety margin; hence, due to the possible presence of residual disease and/or satellites, the locoregional treatment should be extended to the perinodular parenchyma. Indeed, also regardless of the tumor type and lesion size, long-term data have shown an appreciable incidence of local relapse after RFA (17). In addition, the risk of incomplete treatment is high in cases of tumoral nodules located close to large vessels or in the proximity of the liver surface close to the stomach and/or bowel. Thus, many studies have investigated the possibility of optimizing the volume of tumor necrosis induced by RFA, both with modern devices and technologies able to increase the energy deposition (18, 19), and also by using chemotherapeutic agents combined with RFA in different schedules (20-22).
Hepatic transarterial chemoembolization (TACE) has been demonstrated to be an interesting locoregional approach in the treatment of liver malignancies, expecially in HCC (23-26).
This study aimed to evaluate the technical feasibility and safety of TACE plus RFA, administered concurrently (“single-step therapy”), in patients with primary and secondary liver neoplasms, unresectable or refusing surgery; the secondary end-point was to assess the efficacy of treatment in terms of complete response and the local control of disease.
Patients and Methods
Study population. From July 2006 to October 2007, 34 patients with 58 primary and secondary liver neoplasms were enrolled into the study. The main inclusion/exclusion criteria are shown in Table I. Pre-treatment evaluation included hepatic contrast-enhanced ultrasound (CEUS) and total body CT scan.
Technique. Firstly, an hepatic arteriography, to determine the parenchymal and neoplastic vascularization, was performed with a percutaneous femoral approach and by using a 4-5 Fr. wire-catheter (Terumo Co., Japan) followed by a 3 Fr. coaxial catheter (Terumo Co., Japan). In one subgroup of patients, chemoembolization was performed using Lipiodol (LUF) mixed with mitomycin C plus epirubicin; a first dose was administered via the hepatic artery (by a selective-superselective infusion), immediately followed, during the same session, by the RFA of the nodules to be treated. During the last stage of this three-stage process, the remaining dose of the antiblastic drug was administered followed by hepatic arterial embolization with a gelatine sponge.
In the other subgroup of patients, doxorubicin or irinotecan, according to the type of neoplasm, loaded on microspheres (Dc-Bead; Biocompatibles, Farnham (GB); Hepasphere; BioSphere Medical, Roissy, Cedex, France), without Lipiodol, were perfused; in these cases, the two-stage procedure was completed by performing RFA immediately after TACE.
The percutaneous US-guided RFA was performed with a 17-gauge monopolar cooled-tip electrode-needle with a 1 to 3 cm-long non-insulated tip (Radionics, Burlington, MA, USA) while, for the lesions larger than 3 cm, bipolar multiprobe 15-gauge electrode-needles (Olympus, Celon AG, Teltow, Germany) with a 4 cm-long exposed section were used.
Response assessment. Local therapeutic efficacy was assessed by contrast-enhanced CT scan, and technical success was defined as non-enhancing tissue including the neoplasm and a safety zone of 5 mm or more from the tumor edges (complete ablation).
The contrast-enhanced CT scan was obtained 48 hours after the treatment in order to detect early complications and to evaluate technical success.
Post-treatment follow-up included upper abdominal contrast-enhanced CT scan one month after the procedure and every three months thereafter, in order to assess the treatment outcome. Local recurrence was defined as the appearance of an enhanced area adjacent to the zone of ablation. Distant recurrence was defined as the detection of new lesions in untreated hepatic areas.
Statystical analysis. The statistical analysis, performed using the Statistical Package for the Social Sciences (SPSS inc, Chicago, IL, USA) software (version 9.0), evaluated the differences in time to progression between the subgroups according to the size and histological type of the neoplasms, as well as to the schedule of treatment. The estimated local tumor progression and overall survival rates were evaluated by the Kaplan-Meier method.
Results
Treatment response. The characteristics of the patients are summarized in Table II. With a median follow-up of 14 months (range 2-17), 31 patients were evaluable for local response and 34 for toxicity. With regard to the three cases not evaluable for response, one patient showed multifocal bilobular disease at the first angiographic step of the procedure, while two patients died early, one due to severe liver insufficiency and the other due to reasons unrelated to the treatment.
Main inclusion/exclusion criteria of the study.
A total of 37 sessions of TACE plus RFA (single-step therapy) for 58 neoplasms was performed. In 23 sessions of TACE, epirubicin (35 mg) plus mitomycin C (15 mg) was used, doxorubicin (100 mg) loaded on Dc-Beads was used in 9 cases and one patient was treated with doxorubicin (100 mg) loaded on Hepasphere. Finally, irinotecan (100 mg) loaded on Dc-Beads was used in 4 patients affected by liver metastasis from colorectal cancer. A monopolar electrode-needle was used in 52 nodules, whereas 6 neoplasms (larger than 3 cm) underwent the bipolar multiprobe technique, with a maximum of four electrode-needles employed simultaneously.
Technical success was evaluable for 51 nodules in 31 patients. Complete necrosis was observed in 45/51 nodules (88%); therefore in six cases (local progressive disease) the treatment was considered incomplete. Intrahepatic recurrences (distant recurrences) distant from the treated areas occurred in 8/34 patients (23.5%).
Three patients received a second session of single-step therapy, two of them due to relapsed disease, while one patient was treated twice due to bilobular disease.
In all patients treated with TACE including LUF, the early CT scan evaluations showed a typical appearance, with a homogeneous deposition of Lipiodol inside the treated nodules, and a wide segmental distribution in the area surrounding the nodules. In the patients treated with microspheres without LUF, the necrotic area was very wide and with sharp outlines compared to the surrounding healthy parenchyma; this radiological aspect was characteristic, not detectable in the cases treated with LUF and considered as a skip area (Figures 1 and 2).
Patient characteristics.
The statistical analysis did not find any significant correlation between local tumor progression and the histopathology, size of the nodules, or the schedule of treatment. The estimated local tumor progression and overall survival rates are showed in Figures 3 and 4, respectively.
Side-effects and complications. The treatment was well tolerated by the majority of patients. Hematological toxicity was moderate; grade 3-4 thrombocytopenia occurred in 4/37 sessions in the cirrhotic patients (10.8%), while grade 3-4 anemia and leukopenia were observed in two cases (5%), requiring blood cell transfusion in one patient.
Elevated serum bilirubin levels occurred in 8 sessions (grade 1-2 for 7 patients, 19%, and grade 3-4 in one patient, 2.7%). Raised aspartate aminotransferase/alanine aminotransferase (AST/ALT) levels were commonly observed, but recovered by the first week with standard post-TACE care.
Six patients (18%) experienced slight, long-lasting fatigue. In addition, grade 1 nausea/vomiting was common and easily manageable. In 4 sessions (10.8%), the patients had moderate abdominal pain and recovered within 12 hours with the administration of analgesics; moderate-grade and short-lasting ascites was observed in two cirrhotic patients with HCC.
One patient, affected by cirrhosis, developed severe impairment of liver function and died due to liver insufficiency.
Discussion
In the current study, the three stages of the treatment had different aims. Firstly, TACE was performed to treat hyper-hypovascular large nodules, ghost nodules and satellites; the subsequent RFA may have been potentiated by the ischemic effect of embolization and by using LUF, thus reducing the heat dissipation due to the blood flow in the adjacent vessels (“heat-sink” effect) (8), and consequently obtaining a larger and more homogeneous volume of necrosis.
In the third stage, TACE could have contributed to prolonging the contact of the peritumoral area with the antiblastic drugs because of the marked hyperemia surrounding the tumoral area including satellites.
Furthermore, we hypothesized that the use of nondegradable microspheres (Dc-Beads and Hepasphere) could optimize and extend the ischemic area, and this was the rationale for using these devices in one subgroup of the patient population. The possibility of increasing the volume of necrosis by the ischemic effect of embolization in combination with RFA has been described in several studies (27-34); in addition, some experimental reports have shown synergism between some antineoplastic drugs, such as doxorubicin, and RF-induced thermal ablation (20-22).
Experimental data have indicated an increased delivery of doxorubicin to the peripheral area treated with RFA, probably due to hyperemia, in comparison with the direct intratumoral injection of doxorubicin (21, 35). However, the increased volume of cellular necrosis induced by the combination of chemotherapy plus RFA could involve multiple mechanisms.
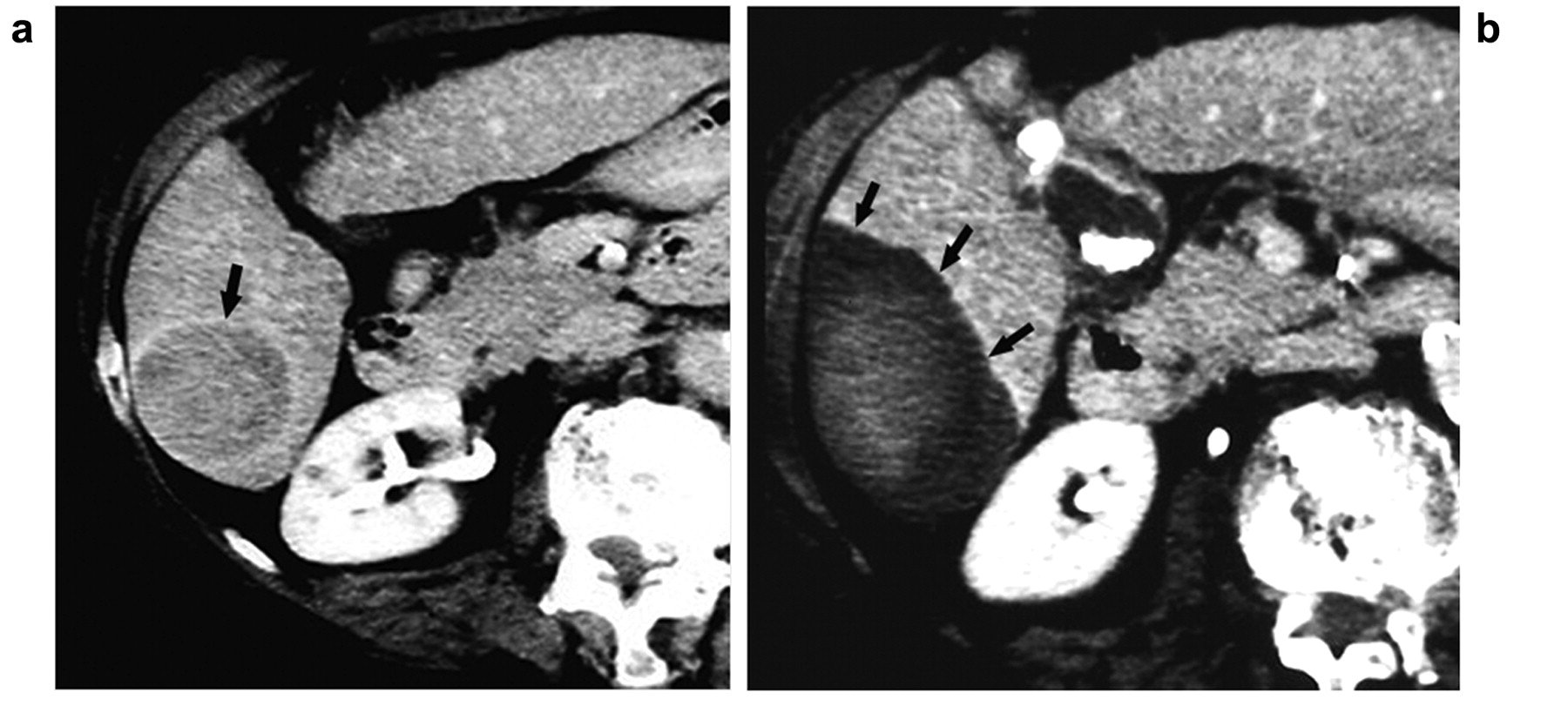
Large nodular HCC measuring 5.5 cm in a 75-year-old woman. (a) Axial venous-phase enhanced CT image showing the neoplasm before “single-step” therapy. (b) After the procedure, CT image demonstrating the necrotic area including the primary nodule, visible as a slightly hyperdense area. The safety zone appears as non-enhancing tissue around the tumor and is very large and clear-cut with respect to the surrounding parenchyma (skip area).
In fact, doxorubicin activity is strengthened by the hypoxia and also by the moderate hyperthermia that is generally detectable at the periphery of a thermally-ablated area (20); in addition, hyperthermia interferes with cellular and vascular structures (21, 36, 37), by increasing the permeability of cellular membranes and by damaging the pump that usually extrudes intracellular doxorubicin (36). Furthermore, RFA slackens the blood flow at 45-50°C (such as in the peritumoral area). Under hypoxic conditions, the cellular uptake of doxorubicin is increased. Therefore, the efficacy of doxorubicin could be optimized at very low doses; hence, the synergism between doxorubicin and RF heating is potentiated, thus increasing the extent of coagulation necrosis.
In the peritumoral area, multiple sublethal injuries occur that generally singly cause reversible cellular damage, potentially representing a possible starting point for relapses; the synergism between the sublethal damage caused by the hyperthermia and the drug-induced cytotoxicity might lead to lethal effects over a larger peritumoral area and, finally, achieve a safety zone never smaller than 5 mm.
In this study, following the reported efficacy of drug-eluting beads as locoregional intra-arterial hepatic therapy (38-42), this device was used with doxorubicin or irinotecan in cases of liver metastasis from colorectal cancer. This drug/device combination was chosen in order to increase the therapeutic efficacy by long-term local drug release within the tumoral tissue, as well as to minimize the toxicity related to systemic levels of the drug.
With regard to the RFA procedure, a very interesting observation was made. In our previous experience (personal, unpublished data) in the treatment of liver neoplasms, a peak of maximal power during RFA ranging from 120 to 160 W was achieved, with values of impedance usually between 85 and 65 Ohms; nevertheless, in these cases, the energy was delivered with very frequent peaks interrupted by pauses (“on-off slots”). However, during the combined treatment it was possible to detect lower values of impedance while delivering very high power. Furthermore, because of the constantly low impedance (usually ranging between 60-80 Ohms), it was possible to deliver progressive amounts of power, at a rate of 10 W/minute, with a steady course without automatic stops of the RFA generator (Figure 5). We think that this could actually correlate with the complete and persistent ischemia caused by the embolization of medium/small vessels and be capable of decreasing the heat-sink effect and consequently optimizing the RFA by a more homogeneous and continuous energy deposition.
The single-step therapy was demonstrated to be feasible and safe. With a median follow-up of 14 months, a satisfactory local response was evident, irrespective of the type of treatment, histopathology and size of the nodules. In all cases, a larger necrotic volume was obtained, despite our expectations based on the effects of RFA alone. Hence, assuming that RFA alone is able to achieve a satisfactory local control in neoplasms smaller than 3 cm, we believe that this combined technique could be applied to obtain a higher rate of complete response in the treatment of lesions with maximum diameter larger than 3-4 cm. The local tumor control is a significant prognostic factor in ablative treatments (33), thus the combined technique could improve the therapeutical results in these cases These preliminary data, even if limited by the heterogeneity and the small patient population, strongly supported further investigation and a longer follow-up to draw definitive conclusions also with respect to long-term efficacy and survival.

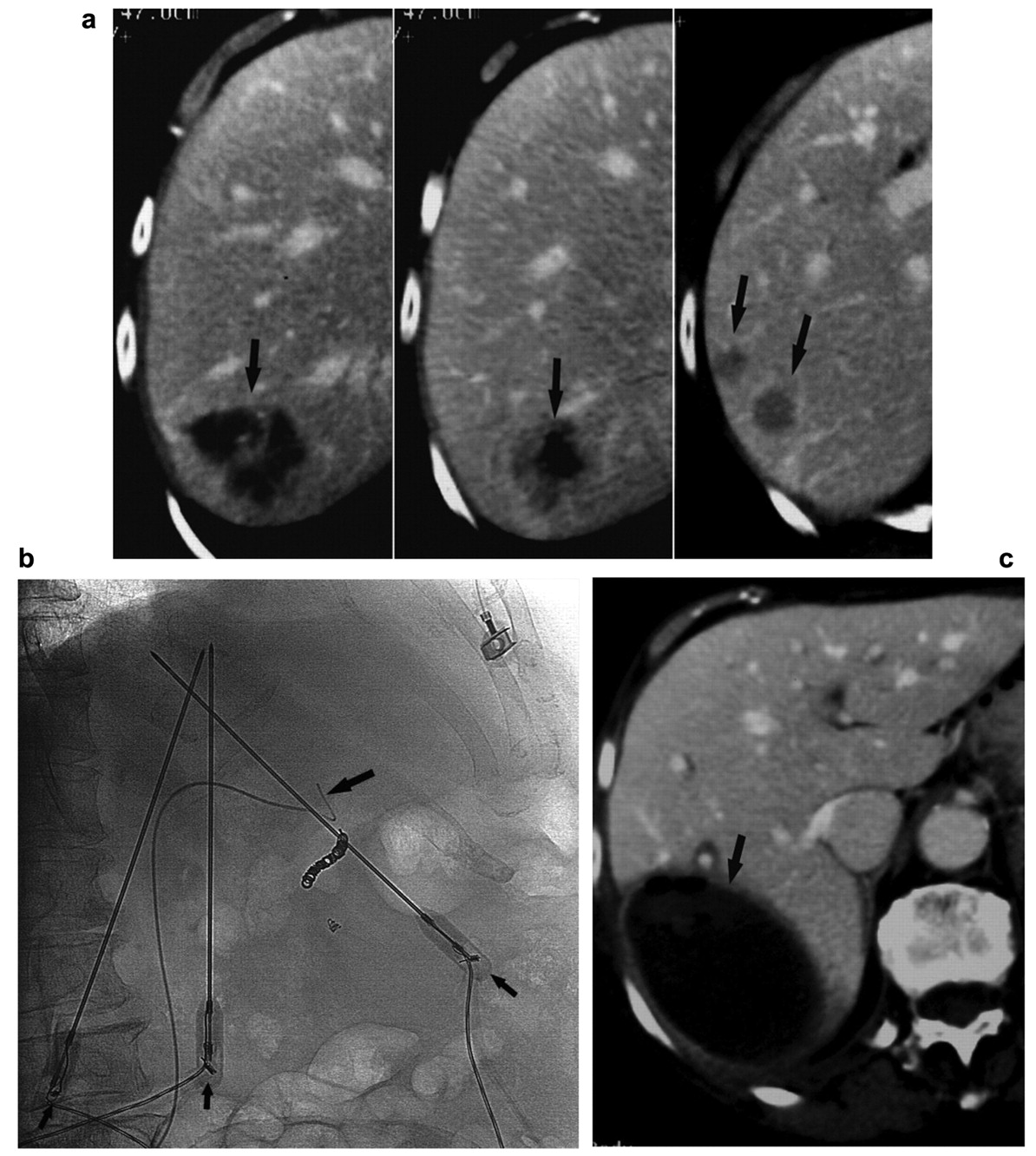
Liver metastases from colorectal carcinoma in a 59-year-old woman, pretreated with RFA of a single nodule and relapsed in three adjacent sites. (a) The axial venous-phase enhanced CT scan showing the three new tumors before single-step therapy. (b) The catheter used for TACE during the procedure, with three electrode-needles simultaneously delivering RFA. (c) After the procedure, CT image showing the very large necrotic area, with maximum diameter of 8.5 cm, including the three nodules plus a safety zone, clear-cut with respect to the surrounding parenchyma (skip area). At the perifery of this area, there is a pseudocapsule representing fibrosis and reparative phenomena.
In addition, the good tolerability of these procedures make it an attractive option to be integrated into a multidisciplinary approach. Hence, patients with HCC, with acceptable hepatic reserve, could receive a more efficacious locoregional treatment, which is minimally invasive and repeatable or subdividable in cases of bilobular disease.

Local progression-free survival after RFA plus TACE (single-step therapy).

Overall survival after RFA plus TACE (single-step therapy).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Energy delivery by RFA in the combined treatment. The power values detected during the RFA (10 W/60 seconds) showed an incremental trend followed by a plateau-phase in which the impedance generally did not exceed 80 Ohm.
Furthermore, liver metastases could be treated with a combination of locoregional and systemic treatment; this approach could be especially useful in patients with colorectal or breast cancer, or other chemosensitive neoplasms with a high risk of extrahepatic metastasis.
On the basis of our results in the group of patients treated with drug-loaded microspheres, we believe that more advanced and efficacious applications will be derived from the use of such devices. In conclusion, the improvement of minimally invasive locoregional procedures, both with specific drugs (such as irinotecan for liver metastases from colorectal cancer) and by up-to-date technologies, such as bipolar multiprobe devices to treat larger nodules, could allow better results in the management of liver malignancies.
Acknowledgements
The authors would like to thank Mrs Teresa Lionetti and Mr Vincenzo Colaluce for their valued technical collaboration.
- Received February 27, 2009.
- Revision received July 2, 2009.
- Accepted July 13, 2009.
- Copyright © 2009 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved