


Abstract
Background/Aim: Mutations in the ASXL transcriptional regulator 1 (ASXL1) and splicing factor 3b subunit 1(SF3B1) genes are commonly observed in myeloid neoplasms and are independent predicative factors for overall survival (OS). Only a few contradictory reports exist on the clinical significance of concurrent ASXL1 and SF3B1 mutations. Previous studies also did not exclude patients with mutations of other genes, which could be confounding factors. Materials and Methods: We identified 69 patients with mutation of only ASXL1, 89 patients with mutation of only SF3B1, and 17 patients with mutations exclusively of both ASXL1 and SF3B1 from our database of 8,285 patients and compared their clinical features and outcomes. Results: Patients with ASXL1 mutations more frequently had acute myeloid leukemia (22.47%) or clonal cytopenia of unknown significance than patients with SF3B1 mutations (1.45%) or with ASXL1/SF3B1 mutations (11.76%). Patients with SF3B1 or ASXL1/SF3B1 mutations were more frequently diagnosed with myelodysplastic syndrome (75.36% and 64.71%, respectively) than patients with ASXL1 mutations (24.72%). Patients with ASXL1/SF3B1 (23.53%) mutations more frequently had myelodysplastic/myeloid proliferative neoplasm than did patients with ASXL1 mutations (5.62%) or with SF3B1 mutations (15.94%). OS of the ASXL1 mutation-only group was worse than that of the SF3B1 mutation-only group with a hazard ratio of 5.83 (p=0.017). Finally, and most importantly, the OS of the ASXL1/SF3B1 co-mutation group was poorer than that of both single-mutation groups (p=0.005). Conclusion: ASXL1/SF3B1 co-mutations portend worse OS than isolated ASXL1 or SF3B1 mutations, which might be due to abnormalities in both the epigenetic-regulatory and RNA-splicing pathways or because two genes instead of one are mutated.
The additional sex combs-like 1 (ASXL1) gene on chromosome 20q11 is involved in gene expression and epigenetic regulation and is a tumor-suppressor gene (1, 2). Somatic mutations in ASXL1 are frequently observed in myeloid malignancies, including clonal cytopenia of unknown significance (CCUS) (3-5), myelodysplastic syndrome (MDS) (6-8), myeloproliferative neoplasm (MPN) (9-14), MDS/MPN (mostly chronic myelomonocytic leukemia, CMML) (1, 15-17), and acute myeloid leukemia (AML) (8, 18-20). ASXL1 mutations in myeloid neoplasms are typically frameshift or nonsense mutations near the last exon and result in the expression of a C-terminally truncated mutant ASXL1 protein and are an independent predicative factor for poor overall survival (OS) and poor event-free survival in patients with AML (6, 20).
Splicing factor 3B subunit 1 (SF3B1) gene on chromosome 2q33.1 participates in pre-mRNA splicing (21, 22). Mutations in SF3B1 are also frequently detected in the above hematopoietic disorders. Patients with SF3B1 mutations represent a distinct patient group, particularly associated with the presence of ring sideroblasts (23, 24). Some studies have associated SF3B1 mutations with favorable clinical prognoses (23, 25, 26), whereas other studies showed contradictory correlations (7, 13, 27, 28).
ASXL1 mutations have been found to coexist frequently with mutations of other genes, including TET methylcytosine dioxygenase 2 (TET2), isocitrate dehydrogenase isocitrate dehydrogenase (NADP+) 1 (IDH1), IDH2, U2 small nuclear RNA auxiliary factor 1 (U2AF1), serine and arginine-rich splicing factor 2 (SRSF2), CCAAT enhancer-binding protein alpha (CEBPA), RUNX family transcription factor 1 (RUNX1), GATA-binding protein 2 (GATA2), NRAS proto-oncogene (NRAS), Janus kinase 2 (JAK2), stromal antigen 2 (STAG2), and SET-binding protein 1 (SETBP1) (18-20, 29-33). However, ASXL1 mutations were reported to be mutually exclusive from those of DNA methyltransferase 3 alpha (DNMT3A), FMS-related receptor tyrosine kinase 3 (FLT3–ITD), and nucleophosmin 1 (NPM1) (18, 29, 34, 35). For mutations of SF3B1, TET2 was the most commonly co-mutated gene, followed by RUNX1, JAK2, and DNMT3A (36).
Co-mutations of ASXL1 with SF3B1 are less frequent (36) and have even been reported to be mutually exclusive by some authors (20, 28, 37). Reports about the clinical significance of ASXL1 and SF3B1 co-mutations are also few and contradictory. Previous studies were also confounded by the inclusion of patients with mutations in genes other than ASXL1 or SF3B1, which may have produced misleading results. The goal of this study was to compare patients with only ASXL1 or SF3B1 mutations or their co-mutation to exclude these confounding factors.
Materials and Methods
Selection of patients. This study was approved by the Institutional Review Board (MCC17964). All patients with next-generation sequencing (NGS) data up to August 2022 (8,285 patients) were searched per IRB protocols. Patients with CCUS, MDS, MPN, MDS/MPN, or AML and only ASXL1 mutation, only SF3B1 mutation, or only ASXL1/SF3B1 co-mutation were selected for this study. Two separate Board-certified hematopathologists reviewed the pathology reports and pathology slides to confirm the diagnoses. The diagnoses were rendered following the revised fifth edition of the WHO Classification of Hematopoietic Malignancies (2); CCUS was defined as patients with cytopenia and somatic mutations indicative of clonal hematopoiesis but not meeting the criteria of MDS. Cytogenetic results and fluorescence in-situ hybridization panel for MDS, including del(5q), del(7q), del(17p), del(20) and trisomy 8, were collected from our electronic database for analysis.
NGS and statistical analyses. As has been described in detail in in our previous studies (38, 39), in-house targeted NGS was performed using Illumina MiSeq or NexSeq500 instruments (Illumina, San Diego, CA, USA). The following most frequently mutated genes in myeloid neoplasms were tested in our in-house, 54-gene panel by NGS: ABL proto-oncogene 1 (ABL1), ASXL1, ATRX chromatin remodeler (ATRX), BCL6 co-repressor (BCOR), BCL6 corepressor-like 1 (BCORL1), B-Raf proto-oncogene (BRAF), calreticulin (CALR), Cbl proto-oncogene (CBL), CBLB,CBLC, cyclin-dependent kinase inhibitor 2A (CDKN2A), CEBPA, colony-stimulating factor 3 receptor (CSF3R), Cut-like homeobox 1 (CUX1), DNMT3A, ETS variant transcription factor 6 (ETV6), enhancer of zeste 2 polycomb repressive complex 2 subunit (EZH2), F-box and WD repeat domain-containing 7 (FBXW7), FLT3, GATA1, GATA2, GNAS complex locus (GNAS), HRas proto-oncogene (HRAS), IDH1, IDH2, IKAROS family zinc finger 1 (IKZF1), JAK2, JAK3, lysine demethylase 6A (KDM6A), KIT proto-oncogene (KIT), lysine methyltransferase 2A (KMT2A), KRAS proto-oncogene (KRAS), MPL proto-oncogene (MPL), MYD88 innate immune signal transduction adaptor (MYD88), notch receptor 1 (NOTCH1), NPM1, NRAS, platelet-derived growth factor receptor alpha (PDGFRA), PHD finger protein 6 (PHF6), phosphatase and tensin homolog (PTEN), protein tyrosine phosphatase non-receptor type 11 (PTPN11), RAD21 cohesin complex component (RAD21), RUNX1, SETBP1, SF3B1, structural maintenance of chromosomes 1A (SMC1A), structural maintenance of chromosomes 3 (SMC3), SRSF2, STAG2, TET2, Tumor protein p53 (TP53), U2AF1, WT1 transcription factor (WT1), and zinc finger CCCH-type, RNA-binding motif and serine/arginine-rich 2 (ZRSR2). All the important regions of ASXL1 and SF3B1 genes were covered in the test. All variants with more than 1% minor allelic frequency in the general population were considered germline mutations and excluded.
The percentages of patients with specific diagnoses or cytogenetic abnormalities were compared by two-way Fisher’s exact test, the OS from the time of mutation detection to the time of last contact or death was compared by Kaplan-Meier survival analysis, while the medians of the ages and the duration of OS were compared two-way Mann-Whitney U-test. Statistical significance was defined as p<0.05.
Results
There were 8,285 patients diagnosed with or suspected to have a myeloid neoplasm and with NGS test results in our database; 1,515 patients had ASXL1 mutations, and 583 had SF3B1 mutations. Most of these patients with ASXL1 or SF3B1 mutations also had mutations of other genes. We also found 97 patients with concurrent ASXL1/SF3B1 mutations, also mostly with other additional genes mutated. We identified 89 patients with only ASXL1 mutations (ASXL1 group), 69 with mutations with only SF3B1 mutations (SF3B1 group), and 17 patients only with co-mutations of ASXL1 and SF3B1 (ASXL1/SF3B1 group) from these patients. The most frequent variants for ASXL1 and SF3B1 mutations were G646Wfs*12 and K554E, respectively, in all three groups.
The median age of the ASXL1 group at 69 years was much younger than that of SF3B1 and ASXL1/SF3B1 groups (76 and 75 years; p=0.012 and p<0.001, respectively). The female-to-male ratios were similar and not statistically significant among these groups (0.77, 0.53, and 0.70, respectively).
The distribution of the diagnoses of the patients in this study is shown in Table I. Patients with ASXL1 mutations more frequently had AML (22.47%) than did patients with SF3B1 mutations (1.45%, p<0.001), and had a trend for being more frequent than in those with ASXL1/SF3B1 mutations (11.76%, p=0.098), possibly because there were very few cases in the ASLX1–SF3B1 group. Similarly, patients with ASXL1 mutations more often had CCUS (33.71%) than did patients with ASXL1/SF3B1 (0%, p=0.002) or SF3B1 mutations (7.25%, p<0.001). However, patients with SF3B1 or ASXL1/SF3B1 mutations more frequently had MDS (75.36% and 64.71%, respectively) than did those with ASXL1 mutations (24.72%) (p<0.001 and p=0.004, respectively). Interestingly, patients with ASXL1/SF3B1 co-mutations (23.53%) were more often diagnosed with MDS/MPN, including MDS/MPN-RS-T and CMML than patients with ASXL1 mutations (5.62%, p=0.035) or SF3B1 mutations (15.94%, but not statistically significant). Finally, as to be expected, in MPN, mostly chronic myeloid leukemia and occasional essential thrombocythemia, only ASXL1 mutations were seen.
Comparison of the diagnoses of patients in this study by ASXL transcriptional regulator 1 (ASXL1) and splicing factor (SF3B1) mutation status.
The associations of ASXL1, and SF3B1 mutations with cytogenetic abnormalities are compared in Table II. Normal cytogenetics was the most frequent finding in all three groups of patients. The proportions of patients with normal cytogenetics were similar in the ASXL1, SF3B1, and ASXL1/SF3B1 groups (62.5%, 66.67%, 56.72%, respectively). Therefore, we can compare the OS of these three groups of patients with normal cytogenetics to avoid the confounding factor of cytogenetic abnormalities, which is known to have an impact on patient prognosis (40). Similarly to a previous report (41), patients with ASXL1 mutations significantly more frequently had myelodysplasia-related cytogenetic abnormalities, namely del(5q) (12.28%) and del(7/7q) (14.04%), than did patients with SF3B1 mutations (both 1.61%, p=0.027 and p=0.011, respectively). Patients with ASXL1 mutations also more frequently had del(5q) and del(7/7q) than did those with ASXL1/SF3B1 co-mutations (0% and 7.14%, respectively), although not statistically significant, likely because of too few specimens in the double-mutation group.
Comparison of the cytogenetics by ASXL transcriptional regulator 1 (ASXL1) and splicing factor 3b subunit 1(SF3B1) mutation status.
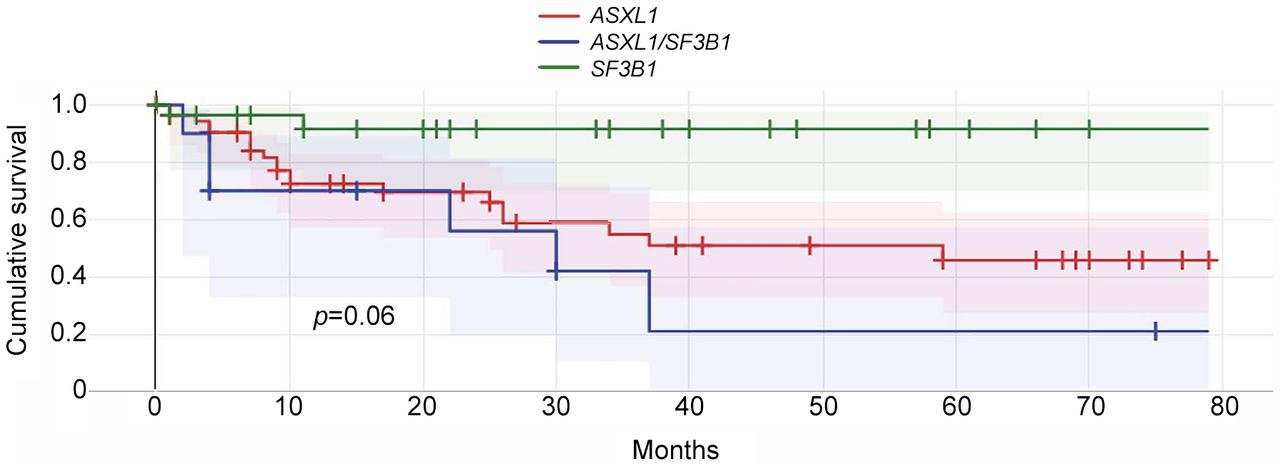
Finally, we compared the OS of the three groups of patients with normal karyotype by Kaplan-Meier survival analysis (Figure 1). Cytogenetic abnormalities are known to affect the prognosis of patients with myeloid neoplasms. Therefore, by only comparing the OS of the patients with normal cytogenetics, the interference of cytogenetic abnormalities is excluded. The ASXL1 group had worse OS than the SF3B1 group, with a hazard ratio of 5.83 (p=0.017). Interestingly, we found that the ASXL1/SF3B1 co-mutation group had poorer OS than both the single mutation groups, with a hazard ratio of 9.84 (p=0.005). In patients with MDS, the median OS of the ASXL1/SF3B1 group was also the shortest (4.7 months), followed by the ASXL1 group (7.6 months) and the SF3B1 group (15.5 months); however, these were not statistically significant, probably because of an insufficient number of patients in these groups.

Comparison of the overall survival of patients with normal cytogenetics by ASXL transcriptional regulator 1 (ASXL1) and splicing factor (SF3B1) mutation status by Kaplan-Meier analysis.
Discussion
It has been reported that >80% of patients with MDS have at least one mutation in different pathways, which include DNA splicing (SF3B1, SRSF2), DNA methylation (DNMT3A, TET2), DNA repair (ATM, BRCC3), chromatin modification (ASXL1, EZH2), RNA transcription (TP53, RUNX1), RAS pathway (KRAS, NRAS), cohesin complex (STAG2, RAD21), and kinases (JAK2, FLT3). It is becoming more and more accepted that molecular abnormalities involving oncogenic genes might take precedence in prognosis of myeloid neoplasms and may be more important than morphological findings, such as the degree of dysplasia. ASXL1 and SF3B1 are among the most mutated genes in patients with myeloid neoplasms. Novel therapeutic strategies targeting ASXL1 mutations have been investigated (42, 43) and produced promising results. New agents targeting SF3B1 in MDS are also under investigation (44).
ASXL1 mutations occur in 10% to 31% of patients with MDS and especially in high-risk MDS (7, 8). ASXL1 mutations resulted in decreased OS and increased rate of relapse following allogeneic hematopoietic stem cell transplantation (1, 4, 5, 42, 45, 46). Patients with MDS without ASXL1 mutation exhibit improved survival and less frequent progression to AML (6, 31, 47-49). In MDS, a combination of 20q deletion, which is considered to have a favorable prognosis, with ASXL1 mutation conferred an inferior 2-year OS rate (50). ASXL1 mutations are the most frequently detected (40-50%) mutations in patients with CMML and portend poorer prognoses (15, 20, 46, 51, 52) and poor response to hypomethylating agents (31). ASXL1 mutations have also been reported in 5% to 11% of patients with AML (31, 34), more likely in older patients, male patients (19, 29, 34), and in those with secondary AML (29). In AML, ASXL1 mutations frequently co-occurred with mutations of RUNX1 (18, 29, 34) and IDH2 (29, 53), M0 karyotype of the French-American-British classification (34, 35), t(8; 21) (34, 54, 55), trisomy 8 (29, 34), and del(7q)/−7 chromosomal aberrations (29). Many studies have associated ASXL1 mutation with poor prognosis in patients with AML (10, 18, 21, 34, 56, 57).
Mutations in SF3B1 were detected in 7% to 53% of MDS cases (31) and in approximately 15% of patients with AML (58, 59). These mutations lead to superior prognoses (31, 45, 47, 60). SF3B1-mutated MDS is now referred to as a new subtype of the disease. It is defined by mutations, cytopenia, morphological dysplasia (with or without ring sideroblasts), bone marrow blasts <5%, peripheral blasts <1%, an indolent clinical course (25, 47), and less frequent progression to AML (26, 47, 60, 61). In MDS/MPN, JAK2 and SF3B1 mutations are predictors of better survival (36, 62). SF3B1-mutated CMML was also found to be a subtype with significant dysplastic features, lower ASXL1 mutation frequency, higher JAK2 V61F mutation frequency, and a more favorable AML-free survival (63).
The frequency of co-mutation of ASXL1 and SF3B1 is reported to be low (approximately 8%) (36) and even mutually exclusive by some authors [reviewed in (20)]. There are also very few and inconsistent reports about the clinical prognosis of ASXL1/SF3B1 co-mutations (20, 64, 65). All the previous studies also included patients with mutations of genes other than ASXL1 and SF3B1, which could significantly confound the analysis and skew the results. In this study, we selected patients with only ASXL1 or SF3B1, or ASXL1/SF3B1 co-mutations to avoid confounding factors from other genes.
From our database of 8,285 patients diagnosed with or suspected to have myeloid neoplasms and NGS results, we identified 89 patients with only ASXL1 mutations, 69 with only SF3B1 mutations, and 17 with ASXL1 and SF3B1 co-mutations.
Our study showed that patients with ASXL1 mutations more frequently had AML and CCUS than did those with SF3B1 mutations and ASXL1/SF3B1 co-mutations. On the contrary, patients with SF3B1 or ASXL1/SF3B1 mutations more frequently had MDS than did patients with ASXL1 mutations. Patients with ASXL1/SF3B1 mutations more frequently had MDS/MPN than did patients with ASXL1 or with SF3B1 mutations. As expected, only ASXL1 mutations were seen in patients with MPN, which is expected to lack myelodysplasia and, therefore, lack SF3B1 mutation.
Normal cytogenetics was the most frequent finding, similar among all three groups of patients. Consistent with a previous report (41), ASXL1 mutations were significantly more frequent than SF3B1 and ASXL1/SF3B1 co-mutations in patients with myelodysplasia-related cytogenetic abnormalities, such as del(5q) and del(7/7q).
Among patients with normal cytogenetics, those with ASXL1/SF3B1 double mutations showed the worst prognosis out of the three groups (Figure 1), likely because genes in both the epigenetic regulatory and RNA-splicing pathways are affected. In addition, the more genes that were mutated, the worse the prognosis, which has been shown by many previous studies (66-68). Janusz et al. reported that the presence of at least two mutations concomitant with that of SF3B1, including ASXL1, had an adverse impact on survival compared to SF3B1 mutation alone and fewer than two additional mutations (65). The co-mutation of SF3B1 with SRSF2, IDH2, BCOR, NUP98, and STAG2 were also linked to poor prognoses. Mangaonkar et al. also studied the effect of ASXL1 and SF3B1 co-mutation on the OS of patients with MDS with ring sideroblasts and found slightly different results (64). They reported that the median OS was highest in those with mutated SF3B1 without ASXL1 mutation, followed by mutation of both ASXL1 and SF3B1, then wild-type for both ASXL1 and SF3B1, and mutation of ASXL1 with wild-type SF3B1. However, their studies included patients with mutations of other genes. Their study also had fewer patients with ASXL1/SF3B1 co-mutation than our study. Further studies with more patients and with mutations of only these two genes are necessary to clarify the difference in our results.
In summary, our study suggests that concurrent ASXL1 and SF3B1 mutations confer worse OS than mutation of ASXL1 or SF3B1 alone. This might be due to disruption in both the epigenetic-regulatory pathway and the RNA-splicing pathway, or because two genes instead of one are mutated in these patients. However, larger cohort studies are necessary to confirm these results.
Acknowledgements
The Authors thank Janis De La Lglesia and Hebert Gerard for scientific editing.
Footnotes
Authors’ Contributions
Jinming Song and Hailing Zhang designed the projects, collected, and analyzed the data, and wrote the article; Lynn Moscinski, Haipeng Shao, and Mohammad Hussaini made suggestions and edited the article; Ethan Yang participated in the data analysis and prepared the tables.
Conflicts of Interest
There are no conflicts of interest to declare.
- Received January 12, 2023.
- Revision received March 4, 2023.
- Accepted March 14, 2023.
- Copyright © 2023, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.