


Abstract
Background/Aim: Immunomodulatory therapy with Tocilizumab (TCZ), a monoclonal antibody against interleukin-6 receptor-alpha, has been endorsed by the World Health Organization and other major regulatory bodies, as part of the standard-of-care therapy for severe or critical COVID-19 cases despite discordant trial outcomes. The aim of the present study was to report the experience of our center regarding TCZ routine use in severely ill COVID-19 patients who were hospitalized during the third pandemic wave in Greece. Patients and Methods: From March 2021 to December 2021, we retrospectively analyzed COVID-19 patients with radiological findings of pneumonia and signs of rapid respiratory deterioration that were treated with TCZ. The primary outcome included the risk of intubation or/and death in TCZ-treated patients compared to matched controls. Results: TCZ administration was neither predictive of intubation and/or death [OR=17.5 (95% CI=0.47-652.2; p=0.12)] or associated with fewer events (p=0.92) in multivariate analysis. Conclusion: Our single-center real-life experience is in line with recently published research, revealing no benefit from TCZ routine use in severely or critically ill patients with COVID-19.
Coronavirus Disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is a novel infectious disease that emerged in the city of Wuhan, China at the end of 2019 and has unprecedently afflicted humankind resulting, so thus far, in more than 660 million confirmed cases and 6.7 million deaths worldwide (1). Its unpredictable and extremely variable disease course, ranging from asymptomatic cases and mild upper respiratory tract illness to severe, life-threatening interstitial pneumonia and multi-organ failure, has been a major scientific focus and the identification of effective drugs for treatment and prevention has become imperative (2). The replication cycle of SARS-CoV-2 and the subsequent aberrant immune responses to the virus are thought to be the main components of COVID-19 etiopathogenesis, as well as attractive potential drug targets for antiviral therapy (3).
Tocilizumab (TCZ), a monoclonal antibody against interleukin-6 receptor-alpha (IL-6Ra), is indicated for the treatment of several inflammatory diseases, such as rheumatoid arthritis, giant cell arteritis, juvenile idiopathic arthritis, and cytokine release syndrome (4). Based on the findings that within the cytokine storm, IL-6 plays a pivotal role in COVID-19 progression and is a prognostic indicator of poor outcomes, TCZ has been the most widely evaluated therapeutic intervention for severely or critically ill patients since the pandemic onset (5, 6). Despite the discordant trial outcomes regarding TCZ efficacy, ranging from significantly reduced need for mechanical ventilation, and mortality rates to evident treatment-related harm, it is now endorsed by the World Health Organization (WHO) and other regulatory bodies, such as the U.S Food and Drug Administration (FDA), the Infectious Diseases Society of America (IDSA), the National Institutes of Health (NIH), the European Medicines Agency (EMA), and several national committees as part of the standard of care (SoC) therapy for severe or critical COVID-19 (7-12).
The aim of the study was to assess the efficacy of TCZ in patients with severe COVID-19 pneumonia, and signs of rapid respiratory deterioration, during the period following after the recommendation of IL-6R blockade treatment by NIH COVID-19 Treatment Guidelines Panel until the prevalence of Omicron variant that causes significantly less morbidity (11). This time frame corresponds to the third pandemic wave in Greece during which the emergence and predominance of the Delta variant were recorded.
Patients and Methods
Study design. This was a single-center, retrospective observational study of consecutive COVID-19 patients admitted to the Infectious Diseases Unit of a reference hospital in Athens, Greece, during a 10-month period (March 2021-December 2021). Study protocol was approved by the Institutional Review Board of SOTIRIA General Hospital and was conducted in accordance with the Helsinki Declaration of Human Rights (approval number: 3247_06/02/2022). In compliance with the local regulations, Informed Consent Form was waived because of the retrospective design of the study and anonymous clinical data were used in the analysis.
Patients. Severely ill COVID-19 patients, aged ≥18 years, with radiological findings of pneumonia and signs of rapid respiratory deterioration, who had received a single dose of TCZ alongside SoC, were analyzed. Patients in whom TCZ administration was contraindicated or there was a lack regarding variables of interest were excluded. COVID-19 severity was assessed based on clinical parameters and patient oxygen requirements; severe disease was defined as patients meeting one or more of the following criteria: i) oxygen saturation as measured by pulse oximetry (SpO2) ≤94% on room air, ii) PaO2/FiO2 <300 mm Hg, iii) tachypnea (respiratory rate ≥30 breaths per minute) or iv) lung infiltrates >50% (13). According to the national algorithm for the therapeutic management of hospitalized COVID-19 patients with severe disease, SoC consisted of a 5-day course of Remdesivir, dexamethasone (6mg, once daily, for up to 10 days) and a prophylactic dose of anticoagulation with low-molecular weight heparin (14, 15). In our center, at the time, a single dose of TCZ (8 mg/kg IV, maximum dose of 800 mg) was administered to recently admitted patients with rapidly increasing oxygen requirements or in need of high-flow nasal cannula oxygen therapy, and signs of hyperinflammation (e.g., CRP ≥7.5 mg/dl) upon request to the national Medicines Evaluation Committee. Medical records were used to extract the data used in the analysis, including demographics, clinical and laboratory parameters, therapeutic interventions and outcomes.
Endpoints. We sought to evaluate TCZ efficacy in severely ill COVID-19 patients that presented rapid respiratory deterioration. Therefore, the primary endpoint of interest was the assessment of the risk of intubation or/and death in TCZ-treated patients. A propensity-score matching (1:1) analysis was performed to match the baseline characteristics [age, Charlson’s Comorbidity Index (CCI), paO2/FiO2 ratio at admission] of the TCZ-treated patients versus matched controls that were managed exclusively with SoC. All the patients (TCZ-treated, matched controls) included in the final analysis were hospitalized during the same pandemic wave.
Statistical analysis. Descriptive statistics (counts and percentages) were used for categorical variables and age was presented as mean±standard deviation (SD). Odds ratios (OR) [95% confidence intervals (CI)] were reported for the variables retained in the final multivariate logistic regression analysis. Statistical Package for Social Sciences (SPSS), version 19.0 (SPSS Inc., Chicago, IL, USA) was used and statistical significance was set at 0.05 level.
Results
Overall, 64 patients were included in the study, 32 patients per group. Males accounted for the majority of the study population and the mean age was 59 (SD:17.1) and 56 (SD:16.5) years in the TCZ-treated and matched controls, respectively. The entire TCZ group was managed with dexamethasone and anticoagulants, while 2 in 3 matched controls, who progressed to respiratory failure, received corticosteroids. Statin use was reported by 5 TCZ-treated and 9 control patients.
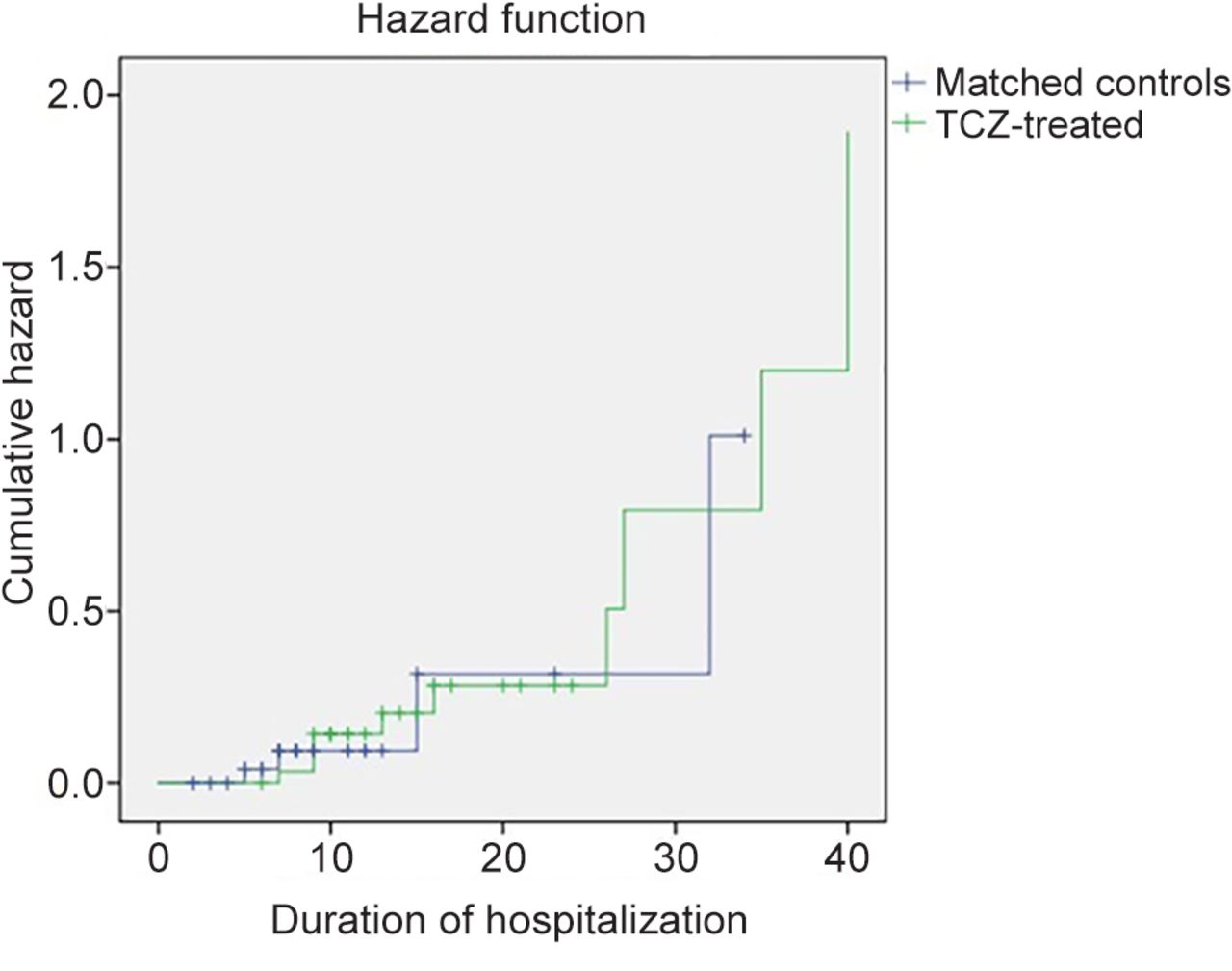
In the analysis of TCZ-treated patients and matched controls, more frequent events (intubation and/or death) were observed in the TCZ group (n=11/32 vs. n=4/32, respectively, p=0.04). In multivariate logistic regression analysis (Table I), upon adjustment for several confounders (e.g., CCI, use of corticosteroids, remdesivir, statins, and anticoagulants administration, CRP levels at admission), TCZ administration did not predict the outcome of interest [OR=17.5 (95% CI=0.47-652.2; p=0.12)]. Moreover, CCI conferred an increased risk of intubation and/or death [OR=2.8 (95% CI=1.4, 5.6-p=0.004)], whereas remdesivir administration [OR=0.02 (95% CI=0.0-0.92; p=0.02)], as well as statin use [OR=0.02 (95% CI=0.001-0.75; p=0.03)] were shown to decrease the risk for adverse events. In Kaplan-Meier survival analysis (Figure 1), with a median follow-up of 10.5 days, TCZ administration was not associated with fewer events (p=0.92).
Logistic regression analysis of factors associated with the risk of intubation and/or death.

Kaplan-Meier survival analysis for the events of intubation and/or death of patients who received Tocilizumab (TCZ) alongside standard of care (SoC) therapy (TCZ-treated) and those who received exclusively SOC (matched controls) by the time of hospitalization.
Discussion
The present study assessed the efficacy of the routine use of TCZ in severely ill COVID-19 patients that presented rapid respiratory deterioration. TCZ administration was neither predictive of the outcome of interest (risk of intubation and/or death) or associated with fewer events. Notably, statin use and treatment course with remdesivir conferred a decreased risk for adverse events, as reported in previously published meta-analyses (16-19).
So far, several randomized clinical trials have failed to demonstrate even a marginal benefit of TCZ in reducing the risk for mechanical ventilation and/or death in severe COVID-19 (20). In the randomized, double-blind, placebo-controlled trial conducted by Stone et al., 243 moderately ill COVID-19 patients with laboratory findings of hyperinflammation (CRP >50 mg/l, or ferritin >500 ng/ml, or D-dimer >1,000 ng/ml, or lactate dehydrogenase >250 U/l), and at least two of the following signs: fever (T>38°C), pulmonary infiltrates, or need for supplemental oxygen were recruited. TCZ was not found to be effective in either reducing the likelihood of intubation and/or death [HR=0.83 (95% CI=0.38-1.81; p=0.64)] or preventing disease progression [HR=1.11 (95% CI=0.59-2.10; p=0.73)]. It is worth mentioning that within the study population, only a subset of patients was managed with remdesivir, whereas no one received corticosteroids (21). A RCT conducted in 24 hospitals across Italy, and designed to evaluate the effect of TCZ administration in the early course of SARS-CoV-2 infection, was prematurely interrupted upon an interim futility assessment, since no benefit in terms of mortality and/or clinical progression was shown in TCZ-treated patients (22). In the EMPACTA trial, a total of 389 patients with severe COVID-19 pneumonia receiving low-flow oxygen therapy were randomly assigned in a 2:1 ratio to receive TCZ alongside SoC versus SoC; a significantly reduced likelihood of progression to the composite outcome of intubation or death was observed in the TCZ-treated group [HR=0.56 (95% CI=0.33-0.97; p=0.04)], even though TCZ failed to improve the all-cause mortality by day 28 (23). Similarly, in the COVACTA trial, 452 patients with evidence of severe COVID-19 pneumonia, as confirmed by radiological (bilateral chest infiltrates on chest radiography or computed tomography) or clinical findings (SatO2 <93%, FiO2:21% or PaO2/FiO2 <300 mmHg) were randomized; TCZ use did not result in better clinical outcomes [mortality rate at day 28: 19.7% vs. 19.4%, weighted difference:0.3 percentage points (95% CI=−7.6-8.2; p=0.94)], but in lower length of ICU or hospital stay (24). Of note, the different outcomes between the EMPACTA and the COVACTA trial, are attributed to patients’ baseline characteristics and the administered SoC; in the EMPACTA, the majority of the study population was in need of low-flow oxygen at enrollment, whereas 54.6% and >80% of the patients were managed with remdesivir and systemic corticosteroids, respectively. Patients with a broader range of disease severity were enrolled in the COVACTA, of whom less than half were treated with corticosteroids and approximately 1 in 10 received remdesivir (23, 24). Lastly, despite high expectations, several other trials designed to evaluate the efficacy of IL-6 receptor blockade did not meet their endpoints, including the risk of mechanical ventilation and mortality (25-29).
TCZ endorsement by the WHO is mainly supported by the RECOVERY and REMAP-CAP trial outcomes, as well as the results of diverse published meta-analyses that demonstrated the favorable effect of TCZ in the treatment of patients with severe COVID-19 (8). In the RECOVERY trial, which included 4,116 hypoxemic patients with signs of systemic inflammation (CRP ≥75 mg/l), mostly managed with corticosteroids (82%), TCZ was reported to reduce mortality [31% vs. 35%, rate ratio: 0.85 (95% CI=0.76-0.94; p=0.0028)] and improve the chances of hospital discharge [57% vs. 50%, rate ratio:1.22 (95% CI=1.12-1.33; p<0.0001)]. Moreover, among non-intubated patients, progression to the composite endpoint of invasive mechanical ventilation or death was less likely in the TCZ-allocated group [35% vs. 42%, risk ratio:0.84 (95% CI=0.77-0.92; p<0.0001)]. Interestingly, even though TCZ efficacy was maintained across the different subgroup analyses (e.g., days since symptoms onset, respiratory support), in the corticosteroids subgroup, TCZ was beneficial only among those receiving systemic corticosteroids, thus highlighting the need for concomitant administration of TCZ and corticosteroids in patients with severe COVID-19 (30). In a prospective meta-analysis of 27 RCTs, the latest and largest one so far, that involved more than 10,000 hospitalized COVID-19 patients, TCZ was associated with lower 28-day-all-cause mortality [OR=0.83 (95% CI=0.74-0.92; p<.001)] (31). In line with the RECOVERY findings, the concomitant administration of TCZ and corticosteroids was shown to further reduce the all-cause mortality [OR=0.77 (95% CI=0.68-0.87)] or the likelihood of progression to invasive mechanical ventilation, extracorporeal membrane oxygenation (ECMO), or death at day 28 [OR=0.69 (95% CI=0.61-0.78)] (30, 31). The main limitations of the meta-analysis are i) the optimal timing of TCZ administration was not addressed and ii) there was no baseline risk stratification for death, since TCZ might be not indicated for patients with modest respiratory requirements and stable clinical status.
The discrepancies in the aforementioned studies can be attributed to the different criteria used as indicators for TCZ administration, including: i) differences in timing of intervention in relation to clinical deterioration, ii) patients’ baseline characteristics, iii) disease severity and iv) mostly the continuing evolution of SoC. Simultaneously, the emergence of different viral variants might explain the controversial results. In the case of our study, all the patients were hospitalized during the same pandemic wave with a predominance of Delta variant, had the same indications for TCZ administration (e.g., disease severity, CRP levels, rapid respiratory deterioration) and were managed with the same therapeutic algorithm. As compared with the subsequent approval by the EMA and emergency use authorization by the FDA of anakinra in the treatment of COVID-19, the administration of the immunomodulatory agent is supported either by scores extracted by the clinical trials’ data or coupled by the testing of a specific biomarker (namely Soluble Urokinase Plasminogen Activator Receptor-suPAR) (9, 12, 32-36). This paradigm may pave the way for a better refinement of the population of COVID-19 patients that would benefit from immunomodulatory treatments in the future.
The results of the present study should be interpreted in the light of certain limitations such as its retrospective character, the small number of patients analyzed and the wide confidence intervals for efficacy comparisons.
Conclusion
The findings of our study do not support the routine use of TCZ in hospitalized patients with severe COVID-19 pneumonia and rapid respiratory deterioration. Although immunomodulatory therapy with TCZ has been prequalified as the SoC therapy in severe and critical COVID-19, the discrepancies in trial outcomes highlight the need for the conduct of more targeted studies and meta-analyses designed to identify interpatient variability and select the subsets of patients at higher risk for intubation and/or death that could benefit from IL-6 blockade treatment.
Footnotes
Authors’ Contributions
Conceptualization, V.R., A.K., K.N.S. and G.P.; methodology, V.R., A.K., K.N.S. and G.P.; software, V.R and A.K.; formal analysis, A.K.; investigation, M.E.L, T.K. and O.S.; data curation, V.R. and A.K.; writing—original draft preparation, V.R.; writing—review and editing, M.E.L., A.K., V.S.; T.N.; E.K.; K.A.; K.N.S and G.P.; supervision, A.K., K.N.S. and G.P. All Authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
The Authors declare no conflicts of interest.
- Received January 23, 2023.
- Revision received February 10, 2023.
- Accepted February 21, 2023.
- Copyright © 2023, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.