


Abstract
Background/Aim: Gastric-type endocervical adenocarcinoma (GEA) is a rare but distinct histological type of gynecological malignancy. This study aimed to conduct a comprehensive analysis of the cytological features of GEA. Patients and Methods: We reviewed 18 cytological samples obtained from 14 patients with GEA. All cytology slides were prepared using conventional smear and liquid-based preparations. We examined the differences between the cytological features of GEA and usual-type endocervical adenocarcinoma (UEA). Results: The cytological samples of GEA exhibited flat, honeycomb-like cellular sheets (p=0.035), vesicular nuclei (p=0.037) with prominent nucleoli (p=0.037), and vacuolated cytoplasm (p<0.001) more frequently than those of UEA, irrespective of the sampling site and preparation method. UEA showed three-dimensional cellular clusters (p<0.001), peripheral nuclear feathering (p<0.001), and nuclear hyperchromasia (p=0.014) more frequently than GEA. Conclusion: GEA can be identified cytologically based on the presence of flat, honeycomb-like sheets of tumor cells possessing vesicular nuclei, prominent nucleoli, and abundant vacuolated cytoplasm.
Cervical carcinoma is the fourth-most frequently diagnosed carcinoma and fourth-leading cause of carcinoma-related mortality in women worldwide (1-6). Cytology-based cervical screening has decreased the incidence and associated mortality rate of cervical carcinoma (7). Despite the declining incidence of cervical carcinoma, the proportion of adenocarcinomas arising from the uterine cervix has risen steadily (8, 9). Endocervical adenocarcinoma (EAC) accounts for 20-25% of all cervical carcinomas (7). EAC comprises a heterogeneous group of tumors of varying etiology and morphology (10-12). Since the 2014 World Health Organization (WHO) Classification of Tumors of Female Reproductive Organs (13) did not fully reflect the current understanding of diverse mechanisms underlying endocervical glandular carcinogenesis, a novel classification system was proposed to provide an updated framework for EAC classification. The International Endocervical Adenocarcinoma Criteria and Classification (IECC) reliably segregated EACs into human papillomavirus (HPV)-related and HPV-unrelated tumors according to the presence or absence of HPV infection-related morphology (apical mitotic figures and basal apoptotic bodies), which is easily identifiable under scanning magnification (12). With the adoption of the 2018 IECC, the updated 2020 WHO Classification of Female Genital Tumors (14) designated these tumors as HPV-associated (HPVA) and HPV-independent (HPVI) EACs. Most EACs, including HPVA usual-type EACs (UEAs), are causally related to oncogenic infections with high-risk HPV (15), whereas HPVI EACs account for 10-20% of all EAC cases. Although the latter is a relatively rare entity, it often presents diagnostic or therapeutic challenges owing to the distinct histological and molecular characteristics and different response to standard therapies (16).
Gastric-type EAC (GEA) is the most common subtype of HPVI EAC (11, 16). GEA presents with characteristic histological features and immunophenotypes, including irregular, angulated, or dilated glands; abundant, clear, or pale eosinophilic cytoplasm; distinct cell borders; varying degrees of nuclear atypia; desmoplastic stromal reaction; negative or patchy p16 positivity; and a mutant p53 immunostaining pattern in approximately half of the cases (16). GEA is consistently diagnosed at an advanced stage and exhibits more aggressive behavior and worse prognosis than those of HPVA EAC (1, 2).
Although the aggressive clinical course of GEA encourages the use of cytological detection methods at the early stage, information on the cytopathological features of GEA is limited. Despite its characteristic histological features, the cytological diagnosis of GEA is often challenging. Liquid-based preparation (LBP) can improve the specimen quality by providing a standardized method for collecting cervical cytology samples and dispersing cells in a thin, relatively inflammation-free layer (17-19). This reduces the likelihood of unsatisfactory smears and increases the detection rate of cytomorphological abnormalities. Although LBP cytology has become a common screening method for cervical carcinoma, data on the features of liquid-based cytology of GEA are scarce.
In this study, we comprehensively analyzed the cytological characteristics of GEA and examined whether significant differences existed between the cytological features of GEA and UEA. We elucidated the characteristic cytological features of GEA and verified that they were consistent with the typical histological features of GEA.
Patients and Methods
Patient selection. This study was approved by the Institutional Review Board of Samsung Medical Center (protocol number: 2023-02-067; approval date: February 18, 2023). The institutional databases were searched for endocervical tumors reported as “gastric-type adenocarcinoma”, “mucinous adenocarcinoma of gastric type”, or “gastric morphology” between 2018 and 2020. Fourteen patients with GEA were identified, and 18 cytological specimens were available. Fifteen UEA cases were also collected to compare the clinicopathological and cytological features between GEA and UEA. The final diagnoses of GEA and UEA were established by two gynecological pathologists (S.P. and H-S.K.) according to the morphological criteria described in the 2020 WHO Classification of Tumors of the Female Genital Tract (14).
Clinicopathological data collection. We thoroughly reviewed the electronic medical records and pathology reports of 14 GEA and 15 UEA patients to acquire the following clinicopathological and follow-up information: patient’s age at initial diagnosis, extension into the vagina and parametrium, pelvic or para-aortic lymph node metastasis, initial International Federation of Gynecological and Obstetrics (FIGO) stage (20), initial treatment, adjuvant treatment, post-treatment recurrence and distant metastasis, disease-free survival (DFS), survival status, and overall survival (OS).
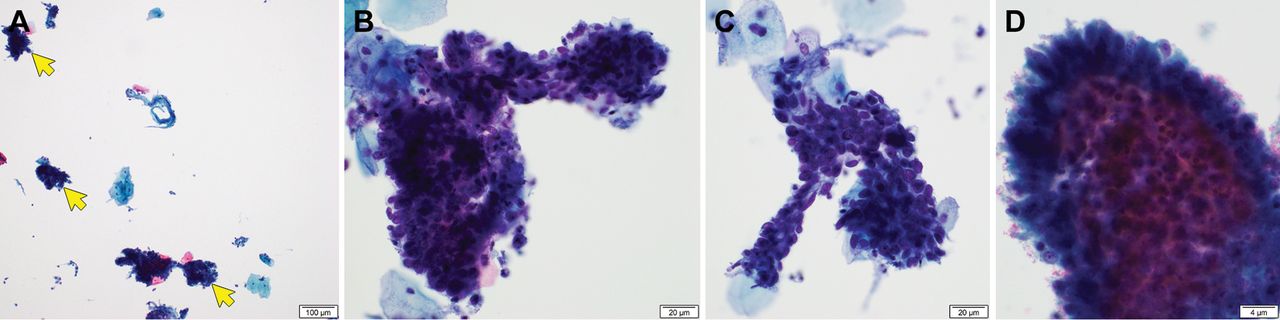
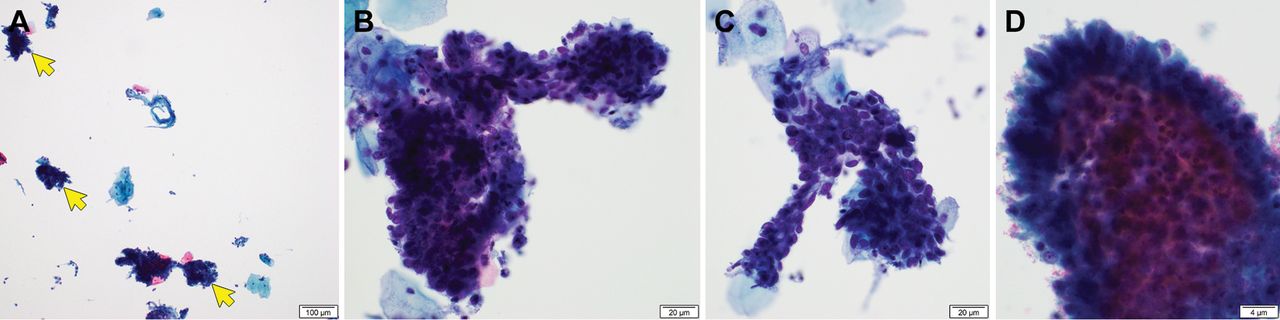
Cytological examination. The preparation methods included ThinPrep (Hologic, Marlborough, MA, USA), SurePath (Becton, Dickinson and Company, Franklin Lakes, NJ, USA), and conventional smears. Two gynecological pathologists (S.P. and H-S.K.) independently reviewed 18 cytology slides obtained from 14 patients with GEA to obtain the following cytomorphological features: hypercellularity (Figure 1A and B), arrangement of the cells as flat, honeycomb-like sheets (Figure 1C and D), foamy or vacuolated cytoplasm (Figure 1E and F), vesicular chromatin (Figure 1G), prominent nucleoli (Figure 1H), mitotic figure (Figure 1I), pink (Figure 1J) or golden-yellow (Figure 1K) mucin, intracytoplasmic neutrophil entrapment (Figure 1L), three-dimensional clusters (Figure 2A), nuclear enlargement, nuclear hyperchromasia (Figure 2B), peripheral nuclear feathering (Figure 2C and D), and abrupt anisonucleosis. Disagreements between pathologists were resolved by consensual discussions. For comparison, we also reviewed the cytology slides of 15 control cases of UEA and collected the above-mentioned cytomorphological parameters. The HPV test results, surgical specimens, and immunostained slides were also reviewed.

Cytological features of gastric-type endocervical adenocarcinoma. (A and B) Hypercellular smear. (C and D) Flat, honeycomb-like cellular sheets of varying shapes and sizes. (E and F) Foamy or vacuolated cytoplasm and distinct cell borders. (G and H) Vesicular chromatin and prominent nucleoli. (I) Mitotic figures (white arrows). (J) Golden-yellow mucin (yellow arrows). (K) Pink mucin (green arrows). (L) Neutrophil entrapment (blue arrow). Staining method: A-K, Papanicolaou staining; L, hematoxylin and eosin staining. Original magnification: A and B, 40×; C, 80×; D, 100×; E-G, 400×; H, 600×; I-K, 200×; L, 400×. The scale bar is shown in the lower right corner of each panel.
Cytological features of usual-type endocervical adenocarcinoma. (A) Three-dimensional cellular clusters (yellow arrows). (B) Nuclear hyperchromasia. (C and D) Peripheral nuclear feathering. Staining method: A-D, Papanicolaou staining. Original magnification: A, 40×; B and C, 100×; D, 400×. The scale bar is shown in the lower right corner of each panel.
Statistical analysis. An independent two-sample t-test, Pearson’s chi-squared test, Fisher’s exact test, or linear-by-linear association test was used to examine the differences in the clinicopathological and cytological characteristics between GEA and UEA. Univariate survival analysis was performed to examine the prognostic significance of the histological type with respect to DFS and OS. A Kaplan-Meier plot was employed to depict the survival curves. All statistical analyses were performed using IBM SPSS Statistics for Windows version 23.0 (IBM Corp., Armonk, NY, USA). Statistical significance was set at p<0.05.
Results
Clinicopathological characteristics of GEA. Table I summarizes the baseline clinicopathological features. Their mean age was 56 years (range=38-79 years). Five (35.7%) and 10 (71.4%) tumors extended into the vagina and parametrium, respectively. Eight patients (57.1%) had lymph node metastases at the initial diagnosis. The distribution of the initial FIGO stage was as follows: I (2/14, 14.3%), II (4/14, 28.6%), IIIC1 (4/14, 28.6%), IIIC2 (2/14, 14.3%), and IV (2/14, 14.3%). One patient with stage IVB tumor received chemotherapy as the initial treatment, and the other patient first underwent surgery followed by chemotherapy. Both patients with stage IIIC2 tumors received concurrent chemoradiation therapy (CCRT) and surgery as the initial treatment. Eight of the 10 patients with IB1-IIIC1 tumors underwent surgery, and six patients received adjuvant CCRT. Radical hysterectomy was performed in nine of 10 patients who underwent surgery. Bilateral pelvic lymph node dissection was performed in 10 patients, while the para-aortic lymph nodes were removed in three patients. All patients developed post-treatment recurrence and metastases. The mean DFS duration was 12.2 months (range=2.0-39.0 months). Five (35.7%) patients succumbed to the disease. The mean OS was 22.9 months (range=5.9-56.9 months).
Baseline clinicopathological characteristics of gastric-type endocervical adenocarcinoma.
Differences in clinicopathological characteristics between GEA and UEA. Table II summarizes the clinicopathological differences between GEA and UEA. Patients with GEA (mean age: 55.8 years) were older than those with UEA (50.5 years), but the difference was not significant. Vaginal (p=0.017) and parametrial (p<0.001) extensions were more frequent and advanced disease was more common (p=0.008) in GEA compared to UEA. Distant metastasis occurred more frequently (p=0.042), and the RFS (p=0.039) and OS (p=0.011) were worse in patients with GEA compared to patients with UEA. The mean RFS of patients with GEA (12.2 months) was significantly shorter than that of patients with UEA (22.9 months). Similarly, the mean OS of patients with GEA was significantly worse than that of patients with UEA, at 20.9 months and 42.7 months, respectively. The frequency of lymph node metastasis or post-treatment recurrence did not differ significantly between the GEA and UEA.
Differences in clinicopathological characteristics between gastric-type endocervical adenocarcinoma (GEA) and usual-type endocervical adenocarcinoma (UEA).
Cytological characteristics of GEA. Table III summarizes the baseline characteristics of the 18 cytological samples obtained from 14 GEA patients. Multiple samples were obtained from two patients. Three samples were collected from each patient. Fifteen of the eighteen cytological samples were processed using LBP, whereas the others were prepared using conventional smears. Specimens were collected from the uterine cervix or vagina (9/18, 50.0%), peritoneal fluid or ascites (7/18, 38.9%), lymph nodes (1/18, 5.6%), and cerebrospinal fluid (1/18, 5.6%). The cervicovaginal samples were diagnosed as follows on the basis of the 2015 Bethesda System for Reporting Cervical Cytology (21): EAC (2/9, 22.2%), adenocarcinoma of undetermined significance (2/9, 22.2%), endometrial adenocarcinoma (1/9, 11.1%), endocervical adenocarcinoma in situ (2/9, 22.2%), atypical glandular cells-favor neoplastic (1/9, 11.1%), and atypical glandular cells-not otherwise specified (1/9; 11.1%). All other samples collected from the body fluids and lymph nodes tested positive for malignant cells.
Baseline cytological information of gastric-type endocervical adenocarcinoma.
Difference between the cytological characteristics of GEA and UEA. Table IV summarizes the cytological differences between GEA and UEA. Features such as flat, two-dimensional honeycomb-like cellular sheets (p=0.035), foamy or vacuolated cytoplasm (p<0.001), and vesicular chromatin (p=0.037) were observed more frequently in GEA compared to UEA. Intracytoplasmic neutrophil entrapment, abrupt anisonucleosis, and conspicuous nucleoli were also identified more frequently in GEA compared to UEA, albeit without a statistically significant difference. In contrast, three-dimensional cellular clusters, nuclear hyperchromasia, and peripheral nuclear feathering were more frequent in the UEA group compared to the GEA group (p<0.001, p<0.001, and p=0.014, respectively). Mitotic figures were more frequent in the UEA group than those in the GEA group, but the difference was not statistically significant. Golden-yellow mucin was observed in only one patient with GEA.
Differences in cytological characteristics between gastric-type endocervical adenocarcinoma (GEA) and usual-type endocervical adenocarcinoma (UEA).
Unusual cytological features of GEA. We identified several unusual cytomorphological features of GEA in a few cases, including small cellular clusters (Figure 3A); large, three-dimensional clusters showing cribriform architecture (Figure 3B); acinar formation of pleomorphic tumor cells possessing enlarged, hyperchromatic nuclei (Figure 3C); multinucleation (Figure 3D); and singly dispersed or loosely aggregated signet ring-like tumor cells (Figure 3E and F). Architectural abnormalities, such as cribriform and acinar structure, were observed on the conventional cervicovaginal smears, whereas small cellular clusters and singly dispersed cells, some of which resembled signet ring cells, were identified on the LBP slides.

Unusual cytological features of gastric-type endocervical adenocarcinoma. (A) Small cellular clusters and single cells (inset). (B) Cribriform structure. (C and D) Pleomorphic and hyperchromatic tumor cells forming an acinar structure (yellow arrows) or multinucleated giant cells (green arrows). (E) Signet ring-like cells dispersed singly or arranged in small cellular clusters (blue arrows). (F) Signet ring-like cells (white arrows). A-F, Papanicolaou staining. Original magnification: A, 400×; B, 100×; C, 60×; D, 100×; E, 60×; F, 400×. The scale bar is shown in the lower right corner of each panel.
Discussion
In this study, we analyzed the clinicopathological differences between GEA and UEA. GEA was characterized by a more advanced initial stage and higher frequencies of vaginal extension, parametrial extension, and distant metastasis compared to UEA. These results are consistent with the previous data, which demonstrated deeper invasion, greater horizontal spread, more advanced disease stage, more frequent vaginal and parametrial involvement, and distant metastasis in GEA compared to UEA (2). Similarly, Park et al. (1) observed higher rates of vaginal involvement and parametrial invasion and more advanced stage-disease in GEA compared to UEA. Karamurzin et al. (22) reported that GEA represents a biologically aggressive subtype of EAC that occurs at a more advanced stage compared to UEA. Previous studies have shown that GEA has a high propensity for lymph node metastasis. Nishio et al. (23) conducted a multi-institutional study, which found that GEA was more significantly associated with lymphovascular invasion and lymph node metastasis than UEA. Nakamura et al. (24) also showed that GEA patients developed lymph node metastasis more frequently than those with other EACs. However, in this study, the frequencies of lymph node metastasis and post-treatment recurrence did not differ significantly between GEA and UEA. The difference in statistical significance between the current and previous results may be attributed to differences in the sample size, stage distribution, treatment modalities, and postoperative follow-up period among studies. Nevertheless, the higher frequency of both local extension and metastasis in GEA observed in this study indicate that GEA is more aggressive than UEA.
We also demonstrated the differences in patient outcomes between GEA and UEA. We found that survival was significantly worse in patients with GEA than that in patients with UEA. The mean respective OS and DFS of patients with GEA were 20.9 months and 12.2 months, which were significantly shorter than those of patients with UEA (42.7 months and 22.9 months, respectively). Several previous studies have reported consistent results concurrent with our findings, i.e., the patient outcomes were worse with GEA. In the most recent study by Ehmann et al. (25), the median progression-free survival and OS for patients with stage II-IV GEA were 17 months and 33 months, respectively, compared to 107 months and 111 months for those with stage I tumors, respectively. Nishio et al. (23) observed that the DFS and OS were worse in patients with GEA than those in patients with UEA. In their subsequent study, the prognosis of GEA was confirmed to be poor, even in cases of early-stage disease and after surgical resection (26). Karamurzin et al. (22) also reported that at initial presentation, 59% of patients with GEA presented with an advanced stage, 50% had lymph node metastases, 35% had ovarian involvement, and 20% had abdominal metastases. The five-year DFS rate was 42% for GEA versus 91% for UEA. Overall, GEA exhibited aggressive behavior and resulted in poor outcomes. A more advanced stage at the time of diagnosis and worse survival of patients with GEA further emphasizes the importance of early detection and accurate diagnosis (27).
GEA has not been well recognized in cytological specimens (27). Previous studies have shown that a small subset of GEA may be misdiagnosed as endocervical adenocarcinoma in situ or atypical glandular cells, and negative for intraepithelial lesion or malignancy (18, 28-31). In this study, 44.4% (4/9) of cases were misdiagnosed as endocervical adenocarcinoma in situ, atypical glandular cells-favor neoplastic, or atypical glandular cells-not otherwise specified. These results highlight the importance of understanding the cytological features of GEA for proper diagnosis. Previous studies have described the cytopathological characteristics of GEA. Kawakami et al. (28) reported monolayered, honeycomb-like cellular sheets, vacuolar and foamy cytoplasm, intracytoplasmic neutrophil entrapment, vesicular nuclei, and prominent nucleoli as the characteristic cytological features of GEA. Similarly, Schwock et al. (30) noted that microvesicular cytoplasm, honeycomb-like sheets, prominent nucleoli, and anisonucleosis are the most discriminatory features of GEA. According to a recent study by Yeo et al. (18), monolayered, honeycomb-like sheets and vacuolated granular cytoplasm were observed more frequently in GEA than UEA. We observed that flat, honeycomb-like cell sheets, foamy or vacuolated cytoplasm, vesicular chromatin, and prominent nucleoli occurred more frequently in GEA compared to UEA, consistent with these studies. UEA exhibited three-dimensional clusters, nuclear hyperchromasia, and peripheral nuclear feathering. In contrast, in this study, the frequency of intracytoplasmic neutrophil entrapment and anisonucleosis, both of which were previously reported to be more frequent in GEA, did not differ significantly between GEA and UEA. Yeo et al. (18) noted that golden-brown intracytoplasmic mucin is a discriminatory feature of GEA. Omori et al. (32) also suggested the presence of gastric-type yellow mucin is a diagnostic clue for the cytological diagnosis of GEA. However, we could not determine the diagnostic significance of yellow mucin, which has been suggested to be a diagnostic clue for GEA, since it was present in only one case of GEA in this study. Meanwhile, we found some unusual cytological features of GEA both in LBP and conventional smear slides, including irregular-shaped small cellular clusters, single scattered tumor cells resembling signet-ring cells, and three-dimensional clusters showing cribriform architecture. Additional studies with larger cohorts are required to clarify the clinical significance of these unusual cytomorphologies of GEA.
We comprehensively analyzed the cytological features of GEA. This study has several strengths. We confirmed previous evidence of the clinicopathological and prognostic differences between GEA and UEA. This study is one of the largest case series describing the cytopathological characteristics of GEA and comparing them with those of UEA. We observed that a subset of GEA was misdiagnosed as atypical glandular cells or adenocarcinoma in situ in cytological specimens, which consistently displayed cytological features distinct from those of UEA. We identified significant cytological features to aid in the differential diagnosis of GEA and UEA. This study also has some limitations. First, all specimens were retrieved from a single institution. However, we collected various types of cytological specimens and found no significant differences in the cytological features according to the sampling method or site.
In summary, GEA is a distinct type of EAC with aggressive behavior and poor outcomes. Accurate diagnosis of GEA during cytological screening is important because it is usually diagnosed at an advanced stage and associated with a shorter survival rate than the other histological types. In this study, we demonstrated several distinct cytological features of GEA, including flat, honeycomb-like cellular sheets, foamy or vacuolated cytoplasm, vesicular chromatin, and prominent nucleoli.
Footnotes
Authors’ Contributions
All Authors made substantial contributions to the conceptualization and methodological design of this study; the acquisition, validation, analysis, investigation, and curation of the data; writing of the original draft; critical review, commentary, and revision of the article for important intellectual content; project administration; and the final approval of the version to be published.
Conflicts of Interest
The Authors have no conflicts of interest or financial ties to declare with respect to this study.
- Received February 18, 2023.
- Revision received February 28, 2023.
- Accepted March 1, 2023.
- Copyright © 2023, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).





{kind=link}
{kind=link}
{kind=link}