


Abstract
Background/Aim: Establishment of powerful and easy-to-evaluate biomarkers that can predict immune checkpoint inhibitor sensitivity in patients with gastric cancer (GC) would be highly useful. The albumin-derived neutrophil-to-lymphocyte ratio (Alb-dNLR) score reportedly is an excellent measure of both immunity and nutritional status. However, the association between nivolumab treatment sensitivity and Alb-dNLR in GC has also not been adequately investigated. This multicenter retrospective study was designed to evaluate the association of Alb-dNLR with therapeutic sensitivity of nivolumab in GC patients. Patients and Methods: This was a retrospective multicenter study with patients from five sites. The data from 58 patients who received nivolumab for postoperative recurrent or unresectable advanced GC between October 2017 and December 2018 were analyzed. Blood tests had been performed before nivolumab administration. We analyzed the correlation between the Alb-dNLR score and clinicopathological factors, including best overall response. Results: Of the 58 patients, 21 (36.2%) comprised the disease control (DC) group and 37 (63.8%) comprised the progressive disease (PD) group. The nivolumab treatment responses were subjected to receiver operating characteristic analysis. The cutoff value was set to 2.90 g/dl for Alb and to 3.55 for dNLR. All eight patients in the high Alb-dNLR group had PD (p=0.0049). The low Alb-dNLR group had significantly better overall survival (p=0.0023) and progression-free survival rates (p<0.0001). Conclusion: The Alb-dNLR score was a very simple and sensitive predictor of nivolumab therapeutic sensitivity and has very good biomarker properties.
Gastric cancer (GC) is the fifth most common cancer in the world, the third leading cause of cancer death, and has the highest incidence in East Asia (1). Systemic therapy can provide symptomatic relief, improved survival, and better quality of life in patients with locally advanced or metastatic GC. Although the prognosis of GC has gradually improved with better surgery, chemotherapy, and immune checkpoint inhibitors (ICIs), it is still not good enough.
Regarding ICIs, the ATTRACTION-2 trial showed that nivolumab, an anti-programmed cell death protein 1 (PD-1) antibody, improved overall survival (OS) in GC patients who received at least two prior regimens of chemotherapy (2). Furthermore, the CheckMate 649 study revealed that nivolumab plus chemotherapy was recommended as first-line therapy for GC (3). Thus, the importance of ICIs in the treatment of GC has increased dramatically. However, the response rate to ICIs in GC patients is unsatisfactory, and the ATTRACTION-2 trial reported a response rate of 11.2% in the nivolumab group versus 0% in the placebo group (2). There is also concern that expensive ICIs will have a negative impact on the health care economy. Therefore, it is highly desirable to establish powerful and easy-to-evaluate biomarkers that can predict ICI sensitivity in GC patients.
We previously reported the efficacy of the GRIm-score (4) and serum lactate dehydrogenase (LDH) to albumin (Alb) ratio as biomarkers for predicting treatment sensitivity in patients with GC using nivolumab (5, 6). Sato et al. reported that low C-reactive protein level, immune-related adverse events, high albumin level, high lymphocyte count, and differentiated histological type may affect outcomes (7). In addition, several reports have also reported that CD8 and the tumor mutation burden could be biomarkers for patients with GC using ICIs (8, 9). However, biomarker identification from a pathological perspective also has the problem of heterogeneous expression within the tumor (10). In addition, it is expected that establishment of biomarkers that can be easily and objectively evaluated in daily medical practice can be achieved.
The derived neutrophil-to-lymphocyte ratio (dNLR) was reported as a simpler measure than NLR, which is calculated from the total white blood cell count and neutrophil count. Reportedly, dNLR is a prognostic biomarker for a variety of cancers (11). In GC, preoperative dNLR has been reported to be a useful prognostic indicator or biomarker of PD-1 antibody sensitivity (12-14). The albumin-dNLR (Alb-dNLR) score has been reported as an excellent measure of both immunity and nutritional status (11). This score is said to reflect the activity of rheumatoid arthritis (15) or to be associated with extremely useful parameters predictive of OS for esophageal squamous cell carcinoma patients (16). However, to the best of our knowledge, there are no reports of an association between GC and Alb-dNLR. The association between nivolumab treatment sensitivity and Alb-dNLR in GC also has not been adequately investigated.
We hypothesized that Alb-dNLR, which can evaluate both nutrition and immunity, might be a biomarker that can easily predict the sensitivity to nivolumab treatment in GC. The study aimed to examine the ability of the Alb-dNLR score as a biomarker for predicting the sensitivity to nivolumab treatment in patients who participated in a multicenter study.
Patients and Methods
Patients. This was a retrospective multicenter study in patients from five participating sites (Gunma University Hospital, Gunma Prefectural Cancer Center, National Hospital Organization Takasaki General Medical Center, Isesaki Municipal Hospital, and the Japan Community Healthcare Organization Gunma Central). The data from 58 patients who received nivolumab for postoperative recurrent or unresectable advanced GC between October 2017 and December 2018 were analyzed (17). Nivolumab was administered every 2 weeks. We evaluated the best overall response to nivolumab using the Response Evaluation Criteria in Solid Tumors guidelines, version 1.1 (18), computed tomography scans, and the patients’ general state of physical condition after starting nivolumab treatment. We collected the following data: sex, age, Eastern Cooperative Oncology Group Performance Status (ECOG-PS), postoperative recurrence, Lauren classification, frequency of previous regimens, and the number of metastatic organs. Patients were classified into two groups: the progressive disease (PD) and disease control (DC) groups. The Institutional Review Board of Gunma University approved this study (approval no. HS2018-237).
Assessment of the laboratory test results. Before nivolumab treatment in patients with GC, we collected the following laboratory test results: white blood cell count, neutrophil count, dNLR, hemoglobin, platelets, total protein, Alb, total bilirubin, aspartate aminotransferase (AST), alanine aminotransferase (ALT), LDH, blood urea nitrogen, creatinine, and C-reactive protein (CRP). The following calculation was used to determine the dNLR:
dNLR=neutrophil count/(white blood cell count - neutrophil count) (11).
Assessment of the Alb-dNLR score. The cutoff values for Alb and dNLR were determined by receiver operating characteristics (ROC) analysis (19). Three groups were classified according to the following Alb-dNLR scores: 2, patients with both low albumin and high dNLR; 1, patients with either abnormality; and 0, patients with high albumin and low dNLR (15). Patients with a score of 2 were designated as the “high Alb-dNLR score group” and those with scores of 0 or 1 as the “low Alb-dNLR score group”.
Statistical analysis. The statistical significance of differences was assessed using the Mann-Whitney U-test for continuous variables and the chi-square test for categorical variables. The optimal cutoff values of the alb-dNLR were determined from the ROC curves. OS and progression-free survival (PFS) rates were analyzed using the Kaplan-Meier method, and the statistical significance of differences was assessed using the log-rank test. The level of statistical significance was set to p<0.05. All analyses were performed using JMP Pro (version 12.0; SAS Institute Inc., Cary, NC, USA).
Results
Patients. The results are shown in Table I. There were 21 (36.2%) patients in the DC group and 37 (63.8%) in the PD group. There was no significant difference in age between the two groups, but significantly more patients in the DC group had an ECOG-PS of 0 (p=0.021). There was a significant correlation between PS and nivolumab response, and there were no significant differences in the presence of postoperative recurrence, Lauren classification, and frequency of previous regimens between the two groups.
Patient characteristics.
Assessment of the laboratory test results. No significant differences in the white blood cell count, hemoglobin, platelets, total protein, total bilirubin, AST, ALT, LDH, blood urea nitrogen, and creatinine were found between the two groups before nivolumab treatment in the patients with GC (Table II). Of the factors evaluated in this study, a low CRP level prior to nivolumab treatment was the only one significantly associated with therapeutic response (p=0.013) (5). The dNLR was 2.11±0.28 for the DC group and 2.72±0.21 for the PD group (p=0.09). The Alb level was 3.24±0.13 in the DC group and 3.22±0.09 in the PD group (p=0.92).
Assessment of the laboratory test results before nivolumab administration.
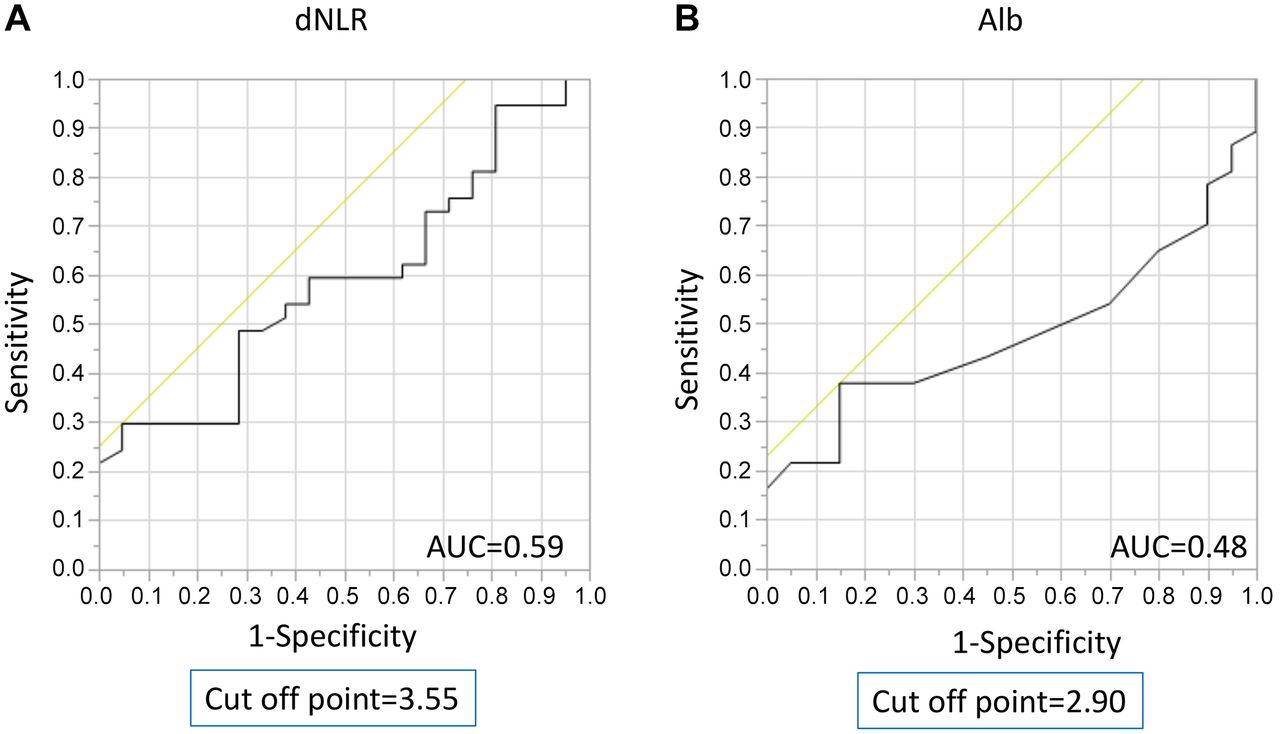
Assessment of the Alb-dNLR score. We performed a ROC analysis of nivolumab treatment response. On the basis of the ROC analysis, the cutoff value of Alb was 2.90 g/dl, and the area under the curve (AUC) was 0.48 for the treatment response (Figure 1A). On the other hand, the cutoff value of dNLR was 3.55, and the AUC was 0.59 (Figure 1B). As mentioned above, we divided the patients into two groups on the basis of the Alb-dNLR score (2=the high Alb-dNLR score group vs. 0 or 1=the low Alb-dNLR score group).

Receiver operating characteristic analysis of derived neutrophil-to-lymphocyte ratio (dNLR) and serum albumin (Alb) for nivolumab treatment response. (A) The cutoff value of dNLR was 3.55, and the area under the curve (AUC) value was 0.59. (B) The cutoff value of Alb was 2.90 g/dl, and the AUC value was 0.48.
Correlations between the Alb-dNLR score and sensitivity to nivolumab. There were 8 (13.8%) patients in the high-score group and 50 (86.2%) in the low-score group (Table III). Age, sex, PS, Lauren classification, presence of postoperative recurrence, and the number of metastatic organs showed no significant associations between the two groups. All eight patients in the high group had PD (p=0.0049). Kaplan-Meier curves of OS and PFS between the patients with high and low scores are shown in Figure 2. The low-score group had significantly better OS (p=0.0023) and PFS (p<0.0001).
Association between albumin-derived neutrophil-to-lymphocyte and clinicopathological data.

Kaplan-Meier curve according to the albumin-derived neutrophil-to-lymphocyte ratio (Alb-dNLR) score before nivolumab treatment. (A) Overall survival. (B) Progression-free survival.
Discussion
This is the first study on Alb-dNLR in patients with GC treated with nivolumab. We performed a ROC analysis of nivolumab treatment response and set the cutoff value of Alb to 2.90 g/dl and that of dNLR to 3.55. All eight patients in the high Alb-dNLR group had PD. The low Alb-dNLR group had significantly better OS and PFS.
The concept of dNLR was previously reported by Proctor et al. (11). The NLR is calculated as the ratio of the neutrophil count to the lymphocytes count, whereas the dNLR does not require lymphocytes and can be easily calculated from the total white blood cell count and neutrophil count. This means that dNLR is simpler and more convenient to use. Furthermore, the concept of Alb-dNLR, in which Alb is added to the dNLR, has been reported to be a simple indicator for assessing both immunity and nutritional status (11). Because it reflects both immunity and nutritional status, the Alb-dNLR score correlates with nivolumab treatment sensitivity in patients with GC using nivolumab.
Of the 58 patients included in this study, 48 were able to receive at least two courses of nivolumab. The data showing whether dNLR and Alb increased or decreased after two courses of nivolumab in those 48 patients compared with those before treatment are shown in Table IV. In the PR+SD group, dNLR increased and Alb decreased or remained unchanged in 4 (21.1%) patients, whereas in the PD group, dNLR increased and Alb decreased or remained unchanged in 17 (58.6%) patients. On the other hand, there were six patients in the PR+SD group in which dNLR decreased or remained unchanged and Alb increased (31.6%), compared with one (3.4%) patient in the PD group (p=0.0047). These results suggest that the dNLR and Alb trends during nivolumab treatment may serve as a useful biomarker for predicting treatment sensitivity at an earlier stage.
Change in Alb levels and dNLR before and after two courses of nivolumab in 48 patients.
There have been several reports on the sensitivity of dNLR and ICIs in the treatment of non-small-cell lung cancer (NSCLC), and high dNLR levels are thought to reflect treatment resistance (20-23). Furthermore, there are reports that in patients with advanced melanoma using nivolumab, baseline NLR and dNLR were significant predictors of therapeutic resistance (24). JV Alessi et al. showed that in advanced NSCLC samples with a PD-L1 tumor promotion score >50%, samples with a dNLR score <2.6 have significantly higher numbers of tumor-associated CD8+, FOXP3+, PD-1+ immune cells, and PD-1 +CD8+ T cells than samples with dNLR ≥2.6 (25). Good responses to ICIs are strongly correlated with intratumoral CD8+ T-cell expression in cancer stroma, and such tumors are called hot tumors with antitumor immunity (26, 27). For this reason, the dNLR and ICI resistance to treatment were significantly associated. In this study, we examined for the first time the relationship between dNLR and therapeutic sensitivity in patients with GC treated with nivolumab, and dNLR was found to be a highly significant predictive biomarker.
Our study had some limitations. First, although this was a multicenter study, the number of patients was relatively small. Second, the cutoff values for Alb and dNLR can vary depending on the subjects under consideration. Therefore, further studies are warranted to increase the significance of Alb-dNLR as a biomarker of nivolumab therapeutic sensitivity. With the approval of nivolumab for first-line treatment in GC, its importance in overall treatment has increased greatly. As a next step, we would like to further investigate the significance of Alb-dNLR as a biomarker in patients who use nivolumab in primary therapy.
In conclusion, this study was the first to characterize Alb-dNLR as a biomarker of therapeutic sensitivity in patients with GC treated with nivolumab after third-line therapy. The Alb-dNLR score used in this study was found to be a very simple and sensitive predictor of nivolumab therapeutic sensitivity and was considered to have very good biomarker properties.
Acknowledgements
The Authors thank Ms. Harumi Kanai for her excellent assistance.
Footnotes
Authors’ Contributions
Conception and design: Nobuhiro Nakazawa, Akiharu Kimura, Norimichi Kogure, Hisashi Hosaka, Atsushi Naganuma, Masanori Sekiguchi, Kana Saito, Kyoichi Ogata, Akihiko Sano, Ken Shirabe, and Hiroshi Saeki; Acquisition of data: Nobuhiro Nakazawa, Hisashi Hosaka, Atsushi Naganuma, Masanori Sekiguchi, Kana Saito, and Akihiko Sano; Analysis and interpretation: Nobuhiro Nakazawa, Makoto Sohda, Kohei Tateno, Takayoshi Watanabe, Akihiko Sano, Makoto Sakai, Hiroomi Ogawa, Ken Shirabe, and Hiroshi Saeki; Writing, review, and/or revision of the manuscript: Nobuhiro Nakazawa, Makoto Sohda, Akihiko Sano, Ken Shirabe, and Hiroshi Saeki. Nobuhiro Nakazawa, Makoto Sohda, Kohei Tateno, Takayoshi Watanabe, Akiharu Kimura, Norimichi Kogure, Hisashi Hosaka, Atsushi Naganuma, Masanori Sekiguchi, Kana Saito, Kyoichi Ogata, Akihiko Sano, Makoto Sakai, Hiroomi Ogawa, Ken Shirabe, and Hiroshi Saeki have read and approved the final manuscript.
Conflicts of Interest
The Authors declare that they have no conflicts of interest in relation to this study.
- Received December 7, 2022.
- Revision received December 23, 2022.
- Accepted January 9, 2023.
- Copyright © 2023, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.