


Abstract
Background/Aim: Triple arthrodesis (TA) is a common procedure for stabilization of painful and unstable hind foot deformities. The aim of the study was to analyze postoperative changes in function and pain following isolated TA based on clinical outcomes, radiological findings, and pain scores. The study also considered economic aspects, such as the inability to work, before and after surgery. Patients and Methods: This was a single-center retrospective study, with a mean follow-up of 7.8 (range=2.9-12.6) years, of isolated triple fusions was performed. Short-Form 36 (SF-36), Foot Function Index (FFI), American Orthopedic Foot and Ankle Society Score (AOFAS) were analyzed. Clinical examination and standardized radiographs pre- and post-surgery were evaluated. Results: All 16 patients were very satisfied with the outcome after TA. In patients with secondary arthrosis of the ankle joint, AOFAS scores were significantly lower (p=0.012), whereas arthrosis in tarsal and tarsometatarsal joints did not affect the score. Body mass index (BMI) was associated with lower AOFAS, FFI-pain, FFI-function and increased hindfoot valgus. The non-union rate was approximately 11%. Conclusion: TA leads to good clinical and radiological outcomes. None of the study participants reported a deterioration in their quality of life after TA. Two thirds of the patients reported significant limitations when walking on uneven ground. More than half of the feet developed secondary arthrosis of the tarsal joints and 44% of the ankle joint.
Triple arthrodesis (TA) involves fusion of the subtalar and Chopart joints and is a common procedure for stabilization of painful and unstable hind foot deformities. The aim of the procedure is to reduce pain, achieve a stable, plantigrade foot position capable of full weight-bearing and correct deformity, without reducing the range-of-motion (ROM) of the ankle joint (1). Mid- to long-term clinical and radiological results from isolated TA are rare. The first TA was introduced by Hoke in 1921, but the fundamental features of the contemporary operation trace back to Ryerson in 1923 (2, 3). During the last century, the surgical technique underwent further modifications (2-4). TA is indicated for correction of several deformities and conditions of the hindfoot such as neuromuscular diseases, e.g. poliomyelitis or Charcot-Marie-Tooth syndrome, congenital clubfoot, contract acquired pes planovalgus, rheumatoid diseases, arthrosis and posttraumatic deformities (1). There are several contraindications for the procedure. Absolute contraindications include general surgical and anesthetic risks, acute or chronic infections, critical soft tissue conditions, severe peripheral arterial occlusive disease and destructive Charcot arthropathy (5). TA is also contraindicated in advanced arthrosis of adjacent joints, such as the ankle joint, the naviculo-cuneiform and the tarsometatarsal joints (4). Ultimately, the decision is up to the treating physician. The elimination of hindfoot motion increases stress shielding in the ankle joint, the naviculo-cuneiform and the tarsometatarsal joints. Therefore, degenerative changes in these joints may generate painful symptoms over time due to the lack of tarsal mobility (6). Non-union may occur through reduced blood supply and insufficiently stable fixation at the time of attempted arthrodesis. Nicotine abuse and obesity were mentioned as risk factors for non-union in the literature (7-9).
The aim of this study was to analyze postoperative changes in function and pain following isolated TA based on clinical outcomes, radiological findings, and pain scores. The study also considered economic aspects, such as the inability to work, before and after surgery.
Patients and Methods
This retrospective clinical and radiological single-center study was performed with the approval of the local Ethics and Research Committee (No. 8285). All mature patients who underwent an isolated TA at our level 1 trauma center, between 2008 and 2017, were included. Non-operative treatment, such as physical therapy, shoe modification and analgesia were exhausted before surgery was indicated. Surgery was performed by senior foot and ankle surgeons. Minimum follow-up was two years. Patient recruitment, exclusion criteria and the composition of the study participants are shown in Figure 1.
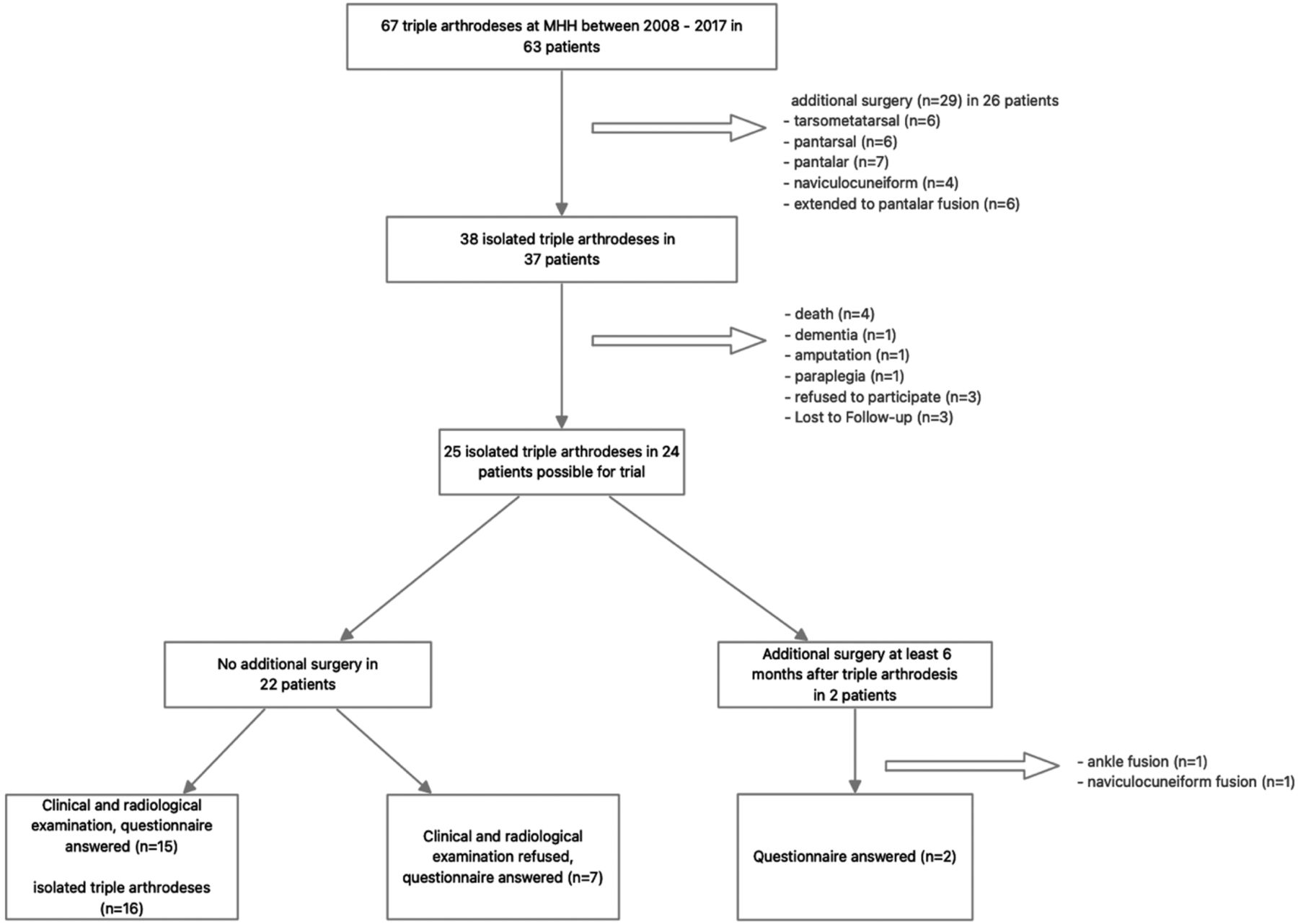
Study participation flowchart.
Patients with bilateral isolated TA were excluded from comparisons between treated and untreated feet. Patients who underwent ankle or tarsal fusion by secondary surgery, answered the symptoms questionnaires by recalling their symptoms before the additional surgery. They were excluded for clinical and radiological follow-up examination.
The following questionnaires for quality-of-life and function were used: Foot Function Index, which includes FFI-pain from 0 points for best and 72 points for worst results and FFI-function from 0 points for best and 90 points for worst results (10). American Orthopedic Foot and Ankle Society Score (AOFAS) contains three categories: pain (40 points), alignment (10 points) and function (50 points). Missing hindfoot mobility after TA leads to a maximum of 44 instead of 50 points for function. Thus 94 points means the best result and 0 points the worst (4, 11). Hannover score was used which contains 20 points for the best and 100 points for the worst outcome (12). Quality-of-life was evaluated using SF-36 (13, 14).
The patients were asked about the total number and frequency of physiotherapy after surgery and how long they were unable to work, before and after surgery. The degree of disability and reduction in earning capacity was noted. The patients were asked how they rated the change in quality-of-life after surgery, from significant deterioration, deterioration, unchanged, improvement to significant improvement.
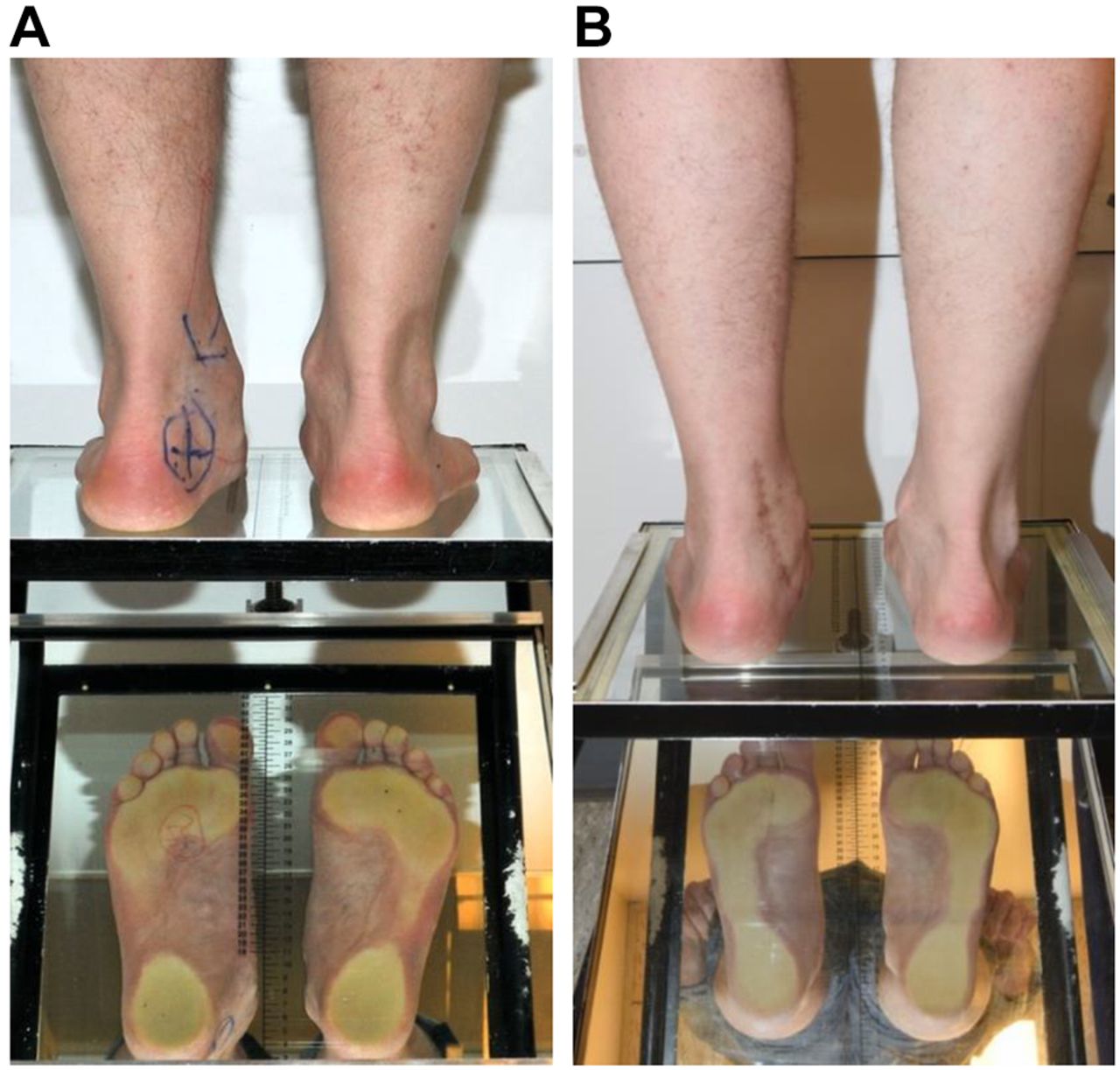
A mirror-table was used for semi-quantitative measuring of the weight-bearing area of the plantar aspect of the foot (Figure 2). ROM of the ankle, naviculo-cuneiform- and Lisfranc joints were measured with a goniometer on both sides. Muscle strength at the lower leg was evaluated by the Oxford scale. To evaluate pain, we used the Visual Analog Scale (VAS) from 0 points (no pain) to 10 points (worst pain imaginable). Radiographs were performed via dorsoplantar and lateral view of the foot whilst weight-bearing, an oblique view of the foot, and anterior-posterior and lateral views of the ankle joint. These were compared to pre-operative radiographs with a focus on progression of arthrosis of the ankle or tarsal joints. To detect evidence of non-union, radiographs at follow-up were used. The grade of arthrosis was evaluated using the Kellgren-Lawrence score (KLS) pre- and postoperatively (15, 16). All patients were scored twice in randomized order. We defined arthrosis as a KLS grade of two or higher (Table I). Based on the radiographs, 3 angles were measured preoperatively and at follow-up (Figure 3).

Patient standing on mirror-table. (A) Preoperatively. (B) At follow-up (3 years after TA). Left foot with TA. TA: Triple arthrodesis.
Kellgren-Lawrence score.
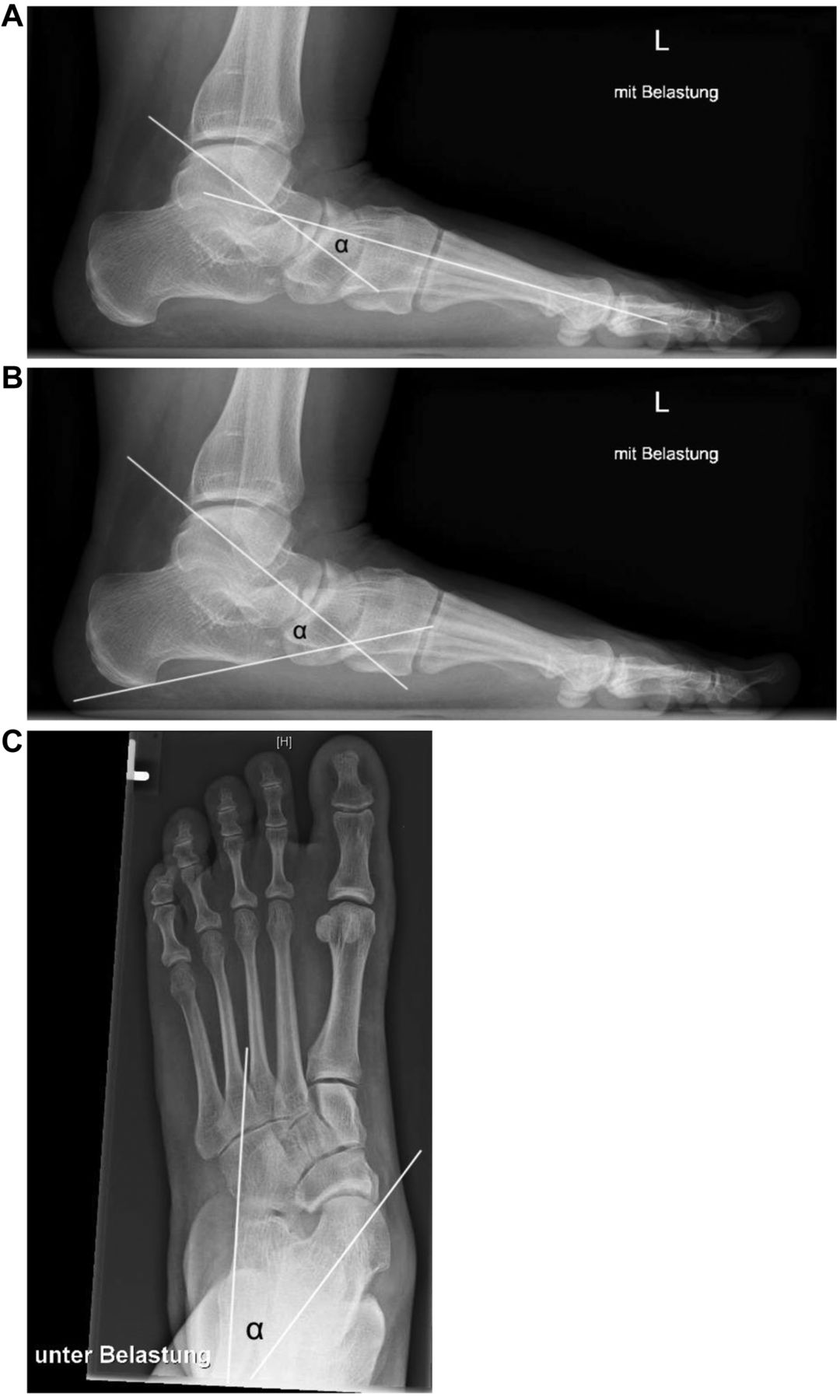
Measured angles based on radiographs. (A) Talometatarsal angle in lateral view. (B) Talocalcaneal angle in lateral view. (C) Talocalcaneal angle in dorsoplantar view.
Statistical analysis. The statistical software IBM SPSS Statistics 26.0 (IBM Corp., Armonk, NY, USA) was used to analyze the current data. To compare the risk factors nicotine abuse and obesity (>30 kg/m2) for non-union, a cross table with Chi-Quadrat-Fisher’s test was used. Depending on the parameter the impact of sex, age, obesity, and arthrosis were examined by means of t-test and bivariate correlation. Statistically significance was assumed at p<0.05.
Results
Patient details. Radiographs of 16 feet (15 patients), taken at the time of clinical examination, and 24 questionnaires were available for evaluation. From the 2 patients with secondary surgery, radiographs before TA and the revision were available for evaluation. Consequently 18 feet of 17 patients, with complete sets of radiographs before and after TA, were included. Fifteen patients (16 feet) were examined clinically and AOFAS were evaluated.
The mean follow-up time was 7.8 (range=2.9-12.6) years. Twenty-four (7 male/17 female) patients were evaluated. The mean age at surgery was 50 (range=16-84) years. The overall mean body mass index (BMI) at surgery was 30.5 (range=18.6-46.1, 95% CI=27.8-33.3) kg/m2. The difference between sexes was not significant (p=0.576). At the time of surgery, 2 patients suffered from diabetes, 4 were smokers or suffered from depression and rheumatoid arthritis. Two of 18 feet developed a non-union (11%) in two different patients. Both were obese, 1 of these was a smoker and neither suffered from diabetes. Of the 16 patients with healed fusions, 7 were obese, 3 were smokers and 2 suffered from diabetes. Indications for TA are shown in Table II.
Indications for TA.
Patient outcome scores and questionnaires. The mean AOFAS value of 16 feet was 65 (range=20-93, 95% CI=53.4-77.3). In patients with increasing arthrosis of the ankle joint (n=7) mean AOFAS was significantly lower than in patients without (n=9) increasing ankle arthrosis (50 vs. 77, p=0.012). However, the values between the groups with (n=8) and without (n=8) increasing arthrosis of the tarsal and tarsometatarsal joints were not significantly different (58 vs. 72, p=0.227). In patients older than 65 years the mean value for AOFAS was tendentially, but not significantly lower (52 vs. 73, p=0.071).
The mean VAS score for pain at follow-up was 4.5 (range=0-9, 95% CI=2.9-6.2). The average SF-36 value was 57 (range=17-99, 95% CI=46.1-67.2). The mean physical component score in SF-36 was 53 (range=20-99, 95% CI=41.7-64.3) and the mean mental component score was 60 (range=13-99, 95% CI=49.4-71).
The mean FFI was 22 (range=0-50, 95% CI=14.7-28.4) for pain and 39 (range=3-85, 95% CI=28.2-50) for function. The mean value for Hannover Score was 55 (range=26-82, 95% CI=47.7-63). Arthrosis in the adjacent joints did not significantly affect the clinical results or pain after TA. Patients with increasing arthrosis in the adjacent joints had a significant (p=0.004) longer follow-up of 9.3 (range=3.6-12.6) years compared to those without increasing arthrosis, follow-up 4.6 (range=2.9-7.9) years.
While more than one third (9 patients) reported a pain free walking distance less than 500 meter (m), 15 patients were able to walk more than 500 m without pain. When walking on uneven ground, a quarter (6 patients) reported having no limitations, two thirds had significant limitations (16 patients) and 2 were unable to do so. Five out of 24 patient were absolutely pain free, 6 patients suffered from pain occasionally and half of the patients had moderate pain. One patient after bilateral TA, suffered from persistent, severe pain in both feet, and showed moderate to severe arthrosis in the adjacent joints on both sides associated with an increased hindfoot valgus of 15° and 20°, respectively. Both patients who underwent further surgery reported an improvement of quality-of-life after TA. One of them was initially completely pain free, the other one reported a reduction in pain-level. However, both developed symptomatic arthrosis and required secondary surgery after 8 and 21 months respectively. Six out of 15 patients reported a significant improvement in quality-of-life after TA, 7 reported an improvement and in 2 pain remained unchanged. None of them got worse.
Personal impact factors for outcome scores. Sex was detected as a parameter for clinical outcome. Males showed significantly better results for SF-36 (73 vs. 50, 95% CI=2.1-44.9, p=0.033), FFI-function (22 vs. 48, 95% CI=−48-−3.9, p=0.023) and Hannover Score (44 vs. 61, 95% CI=−32.5-−1, p=0.038). No significant differences were found between sexes in the FFI-pain, VAS score or AOFAS. Age at surgery was detected to be significantly correlated with clinical outcome scores in FFI-function (Pearson correlation 0.41, p=0.042), SF-36 (Pearson correlation −0.544, p=0.005) and Hannover Score (Pearson correlation 0.548, p=0.005). However, BMI was found to influence outcome parameters significantly: AOFAS (Pearson correlation −0.738, p=0.001), FFI-pain (Pearson correlation 0.637, p=0.008) and FFI-function (Pearson correlation 0.688, p=0.003).
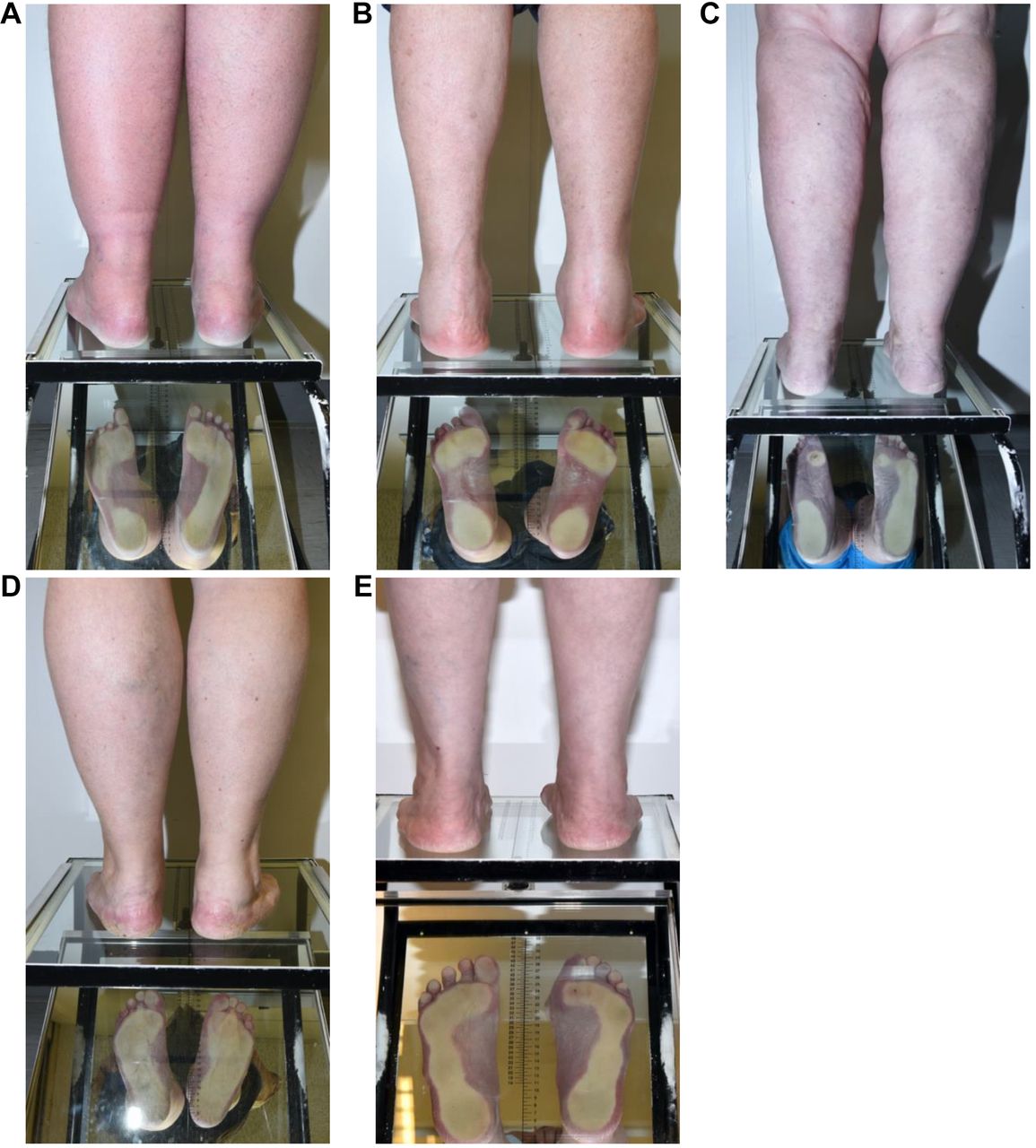
Weight-bearing analysis. Observing the back of both feet under weight-bearing, an obliteration of the paraachillary pits by soft tissue swelling was seen in 9 out of 16 treated feet. Figure 2 shows the status on mirror-table pre- to postoperatively. Figure 4 presents different weight-bearing patterns. In 8 out of 16 feet callosities were seen, which were mostly located plantar to the metatarsal heads.

Patients standing on mirror-table. Different weight-bearing patterns of the foot can be recognized by the pressure distribution of the plantar side of the foot. (A) Forefoot loading with pes equinus (left). (B) Pes cavus (both sides). (C) Sole heel load with pes calcaneus (left). (D) Overloading the medial edge of the foot with hindfoot valgus (left). (E) Overloading the lateral edge of the foot with straight hindfoot axis (both sides).
The mean hindfoot axis was 4° valgus (range=0°-15°, 95%CI=1-6.5) for the treated and 7° valgus (range=0°-10°, 95%CI=4.6-8.4) for the untreated feet, which was significantly different (p=0.049). The patient with bilateral TA was excluded from the evaluation of this parameter. Only 1 patient showed a bilateral hindfoot varus of 5°. Five patients showed a straight axis at the treated feet. In 6 feet a slight (0°-5°), in 1 foot a moderate (6°-10°) and in 3 feet a severe (>10°) hindfoot valgus was seen. A higher hindfoot valgus was significantly correlated with FFI-pain (Pearson correlation 0.541, p=0.031), but not with FFI-function (Pearson correlation 0.441, p=0.087). Obesity was correlated with hindfoot valgus (Pearson correlation 0.621, p=0.01).
Functional examination. The mean extension and flexion of the ankle joint at the treated side was 43° (range=30°-60°, 95% CI=37.2-49.3). At the untreated side the mean ROM was 48° (range=20°-65°, 95% CI=41.7-54.8). This difference was not significant (p=0.2). Extension and flexion of Lisfranc and naviculo-cuneiform joints was significantly lower at the treated side with 21° (range=0°-45°, 95% CI=15.1-27.1) compared to 46° (range=5°-70°, 95% CI=34.7-58.2) at the untreated side (p=0.001). The patient with bilateral TA was excluded from this sub-analysis.
The mean overall postoperative KLS (mean value ≥2) in the ankle joint was significantly correlated with a decreased ROM (Pearson correlation −0.835, p=0.039) but not with the ROM of naviculo-cuneiform and Lisfranc joints (Pearson correlation −0.699, p=0.122). Passive translatorial forces caused pain in 2 naviculo-cuneiform joints and in 1 first and fifth tarsometatarsal joint each. In those, arthrosis was found radiologically in 1 naviculo-cuneiform and fifth tarsometatarsal joint each. However, in the two patients with a non-union, pain was absent under translation forces. Because of complains implant removal was performed in 4 feet. Half of the treated feet (n=8) exhibited full strength in all tested muscles (5/5). In cases of reduced strength, flexors (30%) were more often weaker than extensors (21%). Muscle atrophy at the dorsal side of the lower leg was detected in more than half of the patients (n=9). For 3 patients, barefoot walking was not possible. Normal gait was found in 6 patients. However, significantly limping was only seen in 1 patient, whereas in 8 patients a slightly form of limping was observed.
Six patients were able to stand on one leg, while 8 patients experienced difficulties doing same. One patient was unable to stand on one leg. Orthopedic shoes were used by 4 patients and insoles by 3 patients. A combination of both was used by 2 patients. The remaining 6 patients walked in normal shoes.
Radiographic analysis. From 18 sets of radiographs available for examination non-union was detected in 2 (11%) feet. 1 non-union was seen in the talonavicular joint and the other in the calcaneocuboid joint. Subtalar joints healed in all patients.
Preoperatively in two thirds of the examined feet, arthrosis was mostly found in the talonavicular joint. Degenerative changes in the subtalar and calcaneocuboidal joints were seen in 11 and 8 feet respectively. Table III shows the incidence and progression of arthrosis from the preoperative status to follow-up. At follow-up we found arthrosis in at least one of the adjacent joints in 13 out of 18 feet (72%). The average degree of correction for the lateral talometatarsal angle was 6° (range=−20°-22°, 95% CI=0.9-10.9) and for the talocalcaneal angles in lateral and dorsoplantar view the average amount of correction was 10° (range=−2°-19°, 95% CI=6.7-12.8) and 2° (range=−17°-10°, 95% CI=−2.1-6.5), respectively. We found no association between the amount of correction and the patient outcome rated by AOFAS, Hannover Score, SF-36, and VAS. Table IV compares the measured angles before and after surgery. Figure 5 shows the radiographs of a patient in progress.
Overview of patients with degenerated related joints pre – and postoperatively with distribution of KLS.
Measured angles based on radiographs preoperatively and at follow-up.

Radiographs from the same patient. (A and C) Preoperatively. (B and D) At follow-up (3 years after TA). TA: Triple arthrodesis.
Economic aspects of TA affecting patients. The mean duration of hospitalization after surgery was 9.2 (range=7-13) days. The mean value of physiotherapy in the ambulant setting after demission from hospital was 69 (range=0-388). Three patients absolved an in-house rehabilitation for a mean duration of 5 (range=3-8) weeks. From the patients being in employment, 2 were unable to work before surgery because of pain and functional limitation. After surgery, 10 patients were on sick leave. The mean unemployability pre-surgery was 5.2 (range=2-8.4) months and post-surgery 9.6 (range=3-34.5) months. At surgery, 25% of patients (n=4) were retired, 2 patients had premature pension and 9 patients pursued a profession. The patient with bilateral TA was an employee during both operations. After surgery 2 patients had changed their profession. Six out of 15 patients had a lower income, thereof 3 patients got a reduction in earning capacity of 100% and 3 got less than 50% of their former income. A total of 6 patients had a degree of disability, 3 of these showed a severe degree of disability of at least 50%. Health insurance was not statistically significant for any outcome parameters.
Discussion
Despite being a standard procedure, outcome data after isolated TA are rare. The aim of the study was to detect postoperative changes in function and pain focused on clinical outcomes, radiological findings, and economic aspects after isolated TA at follow-up of at least 24 months after surgery. To achieve a homogenous group of participants we included only isolated TA.
The mean value of 69 units of physiotherapy until follow-up (some patients still have physiotherapy) points towards the complexity of postoperative treatment. Wapner et al. described a postoperative regime of non-weight-bearing for 6 weeks followed by full weight-bearing in a walking cast for additional 8 to 10 weeks after adequate bone healing (17). De Groot et al. described a similar postoperative procedure of 6 weeks non-weight-bearing, but with subsequent weight-bearing for only 4 to 6 weeks (18). The present study did not find any data in the literature on unemployability after surgery. We found a mean return to work interval of 9.6 months, in our study participants. This implies a longer healing process than the postoperative time of partial weight-bearing described by the mentioned authors above. Patients need to be informed about that they may be unable to work for a longer time.
The non-union rate of 11% in our study is similar to the data in the literature which range from 0% to 36% (2, 4, 19-22). Joveniaux et al. reported complete bone healing in 28 subtalar fusions after an average duration of 13 weeks (25-75 percentile: 12-14) (21). Wilson et al. examined 301 feet with TA. They found higher non-union rates in patients who started weight-bearing between the second to the fifth week compared to patients who started full weight-bearing after 9 weeks (14.8% vs. 2.3%) (23). Angus et al. found that 18 out of 80 feet with non-union continued partial weight-bearing for 3.5 weeks longer than those who achieved bony healing (2).
Due to the retrospective design of our study, we were not able to detect the specific time that weight-bearing was commenced. In some cases, full weight-bearing was delayed because of pain or delayed bony healing which were seen on radiographs at the standard postoperative follow-up encounters. Data on the influence of nicotine abuse and obesity on the non-union rate are heterogeneous in the literature. De Groot et al. found no association between smoking and 18 non-unions in 34 patients with TA (18). While Ishikawa et al. (17 non-unions in 160 feet) and Easley et al. (30 non-unions in 184 feet) found positive correlations of non-union and smoking on hindfoot fusions, Gaedke et al. did not find nicotine-abuse as a risk factor for 11 non-unions in 137 ankle fusions (7, 9, 24). Allport et al. examined the effect of smoking on non-union rates in patients who underwent hindfoot or midfoot arthrodesis. In 381 fusion procedures, the non-union rate was significantly higher in smokers, with a relative risk of 5.81. There was no statistically significant difference between ex-smokers and non-smokers (25).
Suda et al. (12 non-unions in 75 patients) reported no correlation between BMI and the non-union rate in arthrodesis for septic arthritis of the ankle, whereas Collman et al. (5 non-unions in 39 patients) observed a tendency between non-union rate and obese patients (8, 26). Gaedke et al. showed that obesity (BMI >25 kg/m2) is not a significant risk factor. Similarly, Ebalard et al. did not find any correlation with BMI and 5 non-unions in 72 fusions of the subtalar and midtarsal joints (24, 27). We also did not identify obesity and nicotine abuse as significant risk factors for non-union in TA. Akin to Ishikawa et al., we also did not find diabetes having a significant influence to non-union rate (7).
Smith et al. reported that 93% of 26 patients were satisfied with the result of triple fusion. Arthrosis was not correlated to pain and satisfaction (28). Pell et al. did not find any association between satisfaction of the patient and arthrosis in 160 patients with 183 TA, too (29). We also noticed no significant effect of arthrosis on patient satisfaction or VAS scores. Graves et al. reported from 14 (82%) satisfied patients with TA (30). In their 19.5 (range=15-27) months follow-up study, Yang et al. investigated the effect of TA combined with osteotomy in 26 patients with acquired rigid flatfoot. The osteotomy corresponded to a wedge-shaped osteotomy of the subtalar joint, the cuboid bone, and the medial cuneiform bone. Overall satisfaction was described as excellent by 22 (85%), good by 2 (8%) patients and poor by no patient. (31). Figgie et al. identified in 52 (94%) patients with rheumatoid arthritis significant pain relief. Bennett et al. found satisfied patients in 21 of 22 and Czurda et al. in 23 of 24 cases (4, 20, 32). De Groot et al. only found 19 (53%) satisfied patients after TA, but 73% of his patients would agree to the operation again (18). According to other authors, in our study 13 (87%) patients reported at least an improvement after surgery and they would agree to the operation again. Mehta et al. investigated the results of hindfoot and ankle fusions in 42 patients with a follow-up of 12 months after the operation respectively. Of these, 17 patients received subtalar arthrodesis, 10 patients received TA, 8 patients received ankle fusion, and 7 patients received tibiotalocalcaneal arthodesis. In TA, the greatest improvement in physical function and reduction in pain were observed (p=0.01) (33). However, it shows that TA can nevertheless lead to a satisfactory result, although the procedure is technically difficult. These improvements can also be attributed to the satisfaction of our study participants. In our cohort, the mean SF-36 value was 57 with lower values for physical function and better scores in mental health. Smith et al. also reported from higher scores in mental health in patients with TA (28). This phenomenon was also observed by Gaedke et al. and Dalat et al. in patients after ankle fusion (24, 34). This shows that some functionality of the foot is reduced after TA, but the mental health is less affected. We identified statistically significance for lower values in women (p=0.033). In our cohort 3 of 4 participants suffering from depression were female.
The average AOFAS score was 65 in our study cohort at 7.8 (range=2.9-12.6) years of follow-up. This value is comparable with the score of 63 (range=14-94) reported by De Groot et al. at a mean follow-up of 6 (SD=2.5) years (18). Pell et al. found an AOFAS score of 60 (range=0-94) at 5.7 (range=2-10.8) years follow-up (29). Czurda et al. reported a much higher average AOFAS score of 74 in 24 TA at a mean follow- up of 21.5 (range=12-56) months and Knupp et al. reported an average value of 70 in 32 TA in patients with rheumatoid arthritis at a mean follow-up of 5.2 (range=4-7) years (4, 35). Higher scores on the AOFAS were reported by Yang et al. with an improvement from 60.2±7.1 points preoperatively to 89.7±5.5 points at follow-up (31). The differences may be explained by the shorter follow-up period or the coincidence with a rheumatoid arthritis in these studies respectively. Fadle et al. showed in their mean follow-up study of 12.9±3.07 months in 10 TA a statistically significant improvement of the AOFAS score from 66.9±7.69 points preoperatively to 85±5.83 points at follow-up. It should be mentioned that the mean age in this study was 25.10±8.36 years, representing a relatively young cohort (22). Aarts et al. reported that AOFAS score remained stable in their 7.5-year follow-up study (range=6-8) and Klerken et al. did not find significant differences for AOFAS score over time after 15 years post-surgery (6, 36). This means that the clinical outcome at 2 years after TA stays constant up to 15 years. This phenomenon has former been described for results after different orthopedic surgical procedures. In studies with shorter follow-up intervals, Speck et al. reported in 7 TA with a mean follow-up of 52 (range=12-96) months an improvement for AOFAS from 42 points preoperatively to 72 points at follow-up. Barg et al. observed in 11 TA with a mean follow-up of 34 (range=24-48) months a significantly improvement from 40 (range=16-58) to 76,5 (range=58-90) points (5, 37). An improvement of the AOFAS was found in all studies on TA.
At follow-up, the treated feet showed a significantly reduced deviation of the hindfoot axis compared to the untreated contralateral feet. However, 1 patient with bilateral TA suffering from an adipositas per magna (BMI=45,4 kg/m2) and recurrent deviation of hindfoot axis, severe arthrosis in the adjacent joints with chronic severe pain. Nevertheless, the patient reported an improvement in quality-of-life after both operations.
We found an elevated BMI to be correlated with a reduced outcome in AOFAS, FFI-pain and FFI-function and higher values of hindfoot valgus. Results to these impacts are limited. Martins et al. studied the prevalence of foot pain (VAS) and the AOFAS score in 40 severely obese patients (BMI >40 kg/m2) and in 40 volunteers (control group) with an average BMI of 24 kg/m2. The incidence of foot pain was significantly higher in obese patients than in the control group (95% vs. 40%). The AOFAS was significantly lower in the severely obesity group than in the control group (66 vs. 88 points). Martins et al. reported that this finding was consistent with the more frequent reports of posterior calcaneal pain in obese individuals, as well as greater mechanical overload in the midfoot leading to localized pain. Lower AOFAS scores confirm poor functional performance in daily activities, quality-of-life, and movement (38). Whereas Rohlfing et al. could not find any correlation between BMI and AOFAS or VAS in their 66.9 (range=4-186) months follow-up study of 51 patients with ankle arthrolysis (39). Future studies should examine these effects in greater cohorts and to provide more detailed analysis. Increased hindfoot valgus was significantly correlated with higher scores in FFI-pain but did not impair the function significantly. Sixteen (67%) patients had significant difficulties going on uneven ground and two others were not able to do so. This problem is explained by the loss of elevation and invasion of the heel after subtalar and Chopart fusion.
The total rate of secondary arthrosis in the adjacent joints varied from 10% to 77% (4, 18, 29). We found degenerative changes in the tarsal joints and ankle joint in 72%. In the ankle joint arthrosis was seen in 11 out of 18 feet (61%) at follow-up. Aarts et al. observed in 18 (33%) patients an increase of arthrosis in the ankle joint after TA in their 7.5-year follow-up study (36). The current study population showed an increase of arthrosis in the ankle joint in 8 (44%) feet after 7.8 (range=2.9-12.6) years. Smith et al. observed a prevalence of degenerative changes in the ankle joint, the naviculo-cuneiform joints and as well in the tarsometatarsal joints in 12 out of 26 patients (46%) at 14 years follow-up (range=11-18) (28). We detected a similar prevalence for tarsometatarsal arthrosis in 8 out of 18 feet (44%). For arthrosis in the naviculo-cuneiform joints we detected 10 out of 18 feet (56%).
To our knowledge, detailed information about the progression of arthrosis in the naviculo-cuneiform and tarsometatarsal joints following TA does not exist in the literature (KLS change to higher grade of arthrosis or from KLS 0-1 to ≥2). We found progressive arthrosis at the naviculo-cuneiform joints in 7 (39%) and at the tarsometatarsal joints in 8 (44%) feet. In total, progression of arthrosis in at least one of the tarsal and tarsometatarsal joints was found in more than half (56%) of the feet after triple fusion.
Bednarz et al. observed, in 63 feet with TA, an average correction of 12° and 7° in the lateral talometatarsal and talocalcaneal angle, at a mean follow-up of 30 (range=12-30) months, which were in both cases statistically significant (40). Graves et al. found in 18 TA at their mean follow-up of 42 (range=27-156) months, an average amount of correction of 13° for the lateral talometatarsal angle and 12° for the lateral talocalcaneal angle. They did not find any correlation between the correction and the satisfaction of patients (30). Our data are similar. However, measurement of angles on radiograph is very subjective. Nevertheless, we observed a significant improvement at follow-up in the talometatarsal (p=0.023) and talocalcaneal (p<0.001) angles in lateral view. Although our follow-up interval was longer, the improvement of the two angles was still significant. This means a stable fusion of the foot lasts over a longer period of time.
The current study is limited by its retrospective design and the small cohort. The identified correlations should be examined in further studies with larger study cohorts. Due to the study design of including only isolated TA, we had to exclude many patients with additional surgery. Two patients completed the questionnaires retrospectively. Further prospective studies with longer follow-up intervals are required to compare values pre- to postoperatively, using VAS, AOFAS and SF-36. To determine the influence of weight-bearing on the non-union rate, precise documentation of the onset of weight-bearing must be used.
Conclusion
This study characterized postoperative changes in function and pain following isolated TA based on clinical outcomes, radiological findings, and pain scores. In summary, TA leads to good clinical and radiological outcomes. The majority of patients were satisfied with the outcome. Due to the procedure being technically difficult, the long recovery period and the high rate of arthrosis in adjacent joints, a decision to proceed to this surgery should be made after exhausting all conservative treatment options. More than half of the feet developed secondary arthrosis of the tarsal joints and 44% of the ankle joint. Ankle joint arthrosis leads to reduced AOFAS scores, whereas arthrosis in tarsal joints does not affect the AOFAS. The non-union rate for TA is approximately 10%.
Acknowledgements
This study was supported financially by the Trauma-Stiftung Hannover.
Footnotes
Authors’ Contributions
RG and CK designed the study. FM, RG, and UW analyzed and interpreted the clinical data; FM performed statistical analysis. FM, RG, and PO wrote the manuscript. All Authors revised the manuscript critically for important intellectual content and approved its final version.
Conflicts of Interest
The Authors declare no conflicts of interest related to this study.
- Received December 29, 2022.
- Revision received January 22, 2023.
- Accepted February 6, 2023.
- Copyright © 2023, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.