


Abstract
Background/Aim: Vitamin D3 (VD3) affects the regulation of the immune system, including the differentiation and function of regulatory T-cells (Tregs). Tregs play an important role in maintaining immune homeostasis in patients with colorectal cancer (CRC). The effects of VD3 on Treg-associated immune function were investigated in Thai patients in the early stages of CRC. Materials and Methods: Twenty-eight patients were randomized to one of two groups: Untreated or treatment with VD3 for 3 months. Whole blood samples were collected at baseline, and at 1 and 3 months. Peripheral blood mononuclear cells were isolated and the populations of forkhead box P3-positive Treg cells was analyzed by flow cytometry. The levels of Treg-associated cytokines, interleukin 10 (IL-10) and transforming growth factor beta 1 (TGF-β1), were measured by enzyme-linked immunosorbent assays. Results: Serum VD3 levels of the VD3-treated group were significantly increased at 1 (p=0.017) and 3 months (p<0.001) compared to the untreated control group. The mean percentage of Tregs was maintained between 1 and 3 months in the VD3-treated group. At 3 months, the untreated group had significantly lower Treg levels than the VD3-treated group (p=0.043). Serum IL-10 levels of the VD3-treated group were statistically increased at 1 month compared to the control group (p=0.032). No significant difference in serum TGF-β1 levels was observed between the two groups. However, the TGF-β1 level in the VD3-treated group at 1 month was lower than that of the control. Conclusion: Our findings suggest that VD3 supplementation can maintain immune responses in the early stages of CRC, helping to control Treg function. Therefore, VD3 should be supplemented to maintain immune homeostasis, especially in patients with vitamin D deficiency.
The second most common disease in the world, by both incidence and mortality, is colorectal cancer (CRC). It is the fourth most frequently diagnosed cancer in Thailand and is widely found in both men (11.4%) and women (10.7%) (1). Data from the Thai Cancer Registry indicate that the prevalence of CRC is rising nationwide, with average annual percent changes for men and women of 4.1% and 3.3%, respectively (2). Although there have been improvements in medical treatments, including neoadjuvant chemotherapy, preoperative imaging and surgical methods, approximately 40% to 50% of patients still have disease recurrence after receiving potentially curative surgical treatments (3). This demonstrates how critical it is to provide patients with CRC with better treatment alternatives.
The meta-analysis of five prospective cohort studies revealed that the risk of overall mortality was 29% lower in patients with CRC with high serum levels of circulating 25(OH)-vitamin D compared to those with low levels (4). Previous research showed that patients with cancer frequently have low levels of serum vitamin D (5, 6). The mean vitamin D level in blood of Thai patients with CRC is reported as 17 ng/ml, which is lower than the level in patients with other cancer types (20.3 ng/ml, p=0.036) (7). There have been some reports on the association between CRC and serum levels of vitamin D. A serum vitamin D level of 10 ng/ml (25 mmol/l) has been correlated to a 29% decrease in cancer-related mortality and a 17% decrease in cancer incidence (8-10). Cholecalciferol, often known as vitamin D3 (VD3) or 1,25(OH)2D3, is the active form of vitamin D. It is well known that VD3 as a supplement is more potent at raising the serum 25(OH)-vitamin D concentration than VD2 (11). Additionally, some experimental data point to a potential role for VD3 in modulating both innate and adaptive immunity (12, 13), as well as a potential for activating T-lymphocyte-mediated anti-tumor immunity. Consequently, it can aid in preventing the spread of a tumor (14). Regulatory T-cells (Tregs), which are immune system cells that inhibit or favor the development of CRC, are a key factor in facilitating immunomodulation in patients with CRC (15).
VD3 is involved in immunological homeostasis, including in Treg activity and differentiation. It has been demonstrated that high levels of VD3 stimulate the lineage-specific forkhead box P3 (FOXP3) transcription factor, which is involved in Treg formation and function (16, 17). Additionally, it has been associated with an anti-inflammatory lymphoid polarization with a high proportion of Tregs and has been demonstrated to increase the quantity and function of circulating CD4+Tregs (18-20). When they control the immunological responses, Tregs may be useful in reducing inflammatory cells that promote tumor development. VD3-induced Tregs may also play a role in manipulating allo-immune and auto-immune T-cell responses by releasing interleukin 10 (IL-10) (21, 22) and transforming growth factor beta 1 (TGF-β1) (23), possibly through the release of granzymes and perforin (23) or through the expression of inhibitory co-receptors, such as cytotoxic T-lymphocyte-associated antigen 4, in order to prevent antigen presentation and initiation of the pro-inflammatory response (16). Following T-cell dominance, an increase in Tregs may hasten disease progression by suppressing T-cell antitumor effects (3). However, the action of Tregs and their prognostic impact on CRC are still debatable (17, 23-28), and Tregs appear to have different influences at different stages of CRC development (29). Therefore, to address the value of VD3 supplementation on CRC outcomes, which could potentially lead to personalized dietary and lifestyle interventions, it is necessary to investigate the immunomodulatory effects of VD3 on Tregs and their associated cytokines in the recovery of patients after surgery for early stages of CRC.
Materials and Methods
Ethical approval. The Institutional Review Board of the Research Affairs, Faculty of Medicine, Chulalongkorn University, and the Ethical Committee of the Police General Hospital have reviewed and approved the ethical issues of the study and the consent form. This study was a part of a randomized control trial registered at the Thai Clinical Trial Registry with the identification number TCTR20171106001 and informed consent was obtained from all participants.
Study design and data collection. A 3-month prospective cohort study was conducted among 28 Thai patients, aged 30-75 years, with early-stage (I-II) CRC who underwent surgery at the King Chulalongkorn Memorial Hospital and the Police General Hospital in Bangkok, Thailand. Patients with a body mass index of 18.5-22.9 kg/m2 who had serum creatinine <2.0 mg/dl, alanine aminotransferase and aspartate transaminase <35 IU/l, albumin ≥3.5 mg/dl, and white blood cell count ≥5,000 cells/mm3, were eligible for the study. Patients were excluded if they had received chemotherapy or radiotherapy, were taking vitamin D-containing supplements (>800 IU/day) unless they discontinued vitamin D supplementation at least 2 months prior to enrollment or had a history of hypercalcemia. Eligible patients were randomized to either a VD3-treated or an untreated group. At at least 1 month after surgery, the VD3-treated group started on VD3 at 8,000 IU/day for 3 months. Blood samples were collected at baseline, and at 1 and 3 months to evaluate Treg numbers and their associated cytokines.
Measurement of serum vitamin D levels. Serum 25(OH)D2 and 25(OH)D3 were detected by using liquid chromatography–tandem mass spectrometry (LC-MS/MS) at Ramathibodi Hospital. An Agilent 6460 triple quadrupole LC/MS equipped with Agilent JetStream Technology (Agilent, Santa Clara, CA, USA) was used, with an observed linearity from 1 to 250 ng/ml.
FOXP3+ Treg identification and flow cytometry. The population of Tregs in all individual blood samples was identified by flow cytometry. Briefly, 6 ml of fresh-heparinized whole blood were collected from patients with early-stage (I and II) CRC at each time point. Peripheral blood mononuclear cells (PBMCs) were then isolated by utilizing SepMate™-15 tubes (STEMCELL Technologies, Vancouver, Canada) and Lymphoprep (Alere Technologies AS, Oslo, Norway) and centrifuged with 1200×g for 20 minutes at 25°C. PBMC layer at the interface was then collected, and washed twice at 3,500 rpm in phosphate buffer saline for 5 minutes. PBMCs were resuspended in RPMI medium-1640 (Glico technology, New York, NY, USA), which was used to investigate the number of FOXP3 Treg, and were analyzed by flow cytometry. In order to distinguish FOXP3+ Tregs from total T-cells, 1×106 cells of PBMCs were incubated with fluorescein isothiocyanate-conjugated mouse anti-human CD4 and anti-human CD25 (BD Bioscience, San Jose, CA, USA) for extracellular staining and anti-human FOXP3 (eFluor 660; eBioscience, San Diego, CA, USA) for intracellular staining. An anti-FOXP3 isotype (Rat IhG2 K, eFluor 660; eBioscience) was used as an isotype control, and BD FACSCalibur and BD Bioscience flow cytometry was used to analyze CD4+CD25+FOXP3+ Treg cells.
Serum Treg-associated cytokines assay. In order to investigate Treg-associated cytokines, a commercial enzyme-linked immunosorbent assay kit (LEGENDplex™ Multi-Analyte Flow Assay Kits; BioLegend®, San Diego, CA, USA) was used to measure serum levels of IL-10 and TGF-β1. The assay was performed according to the manufacturer’s instructions. All assays were performed in duplicate. The samples were then analyzed by flow cytometry, using BD-FACSARIA III (BD Bioscience). The limits of quantification were 24.09 pg/ml and 208.52 pg/ml for IL-10 and TGF-β1, respectively.
Statistical analysis. Mean and standard deviations were used to describe all variables. Mean differences between normally distributed data warranted the use of t-tests. This work analyzed data with IBM® SPSS® Statistic 22 for Windows (IBM Corp., Armonk, NY, USA). A two-tailed value of p<0.05 was set as the significance threshold.
Results
Baseline characteristics. The blood samples were collected from 28 patients with early-stage CRC (36% TNM stage I and 64% TNM stage II), with a mean age of 61±1.1 years, with 64% being male. Furthermore, there was no statistically significant difference between the VD3-treated and untreated groups in mean serum 25(OH) D3 levels, percentage of Treg cells, IL-10, and TGF-β1 at baseline (Table I).
The baseline parameters of participants.
Serum 25(OH)D3 levels. As shown in Figure 1, there was no statistically significant difference (p=0.429) between the two groups in serum 25(OH)D3 levels at baseline. At 1 (p=0.017) and 3 months (p<0.001), the VD3-treated group had significantly higher serum 25(OH)D3 levels than the untreated control group. Serum 25(OH)D3 levels in the VD3-treated group had increased approximately 2-fold and 2.5-fold at 1 and 3 months after treatment, respectively, compared to the untreated group.

Serum 25(OH)-vitamin D3 level at baseline, and at 1 and 3 months in groups treated with and without supplemental vitamin D3 (VD3). Data are the mean±standard deviation (n=28).
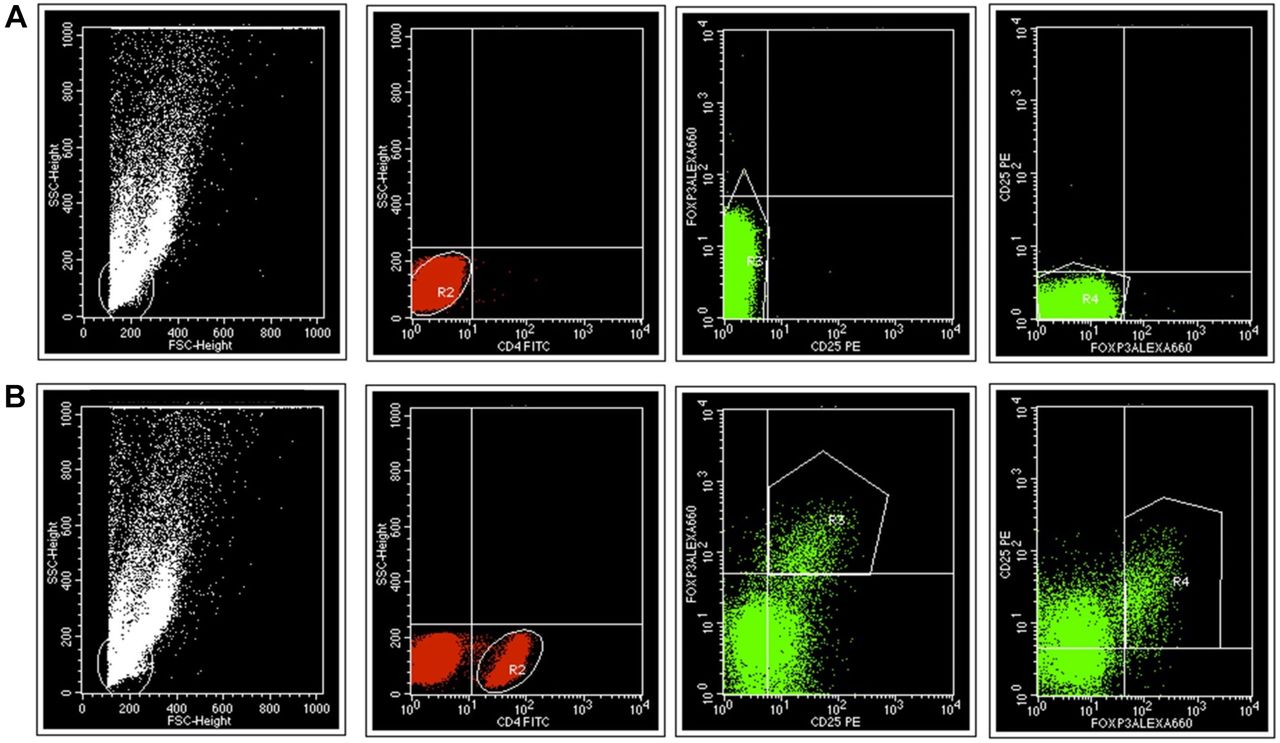
Changes in the level of Tregs. Treg population densities of VD3-treated and untreated groups were analyzed by flow cytometry in Figure 2. As shown in Figure 3, the results revealed that there was no significant difference in Treg levels between the two groups at baseline (p=0.866). At 1 month, Treg levels in the VD3-treated group were comparable to those of the untreated group. A significant increase in Treg level was observed at 3 months in the VD3-treated group compared to the untreated group (p=0.043). However, no significant difference in Treg levels at baseline, 1 month, or 3 months was observed in the VD3-treated group, indicating that VD3 had an immune homeostasis function on Tregs in this group.

CD4+ CD25+ and forkhead box P3+ (FOXP3+) regulatory T-cell (Treg) populations were gated by flow cytometry with BD FACSCalibur to determine T-cell population densities. A: Isotype control. B: Sample from patients with colorectal cancer. The CD4+ population was gated by sideward scatter and fluorescein isothiocyanate-conjugated anti-CD4+, and then Tregs were gated from CD4+ cells as the CD25+ FOXP3+ population. Scatter plots of CD25+ and FOXP3+ showed purity in the Treg (CD4+ CD25+ FOXP3+) cell population gating.

The mean percentage of regulatory T-cells (Tregs) at baseline, and at 1 and 3 months in groups treated with and without supplemental vitamin D3 (VD3). Data are the mean±standard deviation (n=28).
Serum levels of Treg-associated cytokines. As shown in Figure 4, there was no statistically significant difference in IL-10 and TGF-β1 levels between the two groups at baseline. After 1 month of supplementation, the serum IL-10 level in the VD3-treated group was significantly increased when compared to the control group (p=0.032) (Figure 4A). There was no significant difference in serum levels of TGF-β1 between the two groups, although TGF-β1 levels in the VD3-treated group were lower than in the control group at baseline and after 1 month of supplementation (Figure 4B).

Levels of serum interleukin-10 (IL-10) (A) and transforming growth factor-β1 (TGF-β1) (B) in groups treated with and without supplemental vitamin D3 (VD3). Data are the mean±standard deviation (n=26).
Discussion
In this study, the results demonstrate that VD3 has a potential role in modulation of Tregs by maintaining Treg levels in the early stages of CRC. Contrary to the general concept that a high proportion of FOXP3+ Tregs usually correlates with a poor prognosis in patients with cancer (30, 31), some previous studies showed that Treg numbers and activity were related to a better prognosis (32, 33). Depending on the type of immune responses in the tumor microenvironment and the stage of the disease, Tregs have different functions in patients with CRC. Tregs have been shown to be beneficial when inflammatory cells that promote tumor progression dominate. However, when the immune response is suppressed by T-cells, Tregs may accelerate tumor progression and suppress the antitumor effects of the immune system (3).
Serum 25(OH)D3 levels increased significantly after 3 months of supplementation with 8,000 IU/day VD3. The result was the maintenance of Treg numbers in the VD3-treated group compared with the, albeit non-significant, decreasing Treg numbers in the unsupplemented group. This study was performed in patients with early-stage CRC who had only been treated with surgery and had no disease progression. The results of this study correspond with a previous study conducted in healthy subjects (34). The previous study’s finding showed that the VD3-treated group had a higher proportion of Tregs (6.4%±0.8%) than the untreated group (5.5%±1.0%) at 3 months. This finding suggests that maintaining the number of Tregs would benefit patients with early-stage CRC by preserving immune homeostasis.
The results of this study showed that the mean concentration of serum IL-10 in the VD3-treated group was statistically significantly increased at 1 month compared to the control group (p=0.032), but not for TGF-β1. IL-10 usually regulates the emergence of long-lasting inflammatory processes. Chronic inflammatory reactions, especially in the gut, are related to IL-10 deficiency and may be brought on by normal enteric antigens (35). Additionally, IL-10 can prevent the production of pro-inflammatory cytokines, stimulating the growth of tumors (36). As a result, VD3 would be expected to be beneficial in increasing IL-10 and Treg-associated anti-inflammatory cytokines in patients with early-stage CRC. This result corresponds with the findings of a study in patients with multiple sclerosis that indicated a significant increase in the level of serum IL-10 after receiving high-dose vitamin D for 3 months (β=0.737, R2=0.91 and p=0.015) (37).
In our study, a trend for an increase in the level of TGF-β1 in the VD3-treated group at 1 month was observed. However, the difference was not statistically significant when compared to the untreated group. TGF-β1 causes a decrease in colonic epithelial cell proliferation, which promotes differentiation and apoptosis (38). Disruption of TGF-β1 signaling in CRC cells may promote tumor formation in the early stages of CRC, whereas TGF- β1 activation may promote cancer invasion and metastasis (39). In addition, TGF-β1 signaling is required to enable the survival of peripheral Tregs (40). In our study, increased TGF-β1 levels and maintenance of Treg numbers in the VD3-treated group suggest that VD3 might modulate the immune cell response in patients with early stages of CRC.
A chemical network model study on vitamin D sensitivity and immune response suggested that an elevated level of Tregs is present when the vitamin D level is optimum (41). Once the effector T cells start increasing, production of vitamin D is up-regulated, which in turn up-regulates the number of Tregs when the adaptive response occurs, by influencing the vitamin D receptor/phospholipase Cγ 1/TGF-β1 pathway (42).
In addition, a narrative review showed significant molecular findings relating to vitamin D and tumorigenesis from some published data. Vitamin D deficiency may favor a microenvironment leading to tumor growth and progressive tumor aggressiveness (43). Some studies have also reported a relationship between vitamin D and the function of tumor-suppressor genes, including the adenomatous polyposis coli gene (44). Furthermore, inverse correlations between vitamin D levels and cancer-specific survival have been found for several cancer types, including CRC (45). A retrospective study investigating the impact of postoperative vitamin D deficiency on colon cancer recurrence after surgery revealed that vitamin D deficiency at 1 year after surgical resection was associated with increased disease relapse among patients with stages I to III of colon cancer (46). The present study’s findings highlight the potential usefulness of VD3 supplementation on Tregs and immune homeostasis in patients after surgery for early-stage CRC, especially for patients with hypovitaminosis D.
In conclusion, our findings elucidate the immunomodulatory activity of VD3 supplementation on Tregs in blood samples from patients after surgery for early-stage CRC. This study’s evidence suggests that VD3 is an immunomodulator that promotes Tregs to maintain immune homeostasis in patients with early stages of CRC by increasing Treg-associated cytokines and maintaining Treg numbers. It is worth noting that a person with an insufficient 25(OH)D3 level may require vitamin D3 supplementation to strengthen their immune system against cancer. The result from this study might potentially serve as a basis for future studies needed to assess the long-term effects of VD3 on the number and function of Tregs, as well as other immune cells.
Acknowledgements
This work was financially supported by Thammasat University Research Fund to Sophida Sukprasert, contract no. TUGR 2/61/2562, and partially supported by Chulabhorn International College of Medicine, Thammasat University Research Fund to Sophida Sukprasert, contract no. 12/2559, and Graduate Student Research Scholarship by the National Research Council of Thailand to Patnapa Srichomchey, contract no. 23/2561.
The Authors would like to express their gratitude to Dr. Chanyawat Sangsomwong, Dr. Prapon Kanjanasilp, and Dr. Songpol Malakorn, Colorectal Division, Department of Surgery, Chulalongkorn University Hospital and Dr. Warunyu Jiramarit, Department of Surgery, Police General Hospital for all their supports in patient investigation and recruitment, and to Miss Chutima Kirdpattum and Miss Supanit Santaveesuk, Chulalongkorn University Hospital for all their helps in patient screening. The Authors would like to thank Dr. Noel Pabalan for English language editing.
Footnotes
Authors’ Contributions
Conceptualization: Patnapa Srichomchey and Sophida Sukprasert. Methodology: Patnapa Srichomchey, Sophida Sukprasert and Putthapoom Lumjiaktase. Software and formal analysis: Patnapa Srichomchey and Putthapoom Lumjiaktase. Investigation: Nathapong Khulasittijinda and Chucheep Sahakitrungruang. Writing-original draft: Patnapa Srichomchey, Sophida Sukprasert and Putthapoom Lumjiaktase. Visualization: All Authors. Supervision: Narin Voravud and Putthapoom Lumjiaktase. Final revision of the article and project administration: Sophida Sukprasert and Putthapoom Lumjiaktase. All Authors have read and agreed to the published version of the article.
Conflicts of Interest
The Authors declare no conflicts of interest.
- Received October 4, 2022.
- Revision received December 6, 2022.
- Accepted December 7, 2022.
- Copyright © 2023, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.