


Abstract
Background/Aim: A feline inductive odontogenic tumor (FIOT) is a rare type of tumor that is unique to young cats. Case Report: Herein, we report on three cats (aged 6 months to 2.5 years) that had a bulging mass on the maxilla. On diagnostic imaging, cases 1 and 3 had bone expansion in the affected area, and all three cats were diagnosed with FIOT by histological examination. Maxillectomy and/or incisivectomy techniques were performed according to the tumor site with an intended surgical margin of 5 mm. To increase both precision and safety, a piezoelectric surgical instrument was used. The local advancement flaps were used to repair the surgical sites. The surgical outcomes were excellent, and there were no major complications related to the surgery or tumor recurrences during long-term follow-up (3-5 years) for any of the cats. Conclusion: The results from this study were excellent, which may have been due in part to the choice of the surgical instrument that allowed for the implementation of precise and accurate surgical excision and the tension-free flap method for preventing dehiscence of the surgical site.
- Oral tumor
- feline inductive odontogenic tumor
- maxillectomy
- piezoelectric bone surgery
- long-term follow-up
In general, most oral tumors in cats are malignant (1). Squamous cell carcinoma is the most common oral tumor in cats, followed by fibrosarcoma (1). An odontogenic tumor is a rare type of oral tumor in cats that arises from remnants of embryonic tissues destined to develop into teeth and associated structures (2, 3). Odontogenic tumors are classified by their differentiated cell types and inductive properties (4). A feline inductive odontogenic tumor (FIOT) develops from the odontogenic epithelium and induces mesenchymal elements to form aggregated dental papillae (4).
FIOT has been misdiagnosed as ameloblastoma, ameloblastic fibroma, and inductive fibroameloblastoma. However, it is mostly confused with ameloblastoma (5). Feline ameloblastoma is similar to FIOT; however, only epithelial proliferation is observed, and inductive properties are not present in the former. Additionally, feline ameloblastoma occurs in both the maxilla and mandible with equal frequency in cats aged 6 years and older (6).
FIOT is unique to young cats (usually 8-18 months) and occurs with equal frequency in males and females (4, 7, 8). It usually occurs in the rostral maxilla and can be associated with missing teeth (4, 7). Although FIOT is benign, it is locally invasive and causes expansion of the bone. Thus, the recommended treatment is surgical excision, which includes a maxillectomy or mandibulectomy (6, 8, 9). If clean margins are achieved during surgical excision, the prognosis of FIOT is good (10).
Additionally, to improve the surgical results, a piezoelectric surgical instrument is used in these cases. This system is slower than powered rotatory instruments; however, it is safe and precise, reduces tissue trauma, and improves healing at the surgical site Hennet (11).
Also, previous studies have mostly reported short-term follow-ups after surgical treatment (4, 7, 12). In this study, three cases of FIOT were presented to the veterinary hospital for specialized dentistry to assess and treat oral tumors from October 2015 to August 2018. Medical information was obtained from the medical records, including history, physical examination, laboratory diagnostics, diagnostic imaging, surgical treatment, and outcome, along with follow up care. This report describes the diagnosis from histological findings, successful surgical treatment, and long-term follow up (3-5 years) of three cats with FIOT.
Case Report
Case 1. A 2.5-year-old spayed female Korean short-hair cat weighing 5.4 kg with a mass in the rostral maxilla was presented to the Dentistry and Oral Surgery Service at Evichi Veterinary Dental Hospital (EVDH) for specialized dentistry. Awake oral examination revealed an oral mass extending from the mesial aspect of the right maxillary canine tooth to the mesial aspect of the left maxillary third incisor tooth, which engulfed the maxillary incisor teeth. The mass was firm, bright red, and measured about 20×15×6 mm (Figure 1A). For diagnostic purposes, thoracic radiographs, intraoral dental radiographs, CT scans of the head, and an incisional biopsy for histopathologic evaluation were obtained.

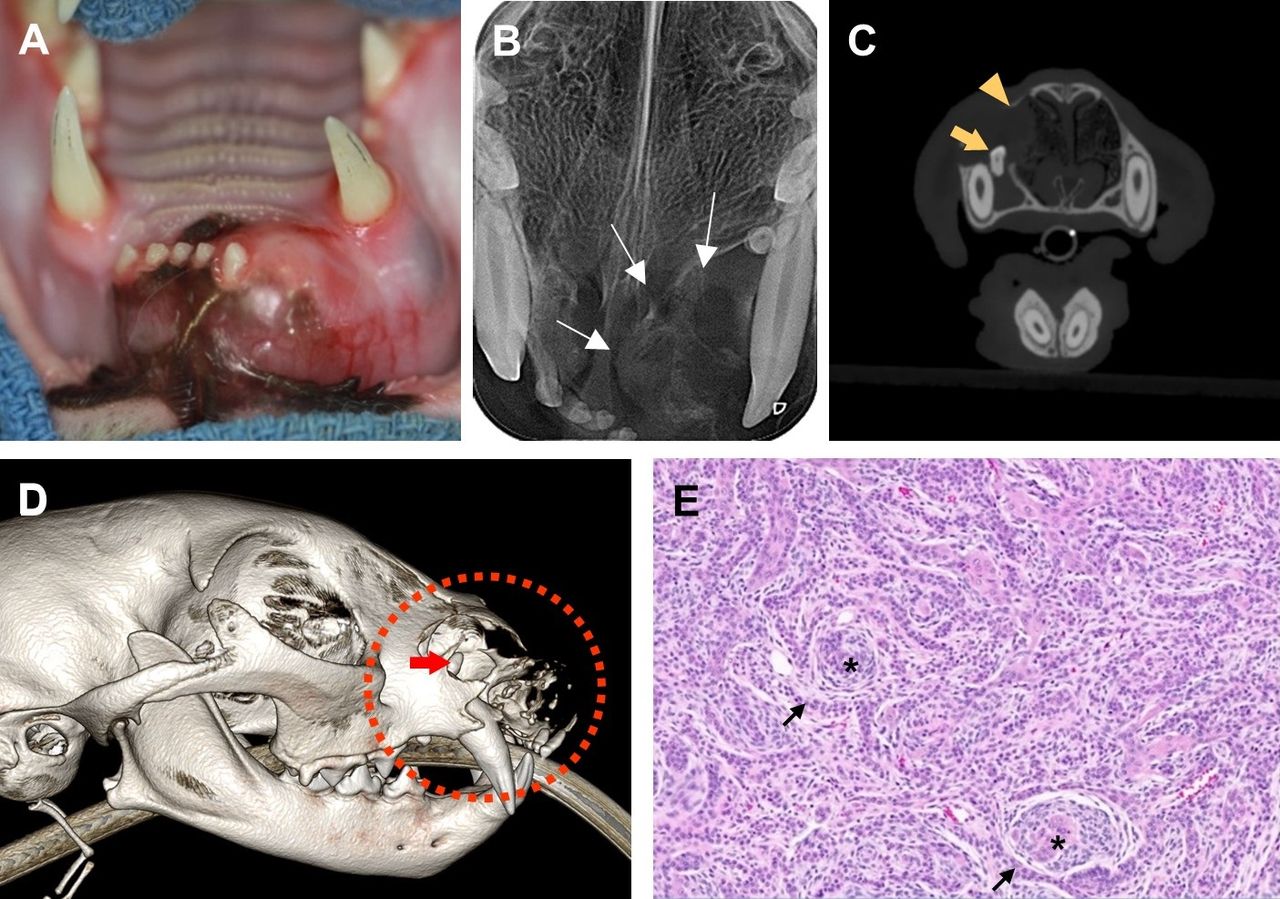
Diagnostic images of case 1. (A) An intraoral photograph of case 1 with a right maxillary tumor. (B) Intraoral radiograph of the rostral maxilla. The incisive bone reveals expansion, and tooth resorption is present (arrows). (C) The incisive bone is shown expanding to the rostral aspect of the right palatine fissure on computed tomographic bone windowed imaging in the dorsal plane (dotted circle). (D) Nodular neoplasm composed of trabeculae of the peripherally palisading odontogenic epithelium (arrows) and circular aggregates of mesenchymal differentiation (asterisks) are found on histological examination. (Hematoxylin and eosin stain, ×10).
Ampicillin (Penbrex inj; Yungjin Pharm, Seoul, Republic of Korea) at 20 mg/kg and butorphanol (Butophan; Myungmoon Pharm, Seoul, Republic of Korea) at 0.1 mg/kg were administered intravenously before general anesthesia. Anesthesia was induced through the intravenous administration of midazolam (Midacum; Myungmoon Pharm) at 0.2 mg/kg followed by propofol (Provive 1%; Baxter, Gurgaon, Haryana, India) at 4 mg/kg. After intubation, inhalation anesthesia was maintained using sevoflurane (Sojourn; Piramal Critical Care, Bethlehem, PA, USA). Intraoral radiographs from the maxilla revealed considerable expansion of the incisive bone from the mesial aspect of the right maxillary canine tooth to the mesial aspect of the left maxillary third incisor tooth that extended to the rostral aspect of the right palatine fissure on the occlusal view. Tooth resorption of the right maxillary third incisor and left maxillary first and second incisor teeth were observed. The right maxillary first and second incisor teeth were missing (Figure 1B). CT imaging (Emotion 6; Siemens, Medical Solutions, Germany) using bone tissue algorithm revealed an expansile mass, approximately 20 mm in diameter, localized to the incisive bone with a periosteal reaction (Figure 1C).
Before the incisional biopsy, meloxicam (Metacam injection; Boehringer Ingelheim, Ingelheim, Germany) was administered subcutaneously at 0.1 mg/kg, and bilateral infraorbital regional nerve blocks were administered using bupivacaine (Bupivacaine HCL 0.5% Inj; Myungmoon Pharm) at 1 mg/kg. A deep incisional biopsy was obtained from the central region of the mass, and samples obtained for histopathology were fixed in 10% neutral-buffered formalin and sent to a commercial laboratory (IDEXX VetConnet PLUS; IDEXX, Westbrook, ME, USA). A board-certified veterinary pathologist reported that the oral mucosa sections contained a nodular neoplasm comprising trabeculae of the peripherally palisading odontogenic epithelium (Figure 1D). Many of the trabeculae contained central stellate cells, and there were several circular aggregates of mesenchymal differentiation. Additionally, the neoplastic cells had some cytoplasms with round nuclei and a single prominent nucleolus, the anisocytosis and anisokaryosis were mild, and mitotic figures were rare. Thus, based on these histological results, case 1 was diagnosed as FIOT.
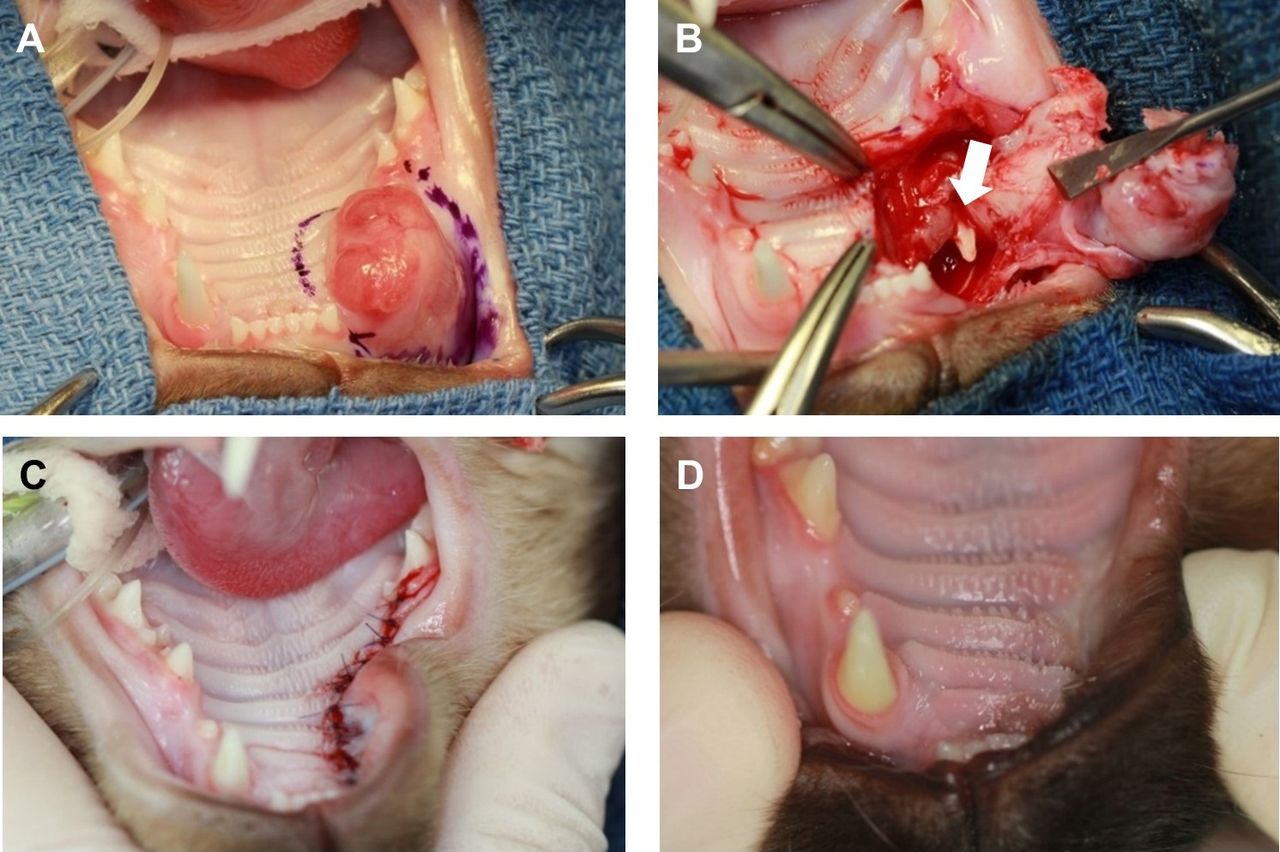
A unilateral rostral maxillectomy (mesial to the right maxillary second premolar tooth) in combination with a bilateral incisivectomy was planned. The cat was re-anesthetized in the same manner as described above and the same pain medications were administered. Additionally, a 12 μg/h transdermal fentanyl patch (Durogesic; Janssen-Cilag, GmbH, Neuss, Germany) was applied for postoperative pain control. The surgical margins were designated at 5 mm and marked around the tumor’s circumference using a sterile surgical pen (Figure 2A). An incision was made along the marked surgical margins to the bone. The soft tissues, including the palate, gingiva, and buccal mucosa, were subperiosteally elevated away from the osteotomy site using a 24G periosteal elevator. The osteotomy was performed using a piezoelectric surgical instrument with a serrated tip (Piezotome M+, Bs1s or Bs1L; Acteon, Merignac, France) (Figure 2B). The tumor segment was removed using a Molt #9 periosteal elevator (Figure 2C). The sharp bony ridges and spikes were smoothed using a diamond-coated tip (SL1 surgery tip; Acteon). A locally advanced mucoperiosteal flap was elevated for tension-free suturing (13). The locally advanced mucoperiosteal flap was closed in a T-shaped single layer using a simple interrupted suture pattern with a 5-0 poliglecaprone 25 (Figure 2D).

Photographs of the surgical procedure for case 1. (A) A unilateral rostral maxillectomy and a bilateral incisivectomy are planned. (B) The ostectomy is performed using a piezoelectric surgery instrument with a serrated tip. (C) A photograph after the tumor is excised. (D) The mucoperiosteal flap is closed using a simple interrupted pattern suture in a T-shaped single-layer flap.
The removed tumor segment was sent to a commercial laboratory where the surgical margins were examined, and complete excision was confirmed. The owner was instructed to offer only softened food, to avoid oral play for 2 weeks, and to flush daily with 0.12% chlorhexidine gluconate rinse. At the 2-week follow-up examination, the cat was eating well, was not experiencing any adverse effects from the surgery, and the sutured oral mucosa was well healed. The cat was followed up every 6 months for 5 years with conscious oral examination and continued to do well with no tumor recurrence.
Case 2. A 6-month-old female Siamese cat weighing 3.5 kg was presented to the EVDH for surgical treatment of an oral mass on the rostral maxilla. According to the owner’s report, the mass had begun to develop in the rostral part of the maxilla, starting at three months of age, and gradually increased. The referring veterinarian found that the right maxillary canine tooth was impacted on intraoral radiography, and a biopsy and histopathologic examination were performed. The cat was diagnosed with FIOT based on histologic examination by a board-certificated veterinary pathologist.
Conscious oral examination revealed an oral mass extending from the distal aspect of the right maxillary third incisor tooth to the mesial aspect of the right maxillary third premolar tooth. The mass was firm, bright red, and measured about 15×16×11 mm. The right maxillary canine tooth was missing. Though a CT scan was recommended for surgical planning, the cat’s owner declined for economic reasons.
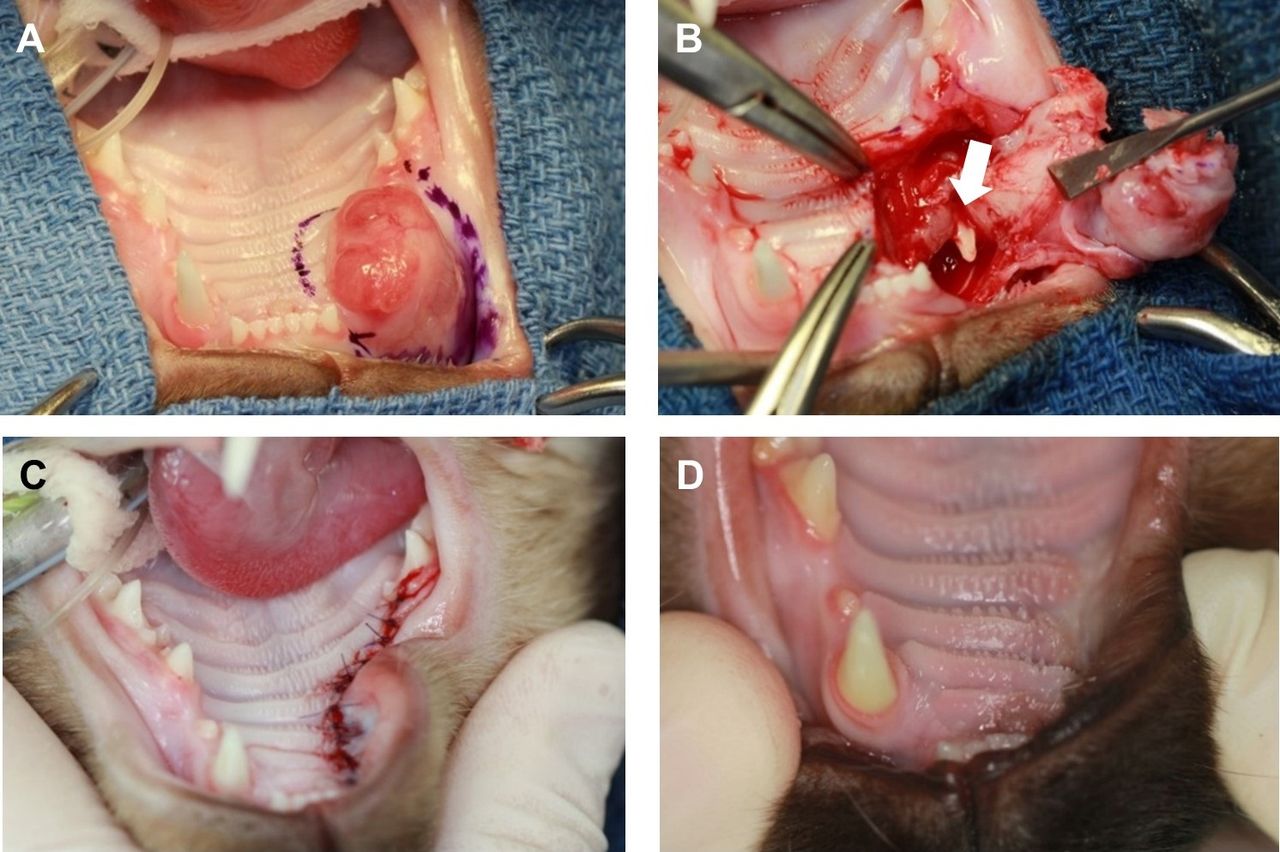
The cat was anesthetized in the same manner as described above for case 1, and the same pain medications were administered. A unilateral rostral maxillectomy including an incisive bone from the distal aspect of the right maxillary third incisor tooth to the mesial aspect of the right maxillary fourth premolar tooth was performed. The surgical margins were designated at 5 mm and marked around the circumference of the tumor (Figure 3A). The unilateral rostral maxillectomy was performed in a similar manner to that performed in case 1 (Figure 3B), except that the impacted right maxillary canine tooth was extracted. Then, the locally advanced mucoperiosteal flap was closed using a simple interrupted suture pattern (Figure 3C). After unilateral rostral maxillectomy, the right mandibular canine tooth was extracted, and the area was sutured to prevent occlusal trauma caused by the concavity of the upper lip. The excised tumor segment was fixed in 10% neutral-buffered formalin and sent to a commercial laboratory where the surgical margins were examined. The narrowest lateral surgical margin was found to be 0.91 mm, though the deep margin was dirty. Vascular invasion was not noted.
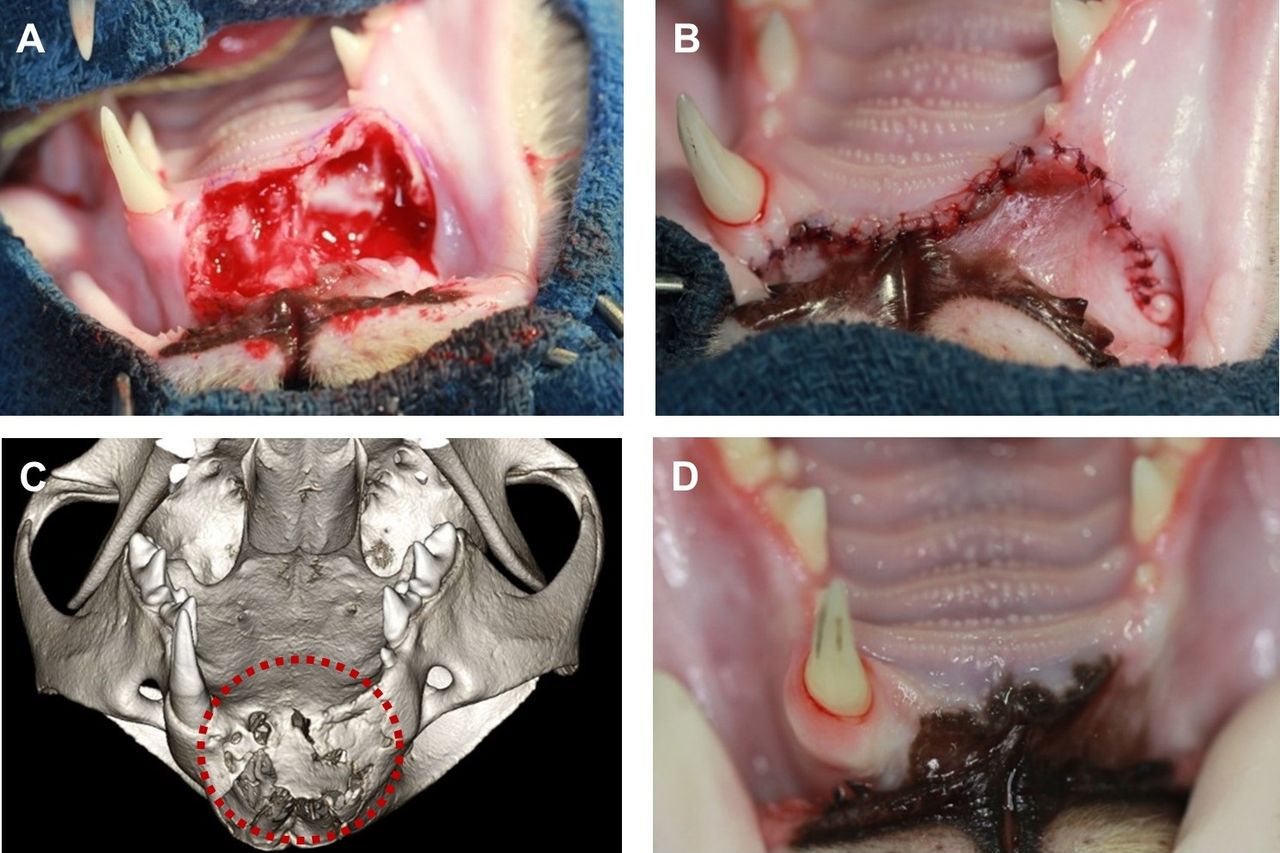
Photographs of the surgical procedure for case 2. (A) A unilateral rostral maxillectomy is planned. (B) The ostectomy is performed using a piezoelectric surgical instrument. The right maxillary canine is found impacted in the tumor (white arrow). (C) The mucoperiosteal flap is closed using a simple interrupted suture pattern. (D) The tumor excision site at the 4-year follow-up.
At the 2-week postoperative examination, the cat was eating well, was not experiencing any adverse effects from the surgery, and the sutured oral mucosa was well healed. The cat was followed up every 6 months for 4 years with a conscious oral examination and continued to do well with no tumor recurrence (Figure 3D).
Case 3. A 2-year-old castrated male Korean short-hair cat weighing 5.0 kg with an oral mass of the rostral maxilla was presented to EVDH for evaluation and treatment. The owner had noticed facial asymmetry due to the mass in the rostral maxilla, two months prior to presentation. However, the size of the mass had rapidly increased 4-5 days prior to presentation. The owner reported that the cat was experiencing discomfort while eating and could not close its mouth completely.
An oral mass extending from the distal aspect of the left maxillary third incisor tooth to the distal aspect of the right maxillary canine tooth was seen on conscious oral examination. The right maxillary third incisor tooth was missing, and a right maxillary canine tooth deviated mesiopalatally. The mass was firm, bright red, and measured about 20×15×13 mm (Figure 4A). For diagnosis, intraoral dental radiographs, cone-beam computed tomography; CBCT (NewTom 5GXL VET scanner; NewTom, Verona, Italy), and a biopsy were performed.
Diagnostic images of case 3. (A) An intraoral photograph of case 3 with a right maxillary tumor. (B) Intraoral radiograph of the rostral maxilla. The incisive bone expands to the rostral aspect of the right palatine fissure (arrows). (C) Cone-beam computed tomography transverse bone windowed image at the level of the canine teeth. The right maxillary 3rd incisor tooth is found non-erupted in the tumor (arrow). Maxillary and incisive bone lysis is seen (arrowhead). (D) 3D reconstructed cone-beam computed tomography image. The right maxillary 3rd incisor tooth is non-erupted (arrow), and extensive incisive bone lysis is observed (dotted circle). (E) A histological image from the resected tumor composed of epithelial cords (arrows) encircling whirls of odontogenic mesenchyme (asterisks). These complexes are embedded in dense collagenous tissue. (Hematoxylin and eosin stain, ×20).
Anesthesia, including positioning and pain medication, was performed in the same manner as that described for case 1. An intraoral radiograph revealed significant expansion of the rostral maxilla from the mesial aspect of the right maxillary canine tooth to the mesial aspect of the left maxillary third incisor tooth, extending to the rostral aspect of the right palatine fissure. Tooth resorptions of the right maxillary third incisor and left maxillary first and second incisor teeth were noted. The first and second incisor teeth of the right maxilla were missing (Figure 4B). CBCT evaluation revealed an expansile mass, approximately 20 mm in diameter, localized to the incisive bone with a periosteal reaction on the transverse bone-windowed view and 3D rendering image (Figure 4C and D). A biopsy specimen obtained for histopathology was fixed in 10% neutral-buffered formalin and sent to a commercial laboratory. A board-certificated veterinary pathologist examined the sample and diagnosed it as FIOT (Figure 4E).
A left incisivectomy and unilateral rostral maxillectomy (mesial to the right maxillary second premolar tooth) were performed. The cat was re-anesthetized in the same manner as that described for case 1. The surgical margins were designated at 5 mm and marked around the tumor. The surgical procedures were similar to those described for case 1 (Figure 5A); however, the mucoperiosteal flap was closed using a simple interrupted suture pattern in the shape of a straight line (Figure 5B). The resected tumor segment was fixed in 10% neutral-buffered formalin and sent to a commercial laboratory where the surgical margins were examined. On histopathology, the mass was diagnosed as FIOT and found to extend to the surgical margins.
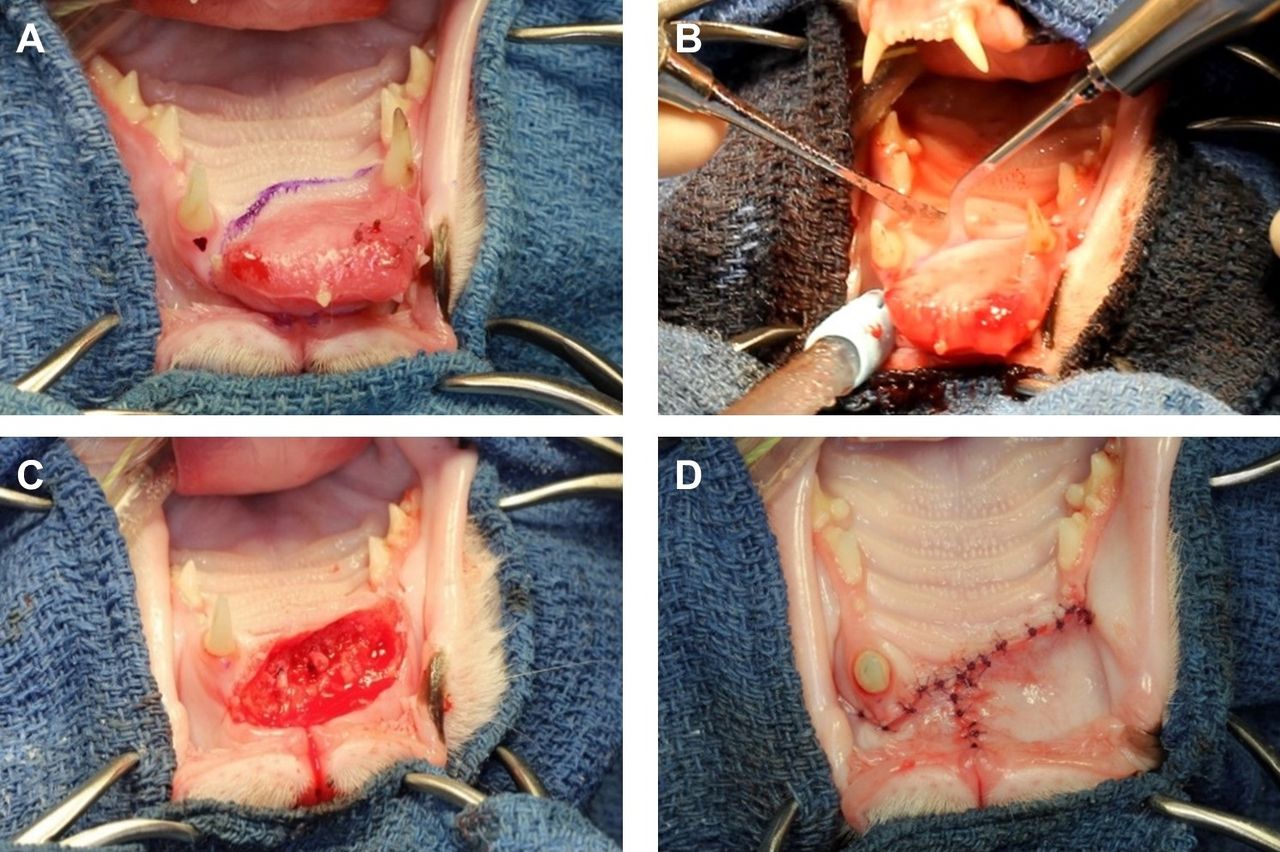
Photographs of the surgical procedure in case 3. (A) Surgical plan is unilateral rostral maxillectomy combined with bilateral incisivectomy. (B) The mucoperiosteal flap is closed in a simple interrupted suture pattern. (C) A 1-year follow up with 3D reconstructed cone-beam computed tomography reveals new bone formation in the rostral maxilla (dotted circle). (D) The tumor-resected site at the follow up 3 years after surgery.
At the 2-week postoperative follow-up examination, the cat was eating well, was not experiencing any adverse effects from the surgery, and the sutured oral mucosa was well healed. At the 1-year follow-up, the cat underwent CBCT scanning under general anesthesia, and CBCT images revealed new bone formation defined at the rostral maxillectomy site (Figure 5C). The cat was followed up every 6 months for 3 years with a conscious oral examination and was doing well, with no tumor recurrence on oral examination (Figure 5D).
Discussion
Odontogenic tumors are unique to the oral cavity and are rare in cats. Stebbins et al. (1989) reported that 2.4% of all oral tumors in cats over a 10-year survey were odontogenic tumors, with FIOT accounting for about 33% of the odontogenic tumors (1). Further, Schmidt et al. (2010) reported that in cats up to 1-year-old, the incidence of oral tumors was 10% of the total tumor incidence site rates. Of the oral tumors found in cats aged < 1 year, the prevalence of FIOT was relatively high (25%), which suggests that this type of tumor usually occurs in young cats (14).
FIOT is histologically a benign odontogenic tumor; however, it is clinically invasive and causes altered bone density in radiographic lesions (8). However, the prognosis is good when surgical resection is performed, and there is no study on the effectiveness or prognosis of chemotherapy and radiation therapy in FIOT yet (15). Additionally, surgery for FIOT requires wide excision, which should include the surrounding tissues, by maxillectomy or mandibulectomy (16).
In these cases, variable diagnostic images were used for surgical planning, such as maxillary resection or incisivectomy. In all cases, assessing abnormalities of the teeth affected by FIOT and incisive and maxillary bones were evaluated with intraoral radiographs. However, traditional intraoral radiographs can only obtain 2D images, thus providing insufficient information for surgical planning. Therefore, CT scan is widely used for better evaluation and surgical planning. In case 1, surgery was performed based on the multiplanar bone window and 3D reconstructions obtained from the preoperative CT scan.
Recently, surgical planning using CBCT has been implemented in the fields of veterinary dentistry and oromaxillofacial surgery. Images of bone structures are obtained with higher resolution compared to those obtained with traditional CT; the exposure to low radiation dose makes it safe for patients. The low soft-tissue contrast of CBCT generally precludes it from being considered the gold standard compared to a standard multiplanar CT in oromaxillofacial tumors. Therefore, the surgeon should miss alterations on the CBCT scan. The surgical plan should be established based on the 2D and 3D images together (17). Especially, in case 3, the extensive incisive bone lysis and complexity of maxillofacial anatomical structure were identified completely via CBCT imaging. Design for surgical margin and successful surgical outcomes were obtained through intraoral radiographs and CBCT images.
For both maxillectomy and mandibulectomy, an ostectomy is essential for the complete removal of the tumor with clean surgical margins. Ostectomies can be performed using hand instruments, including bone chisels or rongeur, and powered instruments, such as rotary burs and oscillating saws (11). Surgical hand instruments are still used; however, they can cause soft tissue injury to the mucosa, muscles, nerves, and blood vessels during ostectomy. Therefore, they should be applied carefully in complex anatomical structures of the oral and maxillofacial areas because they can induce iatrogenic trauma during surgery (11). Rotary instruments can be more delicate than hand instruments; for bone removal, an autoclavable straight or contra-angle surgical handpiece combined with a Lindemann bur, with built-in sterile saline or Lactated Ringer solution is a good choice (18, 19).
Another type of rotary instruments, such as a high-speed hand and burs, can be used in maxillofacial surgery with good outcomes (20). However, air exhausted from the handpiece may cause tissue emphysema in deeper tissue planes (18), and burs may cause trauma to the surrounding soft tissue. In addition, most high-speed handpieces use deionized water or tap water for irrigation fluid and the tubing cannot be sterilized (21). Tap water has been shown to be harmful to canine fibroblasts in vitro (22). Also, the microorganisms in tap water and biofilm that may occur in the waterline can contaminate the irrigation fluid and cause other side effects (23). Therefore, the high-speed dental handpiece and burs should be used very carefully for the complex anatomical structures in the oral and maxillofacial areas because they can induce iatrogenic trauma during surgery.
Oscillating or reciprocating orthopedic saws are faster than piezoelectric surgical instruments (11). However, they can cause uncontrolled damage to the bone or surrounding soft tissues. Cell death, bone lysis, and failed repair have been associated with this device due to thermal injury if proper irrigation is not utilized (11, 24-26).
To overcome these disadvantages, a piezoelectric surgical instrument can be used. This surgical instrument has several advantages when it is used in oral and maxillofacial surgery since it can effectively cut the bone without causing injury to the soft tissues; it is also associated with minimal bleeding during surgery, reduced neurological trauma, a significant reduction in postoperative edema, and precision in the cutting of complex anatomical structures (11, 27-29). Moreover, Ohira et al. reported that a piezoelectric surgical instrument promotes the postoperative healing process after surgery by osteocyte response (30).
For these three cases, maxillectomies were performed using piezoelectric surgical instruments. No complications, such as massive bleeding or damage to blood vessels, occurred, and the cats recovered quickly during the postoperative period. Additionally, this instrument allowed for a precise and clear excision, with no damage of the surrounding soft tissue.
For cases 2 and 3, the deep surgical margins were not clean. The rostral maxilla comprises incisive bone, soft tissue, some cartilage, and the rostral part of the nasal cavity structures. Owing to these anatomical characteristics, it is not easy to secure surgical margins for underlying tissues, including the rostral part of the nasal cavity structures. Furthermore, if the surgical margin was 10 mm, the anatomical part to be removed would be too wide, and functional problems may occur; therefore, the surgical margin was set to 5 mm, which was possible because this tumor was benign in nature and histologically low grade. However, the group of cases was too small, and thus further studies are needed for confirmation.
Also, new bone formation was detected in the rostral maxillectomy site at the 1-year follow-up in case 3. Bone regeneration from intramembranous ossification is thought to result from the remaining tissue. During intramembranous ossification, the undifferentiated mesenchymal cells of the connective tissue like the periosteum become osteogenic cells, such as the osteoblasts, that lead to bone regeneration and osteoclasts that resorb damaged bone (31, 32).
One major complication after a maxillectomy is dehiscence, which can occur in the first 4-5 days postoperatively (33). It is caused by inadequate suture placement, suture line tension, the use of electrosurgery, and marginal necrosis of the flap (33). However, flap formation without electrosurgical equipment, the tension-free flap technique, and adequate suture placement were performed in these cases; thus, there was no complication related to dehiscence.
Additionally, in cases 1 and 3, ipsilateral mandibular canine teeth were not extracted, and the cats were exhibiting entrapment of the upper lip by the mandibular canine teeth. A recent study reported that 13.4% of lip trauma occurred in maxillectomy cases in dogs (34). If it causes ulceration or other soft tissue trauma, the canine tooth should be corrected by crown height reduction and partial coronal pulpectomy, direct pulp capping, and restoration (35). However, there was no occlusal upper lip trauma in cases 1 and 3, therefore no further treatment was performed.
The limitation of this study is that the number of FIOT cases was small. This is likely due to the rare nature of this particular tumor type. In all three cases presented, a 5mm margin appeared to adequately address the tumor. The exact reason for such a narrow margin being successful remains to be fully understood; however, the benign nature of FIOT likely plays a role.
In conclusion, unlike previously reported cases of FIOT, these cats were followed up for 3-5 years. Excellent results were achieved for both the short- and long-term outcomes of the 3 patients in this report. Maxillectomy using piezoelectric surgical instruments and well-designed, tension-free flaps allowed for good healing. Despite narrow margins, there was no recurrence of the tumor in any of the patients, suggesting that the benign nature of FIOT may play an important role in surgical planning.
Acknowledgements
The Authors disclosed receipt of the following financial support for the publication of this article: This work was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Korea government (MSIT) (Daejeon, Republic of Korea) (NRF-2020R1C1C1009798).
Footnotes
Authors’ Contributions
Chun-Geun Kim and Se Eun Kim conceived and designed the study and wrote the manuscript. Eui Sin Yang collected and analyzed data. Frank J.M. Verstraete and Hee-Myung Park revised the manuscript for important intellectual content. Seong Soo Kang and Se Eun Kim supervised the study. All Authors read and approved the final version of the manuscript
Conflicts of Interest
The Authors have no conflicts of interest to declare in relation to this study.
- Received September 30, 2022.
- Revision received October 16, 2022.
- Accepted October 17, 2022.
- Copyright © 2023, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.