


Abstract
Background/Aim: Anterior tension band injuries are usually the result of high impact hyperextension trauma. Current surgical treatment includes anterior cervical discectomy and fusion bearing the risk of soft tissue irritation, degeneration of adjacent cervical segments, implant failure or iatrogenic spondylodesis. This study examined the biomechanical properties of tape suture constructs reenforcing ligamental stability for the treatment of Association of Osteosynthesis (AO) type B3 injuries compared to anterior fusion. Materials and Methods: After creation of an AO type B3 injury in synthetic cervical segments (C5/6, Sawbone®), seven segments were treated with anterior fusion and seven with a tape suture construct, similar to the SpeedBridge™ (Arthrex®). Biomechanical testing was performed, simulating extension, flexion, lateral bending, and rotation. Dislocation (°) and corresponding force (N) were measured and compared. Results: Anterior fusion displayed a mean range of extension, lateral bending, and rotation of 3.60° (SD 1.87°), 2.28° (SD 1.55°), and 2.81° (SD 0.78°), respectively. The tape suture showed a mean range of extension, lateral bending, and rotation of 4.24° (SD 0.81°) (p=0.146), 5.44° (SD 1.56°) (p=0.013), and 5.29° (SD 1.44°) (p<0.01), respectively. No specimen suffered from implant failure. Conclusion: The tape suture construct provides sufficient biomechanical stability for the treatment of AO type B3 injuries compared to anterior fusion. Regarding cervical extension, whose limitation is crucial for ligamental healing, the tape suture shows no significant inferiority. Yet, the tape suture approaches physiological mobility in the planes not affected by the injury. Consequently, the tape suture is a promising alternative preventing an iatrogenic spondylodesis.
Anterior tension band injuries are commonly caused by high impact trauma, such as traffic accidents, or frontal collisions, for example occurring in contact sports (1). From a biomechanical perspective, these anterior longitudinal ligament tears can be attributed to segmental extensions of the cervical column (2). However, hyperextension traumas can also increasingly be caused by low-impact trauma in geriatric patients, based on current demographic changes and the concomitant rise in aging society (3).
In accordance with the Association of Osteosynthesis (AO) classification, anterior tension band injuries are classified as type B3 injuries, involving the rupture of the longitudinal anterior ligament, and oftentimes also affecting the intervertebral disc, resulting in a physical disruption or separation of the anterior structures (4). In this type of injury, substantial dislocation is prevented by an intact posterior hinge (4).
However, disruption of the osteo-ligamentous column can lead to disc extrusion, acute neurological deficits like muscle weakness or paresthesia, pain, or chronic instability. Therefore, the indication for surgical treatment is given in all AO type B3 injuries of the cervical spine (5).
The current gold standard for the treatment of AO type B3 injuries of the cervical spine consists of an anterior cervical discectomy and fusion (ACDF) (6, 7). While the rigidity of this osteosynthesis ensures sufficient stabilization, it also bears various risk factors as it can compromise the surrounding tissue and create an unphysiological stiffness of the cervical spine, especially regarding flexion, lateral bending, and rotation. Besides restricting the mobility of the cervical spine, ventral arthrodesis can furthermore lead to dislocation or postoperative implant failure (8).
In a retrospective study, Ning et al. showed that out of 2,233 patients treated with ventral arthrodesis, 10.7% of the patients had severe complications at an average follow-up of 1.7 years. Among these were oblique plate implantations with partial nerve root irritation and loosening or dislocation of screws and plates with concomitant esophageal rupture in 3 cases (8).
Another complication after anterior plating is an accelerated degenerative change in the adjacent vertebral segments, however, the underlying etiology is not yet fully understood (9). This particularly includes disc degeneration, disc herniation, instability, spinal stenosis, spondylosis, and facet joint arthritis (9). As postulated by Eck et al., the significant biomechanical increase in the loading of the joints of the cervical spine above and below the spondylodesis during flexion potentially initiates the degenerative processes (10).
Cervical total disc replacement (CTDR) has displayed to be a promising alternative to an ACDF preserving mobility in the cervical spine (11, 12). Nevertheless, CTDR is currently solely indicated for degenerative disc disease, yet not authorized for the treatment of traumatic disco ligamental hyperextension injuries as it leaves the anterior instability caused by the ruptured anterior longitudinal ligament (ALL) unaddressed (11).
Aiming to restore the above mentioned ligamental stability, minimally invasive tape suture systems, such as the SpeedBridge™ by Arthrex® (Naples, FL, USA), have displayed promising results regarding biomechanical stability and are already routinely used for the surgical treatment of the syndesmosis of the ankle or ligamental injuries of the knee or shoulder (13-15). These minimally invasive implants aim to reinforce ligamental structures while maintaining micro mobility of the affected joint, ultimately combining the possibility of ligamental healing and the prevention of an unphysiological arthrodesis (14).
However, there are no data regarding the feasibility of these semi-rigid implants in combination with a disc replacement for the treatment of AO type B3 injuries of the cervical spine.
Consequently, the objective of this study was to examine the biomechanical properties of tape sutures for the treatment of AO type B3 injuries of the subaxial cervical spine.
Materials and Methods
Two groups, each consisting of seven composite synthetic cervical columns (Model: Spine, Cervical 1351, Sawbone® Pacific Research Laboratories, Vashon, WA, USA), were created. Next, the C5/6 cervical segments were isolated, maintaining the cervical disc and the anterior and posterior longitudinal ligaments (Figure 1). Based on a protocol of Röhl et al., screws were placed onto the upper and lower surfaces of the specimens to ensure optimal positioning through the creation of an even surface and to provide sufficient stability and force transmission (Figure 1) (7). The specimens were then casted into previously beveled pots (13°) and embedded in resin (RenCast® FC 52/53 Isocyanate/FC 53 Polyol, Huntsman Corporation®, Salt Lake City, UT, USA), maintaining their physiological alignment (Figure 2).

Prepared specimen with the surface screws (C5/6 segment) before embedding.

3D-printed casting guide to achieve a 13° casting line.
The bevel of the pots ensured sufficient space for internal fixation and added additional stability by casting the processus spinosus. The casting guide was designed using CAD (program: Fusion 360® Autodesk, San Rafael, CA, USA) and 3D printed (3D-printer: Original Prusa i3MK3S+®, Prusa Research, Prague, Czech Republique) to obtain an exact 13° casting line (Figure 2).
Subsequently, an AO type B3 injury was created by transecting the entire ALL and the intervertebral disc (4). Next, an anterior discectomy was performed, and a disc replacement (DePuy Synthes Cervios Cage curved, size 5 mm, West Chester, PA, USA) was implanted.
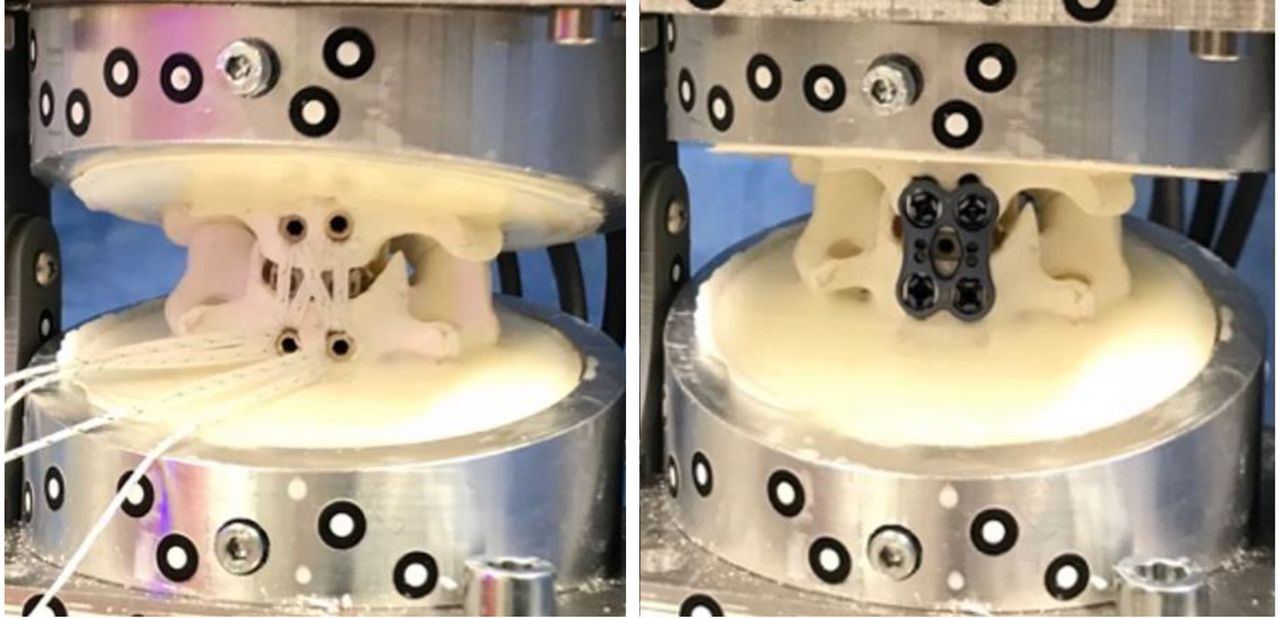
The specimens were then treated with either a standard ACDF or a tape suture osteosynthesis. In case of ACDF, a titanium anterior cervical plate (DePuy Synthes® 14 mm) was implanted with 4 screws (DePuy Synthes® ø 4.0 mm, L 16 mm) (Figure 3) (16). For the implementation of a tape suture osteosynthesis, 3.5 mm holes were pre-drilled into the ventral side of the vertebral bodies and 4 PEEK SwiveLock® ø 4.5 mm anchors with two FiberTapes® (Arthrex, Naples, FL, USA) were inserted in double row technique (Figure 3).

SpeedBridge™ in criss-cross technique and anterior cervical disectomy and fusion.
To generate a pure moment loading, the biomechanical loading method was adapted from a protocol obtained from Röhl et al. (Table I) (7).
Testing protocol.
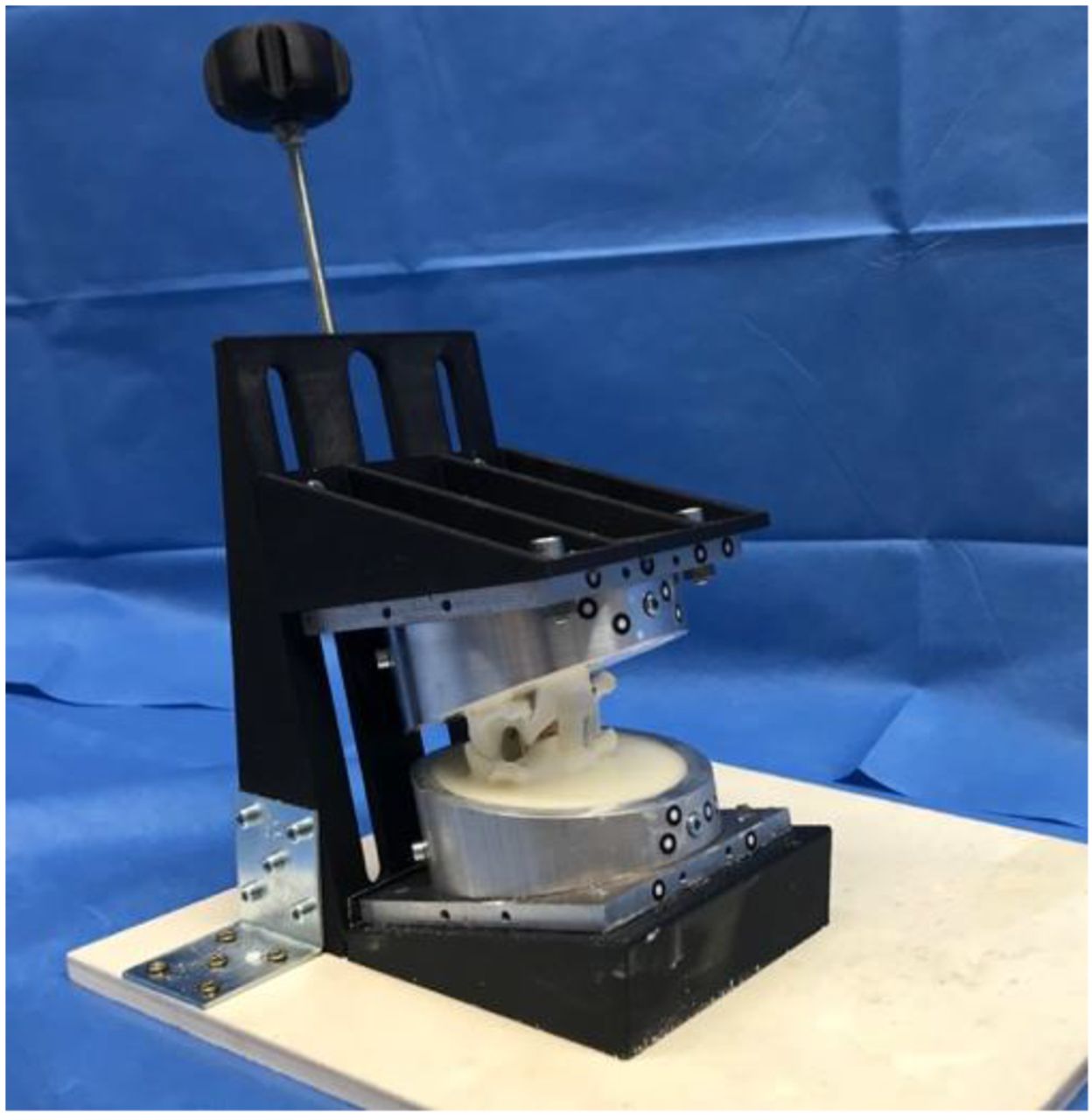
In this study, bending moments for flexion, extension, and lateral flexion were performed by the all-electric testing machine (Instron e10000, Norwood, MA, USA) through a 15 cm lever arm. The lever arm, which was exclusively designed with biomechanical engineers, consisted of a telescopic rail with ball bearings to ensure pure bending moment during motion (Figure 4) (17).

Test set-up. 1) 3D-printed supports with a central ball bearings-joint against rotational shear forces, 2) telescoping rail as lever arm, 3) specimen, 4) initial load of 50 N, 5 x-y-table, 6) load cell, 7) testing machine.
To avoid unphysiological tension during the mounting process, the base was mounted on a x/y table. Torsion moments were applied directly through the testing machine above the actuator (7). To achieve physiological conditions in terms of preload, an initial weight of 50 N was applied on the upper pot. Together with the resin, it accumulates to a total preload of around 75 N, simulating the force of the human head with approximately 5 kg (2) and upper cervical vertebrae. During rotation, the testing machine itself provided the preload. To avoid rotational shear forces during flexion and lateral bending, 3D-printed supports with a central ball bearings-joint were attached on both sides during testing (Figure 4). An optic sensor system (GOM Aramis 3D Camera 12M, GOM GmbH, Braunschweig, Germany) allowed the exact measurement of the bending angles (°) and dislocation (mm) of the specimens with a frequency of 3Hz. During embedding and experimental set-up, the vortices were always parallel to each other.
Fifteen cycles of biomechanical loading were performed to ensure final implant adaption and achieve reproducible results. The loading oscillated around neutral position to simulate complete head movements (18). The maximum speed was set to 0.5°/s (18).
In a preliminary trial, the plate osteosynthesis failed due to screw loosening after loading with the in literature recommended maximum load of 2 Nm (18), most likely due to the significantly reduced ligamentous structures in the synthetic models. Consequently, the momentum was halved to 1 Nm, ultimately enabling biomechanical testing under adequate conditions of all specimens.
Prior to the experiment, a case number estimation was performed based on a study of Duff et al. (19) using G* Power (Version 3.1.9.6., 2014, Düsseldorf, Germany). This resulted in a sample size of 7 per group to achieve a power of 95% with an alpha of 5%.
Statistical analysis was performed with IMB SPSS Statistics® version 28 (Armonk, NY, USA). A paired t-test was performed after demonstrating normal distribution using the Kolmogorov-Smirnov test.
Results
Regarding movement in the sagittal plane (flexion and extension), the tape suture construct showed a slightly higher dislocation with 4.24° [standard deviation (SD) 0.81°] than the plate with 3.60° (SD 1.87°) (Table I and Figure 5), however, not significant (p=0.146).

Plate group compared with tape group.
When considering lateral bending and rotation, the tape again showed a higher dislocation, however, here significantly (p<0.05), corresponding with a wider range of motion (Table II and Figure 5).
Mean dislocation in degree (°).
In detail, the tape suture construct allowed almost double the range of motion regarding lateral flexion (plate: 2.28°, SD 1.55°, tape suture: 5.44°, SD 1.56°, p=0.013) and rotation (plate: 2.81°, SD 0.78°, tape suture: 5.29°, SD 1.44°, p<0.01) (Table II).
Discussion
Hyperextension injuries of the cervical spine with a rupture of the ALL and the intervertebral cervical disc oftentimes result from high impact trauma (1). However, these injuries can also be increasingly observed in orthogeriatric patients after low impact trauma (3). Surgical treatment is required, especially in the case of simultaneous disc injury, ultimately resulting in hypermobility and instability (1).
ACDF represents the current standard treatment, including cervical discectomy and anterior fusion through a ventral plate osteosynthesis (20). However, there are numerous complications associated with a ventral cervical spondylodesis, such as plate malpositioning with consequent soft tissue or nerve root irritation as well as screw loosening resulting in nonunion (8). The postoperative swelling due to the extensive surgical invasiveness and the relevant size of the implants oftentimes lead to postoperative dysphagia (21). Xie et al. reported a complication rate of 10.7% in 2,233 of the cases after anterior cervical locking plate osteosynthesis, such as oblique plate implantations with partial nerve root irritation, soft tissue impairment and loosening or dislocation of screws and plates (8).
The fusion of several segments with long plates also affects the adjacent vertebral segments and ultimately leads to intervertebral disc degeneration, oftentimes requiring revision surgery (8). Another severe yet rarely observed complication is an esophageal lesion, at worst an esophageal rupture with subsequent mediastinitis and a high mortality (8, 16).
Most importantly, however, rigid plate osteosynthesis methods cause a loss of range of motion of the cervical spine in all planes (22). To fully understand this fundamental issue, it is essential to envision the relevant cervical anatomy and its physiological biomechanics. The cervical spine is one of the most complex articular systems in the body (23), providing an immense range of motion in three different planes: sagittal plane (extension: 40°/flexion: 45°), frontal plane (30°), and axial plane (50°) (24). In addition, no other musculoskeletal system is in such constant motion. With an average of over 600 movements per hour, the cervical spine is essential for and involved in almost every activity of the human body, such as speaking, gesturing, rising, sitting, walking, and turning (23).
As mentioned above, an AO type B3 hyperextension injury consists of a rupture of the anterior longitudinal ligament, which spans along the ventral sides of the vertebral bodies and is frequently associated with a lesion of the cervical disc (4). Physiologically, the ALL functions as a tension band, inhibiting a hyperextension and consequently stabilizing the cervical spine in the sagittal plane (2). The cervical disc functions as a “shock absorber”, cushioning and evenly distributing the effective biomechanical forces, and as a connection between the vertebral bodies, forming a functional motion segment (25). Therefore, an AO type B3 injury leads to an instability primarily regarding the extension of the cervical spine in the sagittal plane (4).
Consequently, sufficient treatment of this injury must address the sagittal instability; however, should leave the intact planes unaffected to maintain cervical mobility without compromising necessary ligamental healing, consistent with the principles of minimally invasive surgery and motion preservation.
Coherently, the most reasonable treatment for an AO type B3 injury should focus on the reconstruction or replacement of the affected tension band, the ALL, with a concomitant replacement of the cervical disc.
While the ACDF aims at a fusion of the cervical spine, resulting in an iatrogenic spondylodesis and nullifying the motion of the affected cervical segment, minimally invasive tape suture systems are capable of sufficiently addressing this injury with significantly less restriction to the physiological movement.
This idea of motion preservation for ligamentous injuries with flexible osteosynthesis or tape suture constructs has already successfully been realized for surgery of the ankle, shoulder, or knee (26-29). Recently, studies using tape sutures for the treatment of symphyseal ruptures have also been published by Cavalcanti Kußmaul et al. with promising biomechanical results (30).
To our knowledge, there are no data regarding the technique described above for the treatment of hyperextension traumas of the cervical spine. In this biomechanical study, the tape suture was biomechanically not inferior to the plate regarding the limitation of extension (p=0.146).
Comparing the segments overall mobility of 4.24° (SD 0.81°) in the sagittal plane after tape suture osteosynthesis to the physiological value of 19.7° (SD 3.4°) 31 and to the mobility after plate osteosynthesis (3.60°, SD 1.87°), the tape suture provides sufficient stability in the sagittal plane.
Furthermore, with 5.44° (SD 1.56°) (p=0.013) and 5.29° (SD 1.44°) (p<0.01) for lateral flexion and rotation, respectively, our analysis showed a significantly increased range of motion of the tape suture, approaching physiological values (31).
In detail, with a mean range of motion of 5.29° (SD 1.44°) for rotation, the tape shows a good approximation in the axial plane to the physiological motion of 9.3 (SD 1.9°) (31), whereas the plate almost entirely inhibits rotation of the affected segment (2.81°, SD 0.78°). Similarly, the tape suture displays a significantly higher range of motion (5.44°, SD 1.56°) in the frontal plane compared to ACDF (2.28°, SD 1.55°), again approximating the physiological value of 12.3° (SD 3.2°) (31).
Consequently, this study was able to demonstrate the capability of the tape suture construct to stabilize the cervical spine in the sagittal plane while preserving cervical micro mobility in the unaffected planes and ultimately preventing subsequent iatrogenic spondylodesis.
A further late consequence of segmental fusion is the degeneration of the adjacent segments, also called adjacent-segment disease (ASD) (9, 10, 32). Although not yet proven causative, increased force, and hypermobility in the segments adjacent to the fusion are considered probable (9). Eck et al. for example showed that after C5/C6 fusion, the pressure at C4/C5 increased by 73.2% and at C6/C7 by 45.3% (10). Furthermore, to explain the rapid degeneration of the adjacent segments, the authors postulated that an increased disc pressure restricts metabolism and leads to the local accumulation of waste products. Subsequently, this change in cell metabolism leads to a pH drop and to increased cell death. Other characteristic signs of degeneration are the induction of collagen-I synthesis by increased pressure and the simultaneous decrease of water-binding molecules such as proteoglycans (10). Although this type of change is indistinguishable from normal age-related degeneration, the incidence is higher in patients with spondylodesis of the cervical spine (10).
Girard et al. examined the radiological outcome of 15 patients with ventral plate osteosynthesis and found degenerative changes in 3 cases within the first year of follow up and in all 15 patients after 5 years of follow up (32). In addition, 6 patients showed signs of disc changes. The mean age of the patients at surgery was 33.5 years. Furthermore, the study was able to demonstrate hypermobility in the adjacent segments in 3 patients (32).
Although the use of minimally invasive suture anchor systems for the reduction of adjacent segment disease was not the subject of this study, it can be assumed that due to the increased mobility of the affected segment, the increased pressure in the adjacent segment is less and the resulting degenerative processes are slower or nonexistent.
Disco-ligamentous injuries of the cervical spine are best diagnosed by MRI (33). In case of none or minor disc injury but given surgical indication based on the rupture of the ALL with concomitant sagittal instability, the use of a tape suture system without disc replacement could be considered for ventral stabilization.
Yet, since the cervical disc is significantly impaired in most of the cases, ultimately leading to a degeneration of the cervical disc and potentially resulting in disc extrusion, aggravated instability, neurological symptoms or auto-fusion, the replacement of the cervical disc is of high relevance (34, 35). From a biomechanical point of view, motion preservation can preferably be approximated by the combination of a tape suture construct with a cervical disc prosthesis with a mobile core group. In this study, however, and concomitantly forming a limitation of this study, a cage was used as a disc replacement. Since this study used the ACDF as a reference group for the comparison, however, potential confounding variables, such as different methods for cervical disc replacement, were ruled out and the comparison of the biomechanical properties of the tape suture construct to an ACDF for the treatment of ALL ruptures was optimized. This consequently allows a primary step towards the evaluation of a tape suture construct for the treatment of hyperextension injuries, yet further studies, both in vivo and in combination with flexible cervical disc replacements, are necessary.
Regarding further limitations of this study, the use of synthetical cervical models only allows restricted conclusions for physiological conditions due to the minimal ligament architecture. However, this enables reproducible results as there are no anatomical differences between the specimens, allowing ideal conditions for biomechanical implant comparison. Furthermore, the dissection of all ligamental structures besides of the PLL of the synthetic bone models allowed the creation of an identical, maximal anterior instability in all specimens.
Nevertheless, in vivo studies are necessary to confirm the feasibility of tape suture constructs for ligamentous injuries of the subaxial cervical spine.
Another limitation lays in the impossibility of predictions on long-term stability of the anchors. Yet, as the construct is an established procedure for joint stabilization in other surgical fields, long term stability for the cervical spine can be assumed (15, 36).
In summary, our study shows sufficient and promising biomechanical properties of minimally invasive tape suture systems and subsequently presents a target-orientated surgical treatment for the stabilization of AO type B3 injuries of the cervical spine.
Prospectively, the combination of a tape suture construct for the reconstruction of an anterior stability in combination with a mobile core cervical disc prosthesis could preserve spinal motion and potentially present an alternative to an ACDF.
Acknowledgements
Adrian Cavalcanti Kußmaul disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the 11 [grant number 1124].
Footnotes
Authors’ Contributions
Study conception and design: Adrian Cavalcanti Kußmaul, Titus Kühlein, Axel Greiner, Wolfgang Böcker. Material preparation, experimental testing, data collection and analysis: Titus Kühlein, Bianka Rubenbauer, Adrian Cavalcanti Kußmaul, Manuel Kistler, Sandy Walter. First draft of the manuscript: Titus Kühlein, Christopher A Becker, Adrian Cavalcanti Kußmaul. Review of the manuscript: Bianka Rubenbauer, Axel Greiner, Christopher A. Becker, Jan Bruder. Implementation of improvement: Adrian Cavalcanti Kußmaul, Titus Kühlein.
Conflicts of Interest
Adrian Cavalcanti Kußmaul received financial support from the FöFoLe grant of the Ludwig-Maximilians-University Munich [grant number 1124]. All other Authors have no conflict of interest in relation to this study.
- Received November 21, 2022.
- Revision received December 2, 2022.
- Accepted December 6, 2022.
- Copyright © 2023, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.