


Abstract
Background/Aim: Regarding the surgical treatment of incomplete burst fractures of the spine, no optimal standard procedure has been established. While previous studies have focused on radiological and surgical outcome parameters, the literature has not elucidated economic aspects of various surgical treatment options in detail yet. This study aimed to investigate whether open and minimal-invasive approaches differ in their economic profit gain. Furthermore, we examined whether a single-stage or two-stage approach of anterior-posterior fusion was more profitable. Patients and Methods: By analyzing retrospectively data of 129 patients who underwent surgical procedure due to isolated incomplete burst fractures, we examined the economic profit and radiological parameter of open pedicle screw insertion, minimal-invasive techniques (percutaneous screws, percutaneous screws combined with SpineJack®, kyphoplasty or SpineJack®), and anterior-posterior fusion. Results: Percutaneous screws in combination with SpineJack® gained significantly higher profit and higher profit per day of hospital length of stay. Profit was similar after single-stage and two-stage approach of vertebral body replacement. No significant difference in radiological outcome after 24 months was detected between the various surgical techniques. Conclusion: From a financial aspect, our finding suggests that application of percutaneous screws in combination with SpineJack® may generate the highest economic profit gain regarding treatment of incomplete burst fracture.
The most common injury subtype of a spine injury is the burst fracture (AO Spine, AOS type A3) due to fall from a height, motor vehicle accident, and ground level falls (1, 2). In the United States of America 1,702 per 100,000 persons suffer from vertebral column injuries (3). In average, surgical treatment of spine fractures add up to 19,700 Euro in the Netherlands (4), whereas conservative treatment may cost up to 12,500 Euro. Regarding the adequate therapy of incomplete burst fracture of the vertebrae (AOS type A3) without neurological deficits no consensus exists. Both conservative and surgical approaches can be performed (5, 6), but surgery may have the better radiological outcome (4, 7-10). In terms of functional outcome and quality of life, surgical management did not show superiority over conservative management (3, 11). However, some authors described late neurological deficiency after non-surgical treatment (12, 13). Among the surgical approaches, there are various different techniques to choose from (14). Isolated posterior pedicle screw fixation allows anatomical reduction of the spine and correction of kyphotic deformities. However, there is a risk of loss of correction, which often makes an anterior fusion necessary, as the second step (15). The second step may be performed in the same hospital stay or some weeks later. This combined anterior and posterior fixation provides better restoration of the sagittal profile after 2 years (16). Furthermore, the posterior approach is associated with degeneration and decreased density of the back muscles (17, 18), and the literature reports a risk of soft tissue infections up to 8.5% after spinal instrumentation (19). Therefore, the development of percutaneous pedicle screw fixation, which spares the paravertebral musculature by smaller incisions, led to reduced blood loss, hospital stay, and infection rates (20-22), while retaining similar radiological and functional outcome (23). As an alternative to pedicle fixation, percutaneous vertebroplasty can be performed (24, 25). First described in 1987 (26), injecting bone cement into the fractured vertebra leads to decreased pain and deformities in compression fractures (27). A further development of this procedure represents the kyphoplasty. Before injection of the cement, a balloon is inflated and restores vertebral height (28). In comparison to vertebroplasty, kyphoplasty achieves better functionality in patients and causes less cement leakage (29). However, this procedure may be 10 to 20 times more expensive in some countries (30). The newest variety of this principle represents the vertebral augmentation system. Similar to kyphoplasty, a device is inserted into the vertebra and then expanded. Afterwards, the device is detached and left in the vertebra and cement is injected (28). The vertebral augmentation system (e.g., SpineJack® by Stryker, Kalamazoo, Michigan, USA) may provide better kyphotic angle correction and vertebral height restoration in comparison to vertebroplasty or kyphoplasty (31). Therefore, the aim of this retrospective study was to compare all these different surgical approaches regarding both radiological outcome and economic costs. Furthermore, the cost-effectiveness of combined anterior-posterior fixation against a two-step fixation was investigated.
Patients and Methods
A retrospective evaluation based on pseudonymized data was carried out for this study. In the period between January 2008 and December 2020, 129 patients with isolated vertebral body fractures, AOS Type A3, in the thoracolumbar spine after trauma treated in a Level I trauma center were included. Exclusion criteria were fractures due to infection or tumor disease, monosegmental Cobb angle under 15°, age over 75 years, patients with diagnosed osteoporosis, neurological deficiencies, multiple injuries, and AO type B and C fractures. These patients were divided into 5 groups in regard to the surgical technique they underwent: (I) open posterior fixation, (II) minimal-invasive percutaneous pedicle screw implantation, (III) percutaneous pedicle screw implantation in combination with SpineJack®, (IV) kyphoplasty and SpineJack® only or in combination, (V) posterior fixation with vertebral body replacement. General patient data were gathered from the patient records and listed using Microsoft Excel. Furthermore, economic data regarding length, total cost, revenue, and profit of hospital stay were evaluated. Economic data were collected by our financial department in a cost accounting methodology called activity-based costing (32), which is provided for diagnostic related groups (DRG) by the Institute for the Hospital Remuneration System (InEK GmbH) (33). X-ray images were taken preoperative period and up to 24 weeks postoperative to examine differences between the various methods regarding the cobb angle in the course up to the 24th week. The decision for operative or conservative care was made according to the customary and internationally recognized standards. Each author certifies that all investigations were conducted in conformity with ethical principles of research. Ethical approval was provided from the institutional review board (application number 9773_BO_K2021). Approval of data privacy was provided by the head of the department. Written informed consent for participation was not required for this study in accordance with the national legislation and institutional requirements.
Statistical methods. Statistical analysis was performed with SPSS V26 (IBM, Armonk, NY, USA) using a commercial personal computer (Windows 10 Professional Microsoft Corporation, One Microsoft Way Redmond, WA, USA). An analysis of variance (ANOVA) was performed (α=0.05/95%CI) to quantify the quality of the model, determining the statistical relationship between the procedure and specific outcome parameter like cobb angle and the specific economic values given above. Bonferroni-Correction was performed when necessary. Scatter plots and box plots were used to visualize dependence of metric and categorial values.
Results
Demographic data. Overall, the data from 129 patients could be extracted in the period from January 2008 to December 2020. Due to a moderate compliancy, data histories could not be obtained without gaps for all parameters. We examined 57 male and 72 female patients. Of these, 45 were treated with open, 20 underwent percutaneous surgery, and 24 kyphoplasty/spine jack. Six patients were treated with Spine Jack and screws combined. Twelve patients received anterior fusion in the first inpatient stay, and further 22 patients in the second inpatient stay. The age span (49.91±15.76) was almost normally distributed between 16 and 75 years (Figure 1). Figure 2 shows the distribution of age per interventional group. In detail, “open screws” in mean 45.80±14.66, “percutaneous screws” 42.55±13.66, “spine jack+screws” 66.33±4.32, “spine jack/kypho” 62.17±13.97, and replacement 48.50±14.73. Age distribution was significantly higher in “spine jack+screws” and “spine jack/kypho” as shown in Table I and Figure 2. Furthermore, length of stay in days was the shortest after “spine jack/kypho” (4.08±1.41) and the longest after “replacement” (12.03±7.28) (Table I). Length of stay after “open” procedure was 8.68±3.19 days and 6.85±4.04 days after “percutaneous” technique (Table I). The difference was significant (p<0.001). Four patients (8.9%), who underwent open screw implantation, needed surgical revision up to 1 year after dismissal (one wound infection needing one debridement; one wound infection needing 13 debridements; one implant failure needing one revision; one implant failure with wound healing disorder needing 5 revisions). After percutaneous implantation, 2 complications (10%) were observed within 1 year after dismissal. One wound infection needing one debridement and one adjacent fracture needing surgical revision. One patient of the “spine jack+screws” group (16.7%) developed a nosocomial pneumonia during the hospital stay and had to be treated in an intensive care unit. Regarding vertebral body replacement only one wound infection (2.9%) was observed withing one 1 year after dismissal needing one debridement (Table I).

Age distribution of included patients. Frequency of age in years of every included patient (N=129) showing a normal distribution. Mean=49.91 years.

Age distribution per group. Box plot diagram showing age distribution in years within each group. Age distribution was higher in “spine jack+screws” and “spine jack/kypho”. Number of patients in group “open screws” N=45, “percutaneous screws” N=20, “spine jack+screws” N=6, “spine jack/kypho” N=24 and “replacement” N=34. Black bar representing median. Blue bars representing interquartile range between first and third quartile. Whiskers represent data within 1.5×interquartile range. Data falling outside 1.5×interquartile range but within 3×interquartile range are plotted as outliers with a circle.
Main demographic values stratified by group.
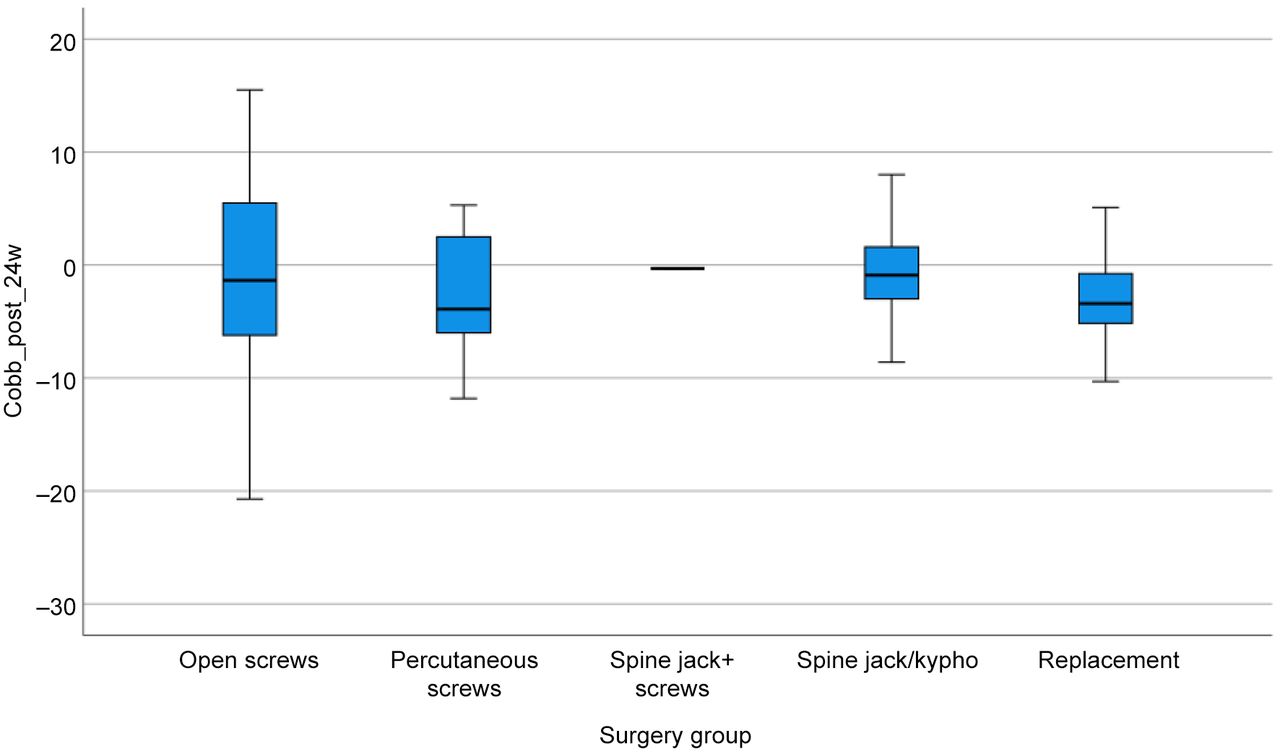
Analysis of Variance (ANOVA): Influence of intervention group on cobb angle direct postoperatively to 24 week follow up. With significant impact, the treatment group influenced the amount of surgical correction of the cobb angle (p=0.036). The two interventions with significant differences in the amount of correction (−6.78°±2.25) were vertebral body replacement versus SpineJack®/kyphoplasty (p=0.031, 95%CI=−13.22- −0.35, Figure 3). Referring to the outcome 24 weeks after surgery compared to the values directly postoperative, no significant difference in cobb angle could be detected (p=0.884, Figure 4).

Difference pre-/postoperative cobb angle in groups. Box plot diagram showing change of cobb angle after surgical intervention for each group. Lowest correction of cobb angle was achieved after “spine jack/kypho”. Number of patients in group “open screws” N=45, “percutaneous screws” N=20, “spine jack+screws” N=6, “spine jack/kypho” N=24 and “replacement” N=34. An analysis of variance was performed. Black bar representing median. Blue bars representing interquartile range between first and third quartile. Whiskers represent data within 1.5×interquartile range. Data falling outside 1.5×interquartile range but within 3 x interquartile range are plotted as outliers with a circle. Data falling outside 3×interquartile range are plotted as outliers with a star.

Differences postoperative cobb angle until week 24 in groups. Box plot diagram showing change of cobb angle after 24 weeks of intervention in comparison to directly postoperative correction for each group. After 24 weeks no significant difference regarding cobb angle between the groups could be detected. Number of patients in group “open screws” N=45, “percutaneous screws” N=20, “spine jack+screws” N=6, “spine jack/kypho” N=24 and “replacement” N=34. An analysis of variance was performed. Black bar representing median. Blue bars representing interquartile range between first and third quartile. Whiskers represent data within 1.5×interquartile range.
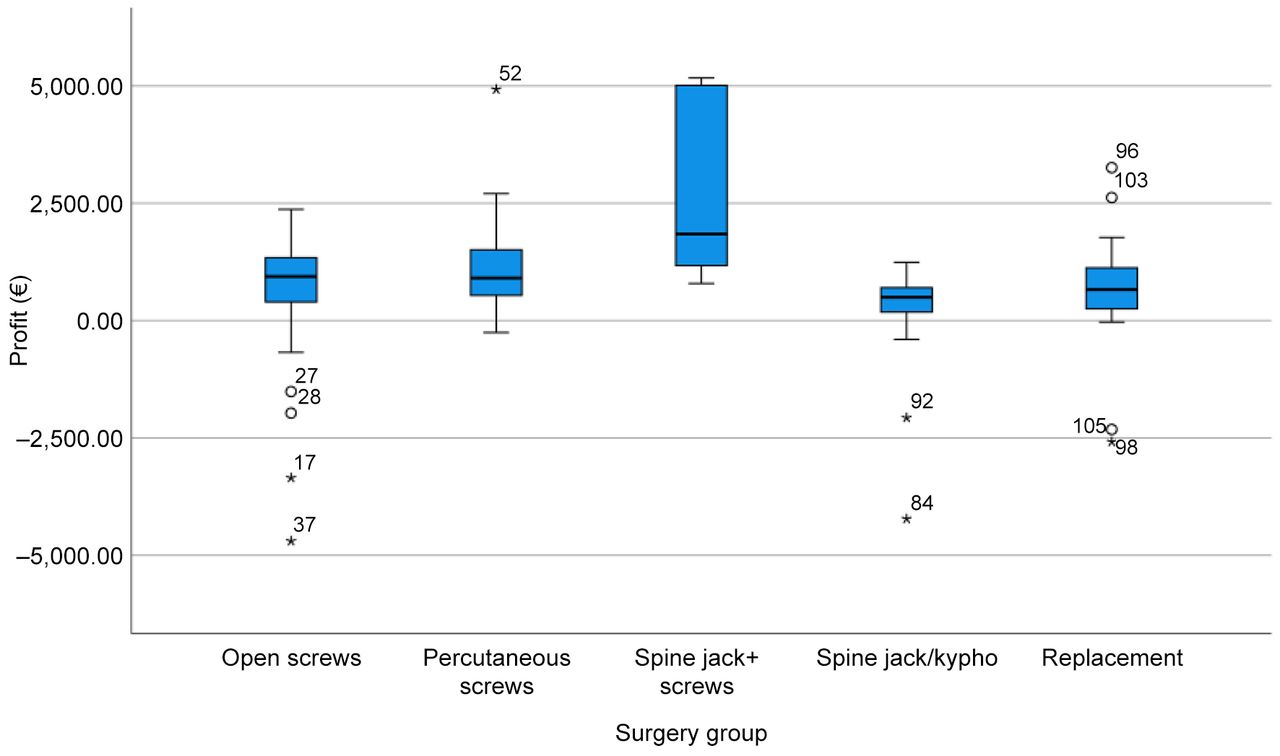
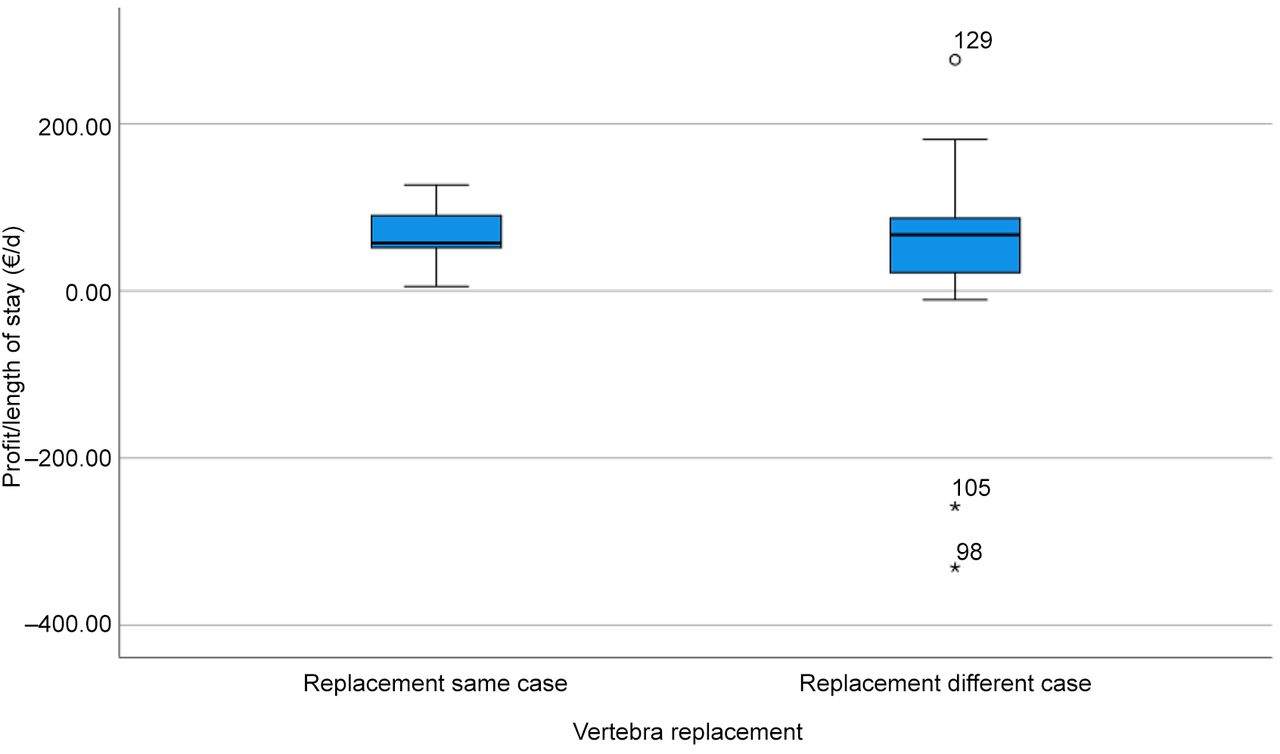
Influence of intervention group on main economic values: Table II shows the revenue stratified by groups being the highest after “open” procedure (11,900.69±4,603.65) and the lowest after “spine jack/kypho” (6,525.49±1,227.45). Regarding total cost, “open” technique caused the highest cost (11,214.03±4,426.54), whereas “spine jack/kypho” caused the lowest cost (9,037.10±3,412.30). Consequently, profit was the highest after “spine jack+screws” (2,799.65±2,126.62) and the lowest after “spine jack/kypho” (144.82±1,154.78). Regarding the length of stay, “spine jack+screws” gained the highest profit per day of stay (396.41±362.56), while “spine jack/kypho” generated the lowest profit per day of stay (30.68±351.41). These differences were significant. The combination of percutaneous screws with Spine Jack showed significantly more profit compared to all other interventions except for percutaneous screws alone (Table II, Table III, and Figure 5). For the profit per inpatient length of stay, the groups also differed significantly (p=0.005). Stratified by intervention group, SpineJack® combined with screws showed significant differences in comparison to all other interventions except for percutaneous screws (Table III, Table IV, and Figure 6). With high significance, the intervention groups showed differences in total revenue (p<0.001). Comparing anterior fusion being performed in the same inpatient stay or with a delay weeks after in a different case, statistically, there was no significant difference in profit (p=0.391) by stratification of groups (Figure 7). With p=0.526, there was no significant difference in profit per length of stay either (Figure 8).
Main economic values stratified by groups.
Combination Spine Jack+screws compared to other for total profit.
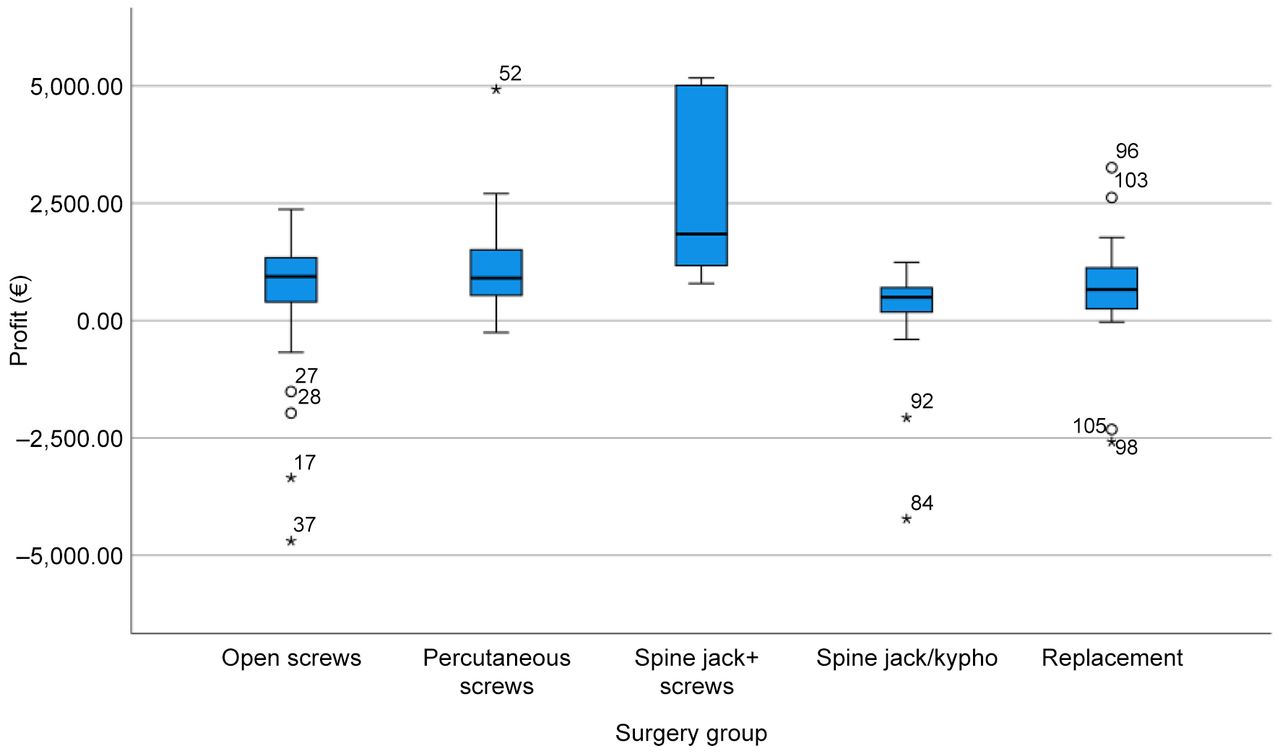
Total profit in groups. Box plot diagram showing profit gained by each group. Surgical intervention with “spine jack+screws” generated highest profit. Number of patients in group “open screws” N=45, “percutaneous screws” N=20, “spine jack+screws” N=6, “spine jack/kypho” N=24 and “replacement” N=34. An analysis of variance was performed. Black bar representing median. Blue bars representing interquartile range between first and third quartile. Whiskers represent data within 1.5×interquartile range. Data falling outside 1.5×interquartile range but within 3×interquartile range are plotted as outliers with a circle. Data falling outside 3×interquartile range are plotted as outliers with a star.
Combination of Spine Jack+screws compared to other for profit per in-patient length of stay.

Profit/inpatient length of stay in groups. Box plot diagram showing profit per day in relation to length of stay for each group. Surgical intervention with “spine jack+screws” generated highest profit per day. Number of patients in group “open screws” N=45, “percutaneous screws” N=20, “spine jack+screws” N=6, “spine jack/kypho” N=24 and “replacement” N=34. An analysis of variance was performed. Black bar representing median. Blue bars representing interquartile range between first and third quartile. Whiskers represent data within 1.5×interquartile range. Data falling outside 1.5×interquartile range but within 3×interquartile range are plotted as outliers with a circle. Data falling outside 3×interquartile range are plotted as outliers with a star.

Total profit in anterior fusion (same vs. different case). Box plot diagram showing profit generated by anterior fusion. Anterior fusion in the same inpatient stay was compared to anterior fusion with a delay of few weeks in a different case. No significant difference was observed. Number of patients in group “replacement same case” N=12 and in group “replacement different case” N=22. An analysis of variance was performed. Black bar representing median. Blue bars representing interquartile range between first and third quartile. Whiskers represent data within 1.5×interquartile range. Data falling outside 1.5×interquartile range but within 3×interquartile range are plotted as outliers with a circle. Data falling outside 3×interquartile range are plotted as outliers with a star.

Profit/length of stay in anterior fusion (same vs. different case). Box plot diagram showing profit per day in relation to length of stay regarding anterior fusion. Anterior fusion in the same inpatient stay was compared to anterior fusion with a delay of few weeks in a different case. No significant difference was observed. Number of patients in group “replacement same case” N=12 and in group “replacement different case” N=22. An analysis of variance was performed. Black bar representing median. Blue bars representing interquartile range between first and third quartile. Whiskers represent data within 1.5×interquartile range. Data falling outside 1.5×interquartile range but within 3×interquartile range are plotted as outliers with a circle. Data falling outside 3×interquartile range are plotted as outliers with a star.
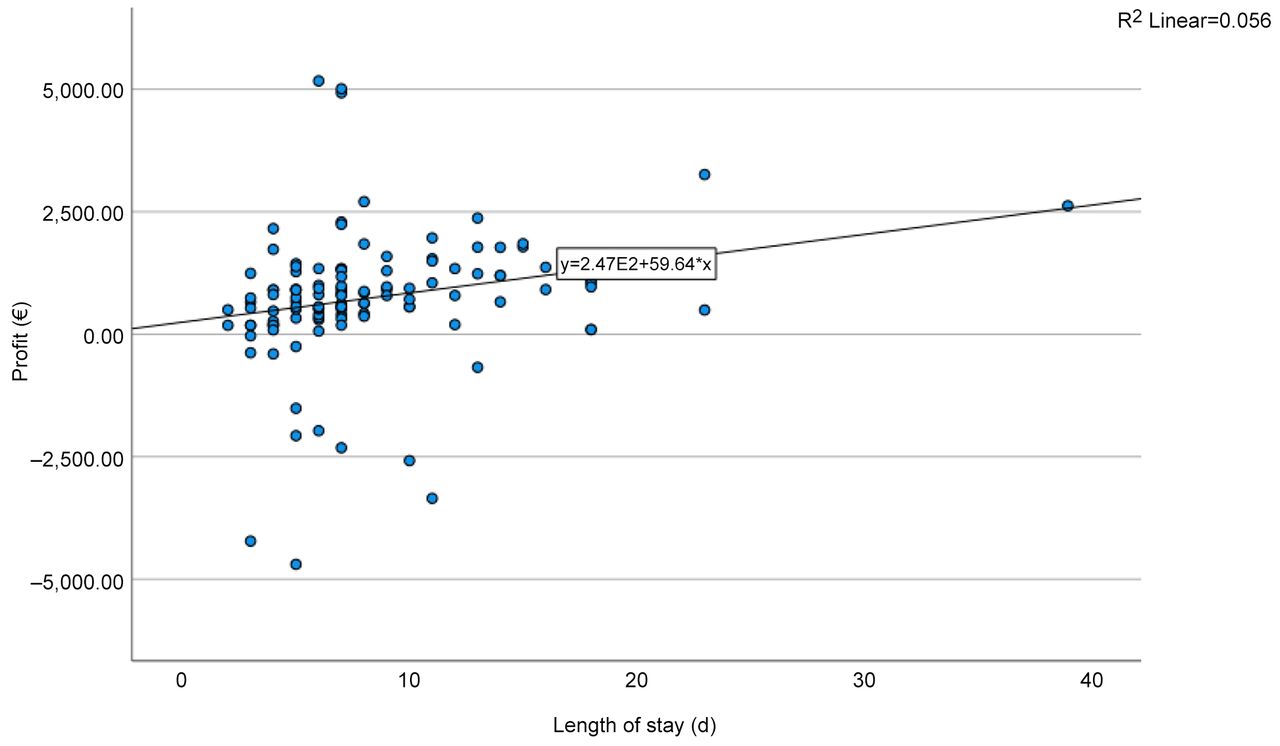
Correlation analysis. The profit correlated weakly positively with the inpatient length of stay when including all groups together (p=0.009, 95%CI=15.12-104.16) (Figure 9), whereas age had no impact (p=0.408, 95%CI=−22.20-9.09) (Figure 10).
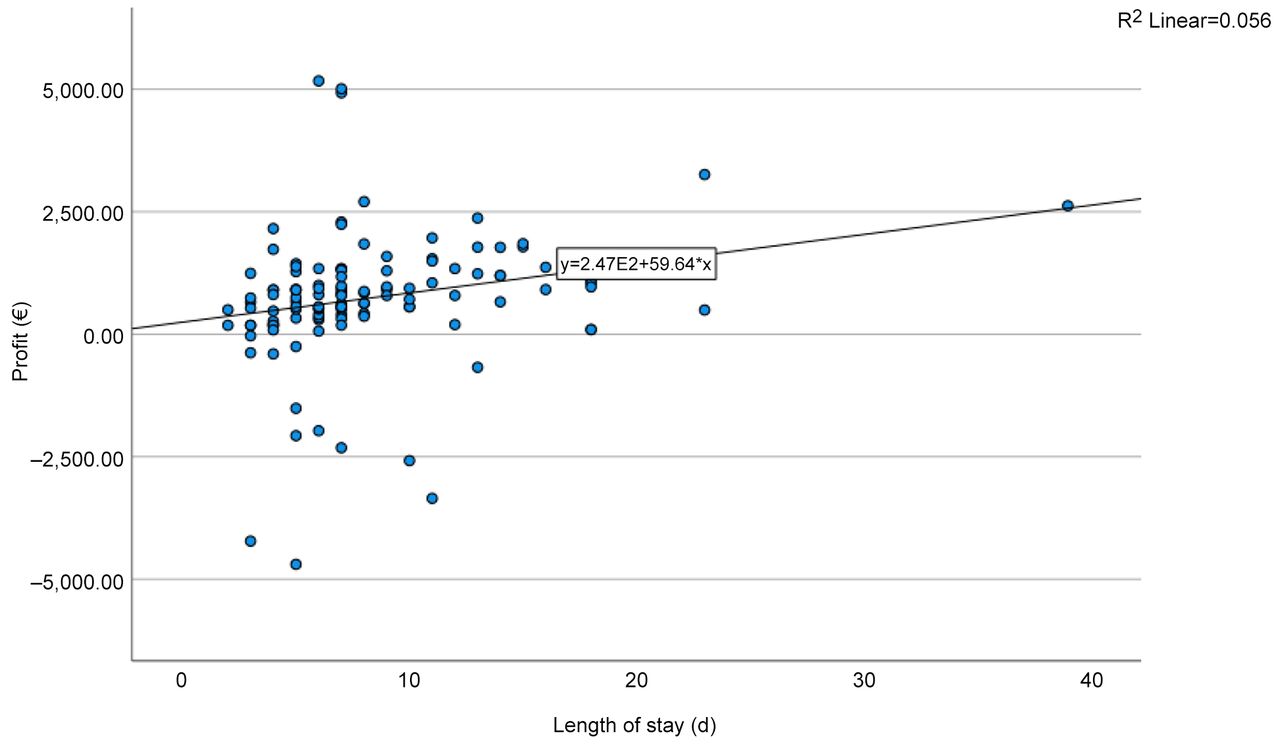
Correlation of profit for inpatient length of stay. Scatter plot diagram showing correlation between length of stay and generated profit. Patients of all groups were included (N=129). Profit correlates weakly positively with the inpatient length of stay. An analysis of variance was performed.

Correlation of profit for age. Scatter plot diagram showing correlation between age of patients and generated profit. Patients of all groups were included (N=129). No correlation between the age and the profit could be observed. An analysis of variance was performed.
Discussion
For the treatment of AO type A3, no consensus exists regarding the optimal surgical technique. A surgeon can choose between different options such as open pedicle insertion, minimal-invasive percutaneous pedicle screws, kyphoplasty or SpineJack®, combined implantation of percutaneous pedicle screws and SpineJack® or vertebral body replacement. To the best of our best knowledge, there is no study focussing on economic aspects of different surgical techniques for the treatment of incomplete burst fracture (AO type A3). Therefore, we analysed 129 patients retrospectively, who underwent surgery due to a thoracic or lumbar AO type A3 fracture in a level I trauma centre from 2008 to 2020 in Germany.
Sole application of kyphoplasty or SpineJack® achieved the smallest postoperative correction of sagittal cobb angle, albeit not significantly. Coincidentally, the average age in this group was the highest (Figure 2), since this technique was not used in younger patients. Our result regarding postoperative correction correlates with a study by Wen et al. (34), where pedicle screw fixation led to higher restoration of vertebral body height in comparison to percutaneous kyphoplasty. However, in the radiological follow-up after 24 weeks, all surgical approaches suffered a loss of correction, and no significant difference could be detected. Wild et al. compared minimally invasive percutaneously and conventionally open posterior stabilized patients and showed that after 5 years, the loss of correction did not show any significant difference (35). Our findings correspond with the literature and suggest that no surgical technique for the therapy of incomplete burst fractures in comparison to each other shows any superiority regarding radiological outcome. However, it has to be noted that in our study, only polyaxial screws were implanted. The use of monoaxial screws could have led to better correction results.
Regarding economic aspects of the various surgical approaches, insertion of percutaneous screws in combination with SpineJack® earned significantly higher profit compared to open surgery, vertebral body replacement, and sole application of kyphoplasty or SpineJack®. Even the profit per inpatient length of stay was around 300 Euro per day, significantly higher in the group of combined percutaneous screws and SpineJack® in comparison to the other interventions (over 10 times higher in contrast to sole application of kyphoplasty or SpineJack®) except for percutaneous pedicle screws. However, a mismatch of the group sizes has to be considered, since only 6 patients underwent percutaneous implantation of screws in combination with SpineJack®. Furthermore, 1 of the 6 patients had to be treated in an intensive care unit due to a nosocomial pneumonia. This prolonged treatment on the intensive care unit could greatly distort the mean profit and profit per day of hospital stay of this group. If the profit was correlated with the age or the length of hospital stay of the patients, no dependence was found for the profit amount regarding patient’s age, whereas the length of stay had a small influence on the profit. The data, this study is based on, showed that the amount of profit is mainly influenced by the surgical procedure.
When assessing the patients with vertebral body replacement, in our cohort a single-stage approach did not gain significantly less profit as a two-stage approach (6 weeks interval between both operations). Even profit per length of stay did not show any differences between these two procedures. This could indicate that performing both operations in one hospital stay is economically equivalent with the two-stage approach, while sparing the patients a second hospital stay and reducing logistical difficulties.
Therefore, our findings suggest, that from a financial point of view, in AOS type A3 fractures of the lumbar or thoracic spine, the application of percutaneous screws in combination SpineJack® may be economically the best method for treatment with similar radiological outcome compared to other surgical approaches. However, combined procedure with percutaneous screws and SpineJack® cannot be recommended as a standard for AO type A3 fractures, since no other outcome parameters besides the sagittal cobb angle were evaluated and no functional outcome parameter was assessed. Furthermore, the sample size in the study was low and the different groups were asymmetrically matched, with the group of combined percutaneous screws and SpineJack® having the lowest number of cases.
Limitations
One limitation of this study is the small sample size with only 129 patients. Furthermore, this study design is only retrospective and monocentric. Due to a moderate compliancy, data histories could not be obtained without gaps for all parameters. An additional limitation is the asymmetric distribution of the group sizes. Only 6 patients underwent percutaneous implantation of screws in combination with SpineJack®, whereas 45 patients were treated open, 20 underwent percutaneous surgery, 24 received sole application of kyphoplasty or SpineJack®, and 34 patients received vertebral body replacement. Since 1 of the 6 patients had to be treated in an intensive care unit due to a nosocomial pneumonia, a distortion of the results regarding economic parameters of this group cannot be excluded.
Conclusion
This study may implicate, that the minimal-invasive implantation of percutaneous screws in combination with SpineJack® gained significantly higher profit and profit per day hospital length of stay compared to implantation of open pedicle screws, vertebral body replacement, and sole application of kyphoplasty or SpineJack®. This finding is independent of the patient’s age. Regarding radiological loss of correction after 24 weeks, we could not detect any differences among the various surgical approaches. However, the minimal-invasive implantation of percutaneous screws in combination with SpineJack® cannot be recommended as the optimal procedure for the surgical treatment of AO type A3 fractures, since this study only aimed to investigate the cost and profit of various surgical approaches without analysing other important clinical outcome parameters. Decision-making for surgery should follow clinical consideration and not financial aspects alone. In addition, costs for implants and hospital stay are different for each clinic or company depending on consumption and manufacturer, wherefore economic advantage of minimal-invasive implantation of percutaneous screws in combination with SpineJack® may be subject to regional characteristics. Furthermore, cemented augmentation techniques are still regarded as controversial in most European countries, since no long-term and clinical functional data are available. Additionally, the single-stage approach of vertebral body replacement gained similar profit and profit per day length of hospital stay in comparison to the two-stage approach. For smoother logistic and to reduce discomfort for the patient, in our clinic we recommend performing both operations during the same hospital stay. However, the decision for a surgical treatment option must not be solely based on economic aspects. Therefore, prospective and randomized trials evaluating functional data and long-term outcome are needed to elucidate these different surgical approaches further.
Acknowledgements
We acknowledge support by the German Research Foundation (DFG) and the Open Access Publication Fund of Hannover Medical School (MHH). Part of the data was collected by the senior author for the master thesis of the MHBA program (Master Healthcare Business Administration, Friedrich-Alexander-University Erlangen Nürnberg). An abstract of this work is submitted for a poster presentation at the German Congress of Orthopedics and Traumatology 2022.
Footnotes
Authors’ Contributions
Niemann, Omar Pacha, and Stübig contributed to the conception and design of the study. Niemann and Clausen organized the database. Omar Pacha performed the statistical analysis. Niemann and Mommsen wrote the first draft of the manuscript. Niemann, Omar Pacha and Graulich wrote sections of the manuscript. All Authors contributed to manuscript revision, read, and approved the submitted version.
Conflicts of Interest
The Authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
- Received June 26, 2022.
- Revision received August 28, 2022.
- Accepted September 1, 2022.
- Copyright © 2022, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.