


Abstract
Background/Aim: Canonical burr-hole craniostomy (BHC) with drainage is the primary treatment for chronic subdural hematomas. However, complicated situations such as organized clots or compartmentation may result in recurrent chronic subdural hematoma (CSDH). Herein, we introduce a novel technique by applying an endoscope for tearing the inner membrane and septum, in addition to evacuating the hematoma in the subdural space where in-line visualization is not possible. Patients and Methods: Two hundred and twenty-nine cases of CSDH were enrolled in this study. Of these, 13 patients were treated endoscopically. The 0-degree and 30-degree, 2.7 mm endoscope was applied after a BHC. The arachnoid knife for microsurgery was used to tear the inner membrane to open the compartments. Results: Non-endoscope-assisted operated (non-Endo group) and endoscope-assisted membranectomy patients (Endo group) demonstrated no differences in sex, age, body mass index, trauma, other diseases, or use of anticoagulation agents. Although the surgery time spent for the Endo patients was longer (128.53±49.56 min) than that for the non-Endo group (65.18±32.89 min), no recurrence was found among the Endo group, whereas a higher rate was observed in the non-Endo group. Conclusion: Novel endoscope-assisted membranectomy is a powerful technique capable of reducing recurrence and improving surgical outcomes.
- Burr hole craniostomy with drainage
- chronic subdural hematoma
- endoscope-assisted membranectomy
- body mass index
- endoscopic transsphenoiolal approach
Subdural hematomas are classified into acute, subacute, and chronic according to the total duration of symptoms (1), with chronic subdural hematomas (CSDH) being the most prevalent type and symptomatically mimicking other disease entities. Globally, the incidence of CSDH is approximately 13.5 per 100,000 persons less than 65-years-old per year; 58 per 100,000 persons of the population 65 years old or older. More importantly, it is approximately five times higher among patients with CSDHs older than 65 years than CSDH patients of less than 65 years (2, 3). In Asia, CSDH is typically caused by minor head trauma (approximately 50%) and occurs predominantly in males around the age of 65 years (4). Two common mechanisms have been proposed in which blood or fluids accumulate within the dura cell layers or at the borders between the dura layers. The most typical mechanism involves a head trauma, which causes tearing of bridging veins within the involved subdural space (5). Another theory suggests that microbleeds are produced between the dura mater and arachnoid membrane, forming neo-membranes 3-4 weeks after a brain insult. The inner membrane is thin and avascular, whereas the outer membrane is thick and rich in fragile blood vessels (neo-membrane) and can be two- or three-layered after repeated episodes of trivial trauma (6). The most complicated situation leading to postsurgical recurrence after burr-hole craniostomy with drainage, abbreviated as (BHC)-D, is the separation or compartmentalization of SDH spaces at different time periods. Symptomatic CSDH frequently requires urgent neurosurgical management. There are several treatment strategies for CSDH, such as twist drill craniostomy, traditional craniotomy, and BHC-D (4). Among these, BHC-D has been the mainstream neurosurgical treatment for CSDH. Symptomatic recurrence has been noted in 2.5% to 33% of post-operative patients and warrants re-exploration or more aggressive craniotomy, which neurosurgeons usually attempt to avoid (2, 7). Radiologically, the double-crescent sign on computed tomography (CT) or magnetic resonance imaging (MRI), namely compartmentation, is a predictor of recurrent CSDH, implying non-liquefaction of CSDH (8). Clinically, it is difficult for neurosurgeons to clean up the arachnoid septum composed of trabecular adhesions and the inner membrane perfectly with simple maneuvers, such as with twist drill craniostomy or BHC-D. Therefore, it is of great value to exploit a novel solution for eliminating the septum and inner membrane to prevent ominous recurrence of CSDH. We believe that endoscope-assisted membranectomy maneuver is more appropriate than BHC-D considering the compartmental restrains of the re-expansion of the compressed brain substance, as other novel techniques such as catheterization and tearing of the inner membrane could eliminate recurrence of CSDH (9).
Patients and Methods
Collection of patients with CSDH. A total of 229 patients with CSDH receiving neurosurgical treatment were recruited from the National Defense Medical Center from July 2016 to June 2020. Among them, forty-eight were bilateral CSDH cases (21.0%), one hundred and three were unilateral left CSDH cases (44.9%), and seventy-eight were unilateral right CSDH cases (34.1%). All procedures were conducted after approval and under the supervision of the Institutional Review Board (IRB) of National Defense Medical Center (IRB number: B202105050).
Non-endoscope-assisted surgery for CSDH. Two hundred and sixteen cases of CSDHs were treated with standardized steps of BHC-D without endoscopic assistance but with surgical loupes or naked eyes. In detail, they were irrigated with warm normal saline or ringer lactate solution into the BHC to decrease osmotic pressure, then placed and closed with a drainage system followed by suction clearance of the residual blood for three-five days. These cases were defined as the non-endoscope-assisted group for CSDH treatment (non-Endo group).
Endoscope-assisted membranectomy for CSDH. Patients with organized clots and compartmentation seen on preoperative CT scans were assigned for endoscope-assisted membranectomy (Endo group). This method was modified from that used by Masopust et al. (10). Thirteen patients were enrolled with informed consent signed by themselves or their family. In this group, we specifically made the personalized burr-hole with an average diameter of 3.5 cm (named as the BHC), at the morphological center of the hematoma island under brain computed tomography. A rigid endoscope (0-degree and 30-degree, 2.7 mm) was used to “circum-illuminate” the residual organized hematoma and performed tearing and splitting of the inner membrane with an arachnoid knife used in microsurgery. Bayonet-shaped microsuctions of 5 and 7 French were reciprocally used to clean the residual clot. Patients were followed-up for six months until July 2021.
Statistical methodology. The Student’s paired t-test was used to compare the distributions of demographic parameters between the non-Endo and Endo groups. Pearson’s Chi-square methodology was used to check the distribution pattern of the other indexes. A p-value of less than 0.05 was considered statistically significant. Analyses were conducted by SPSS software package (IBM SPSS Statistics for Windows, Version 20.0. IBM Corp., Armonk, NY, USA).
Results
Comparison of basic demographic characteristics. The basic characteristics of the 216 non-Endo and 13 Endo patients are summarized and compared in Table I. There were no significant differences (all p>0.05) between the groups regarding age, sex, body mass index, and hypertension. With regard to comorbid chronic disease status, including diabetes mellitus, hemodialysis, and cardiovascular and cerebrovascular diseases, there were no significant differences (all p>0.05). Theoretically, anticoagulant and anti-platelet drugs may increase the risk of CSDH after trivial trauma (11, 12). However, according to our analysis, patients taking anticoagulants did not show a significant propensity to develop future CSDH (p>0.05).
Basic characteristics of 216 non-endoscope-assisted operated patients and 13 endoscope-assisted operated patients.
Comparison of surgical characteristics. The surgical characteristics of 216 non-Endo and 13 Endo patients are summarized and compared in Table II. First, regarding the laterality of the lesion, there was no differential distribution between the two groups (p>0.05). Intracranial pressures (ICP) were recorded in 34.7% of the non-Endo and 30.8% of the Endo patients, and the ICP monitoring showed no significant difference between groups (p>0.05). The surgical time for the Endo group was about two-fold significantly longer (128.54±49.56 min) than that of the non-Endo group (65.18±32.89 min) (p<0.0001). The instrumentation and endoscopic video system settings may be responsible for the time- and effort-consuming preparation for delicate manipulation and postponed the surgical time. Interestingly, the recurrence rate in the non-Endo group patients was 6.5%, whereas the Endo group had no recurrence at follow-up (Table II).
Basic characteristics of 216 non-endoscope-assisted operated patients and 13 endoscope-assisted operated patients.
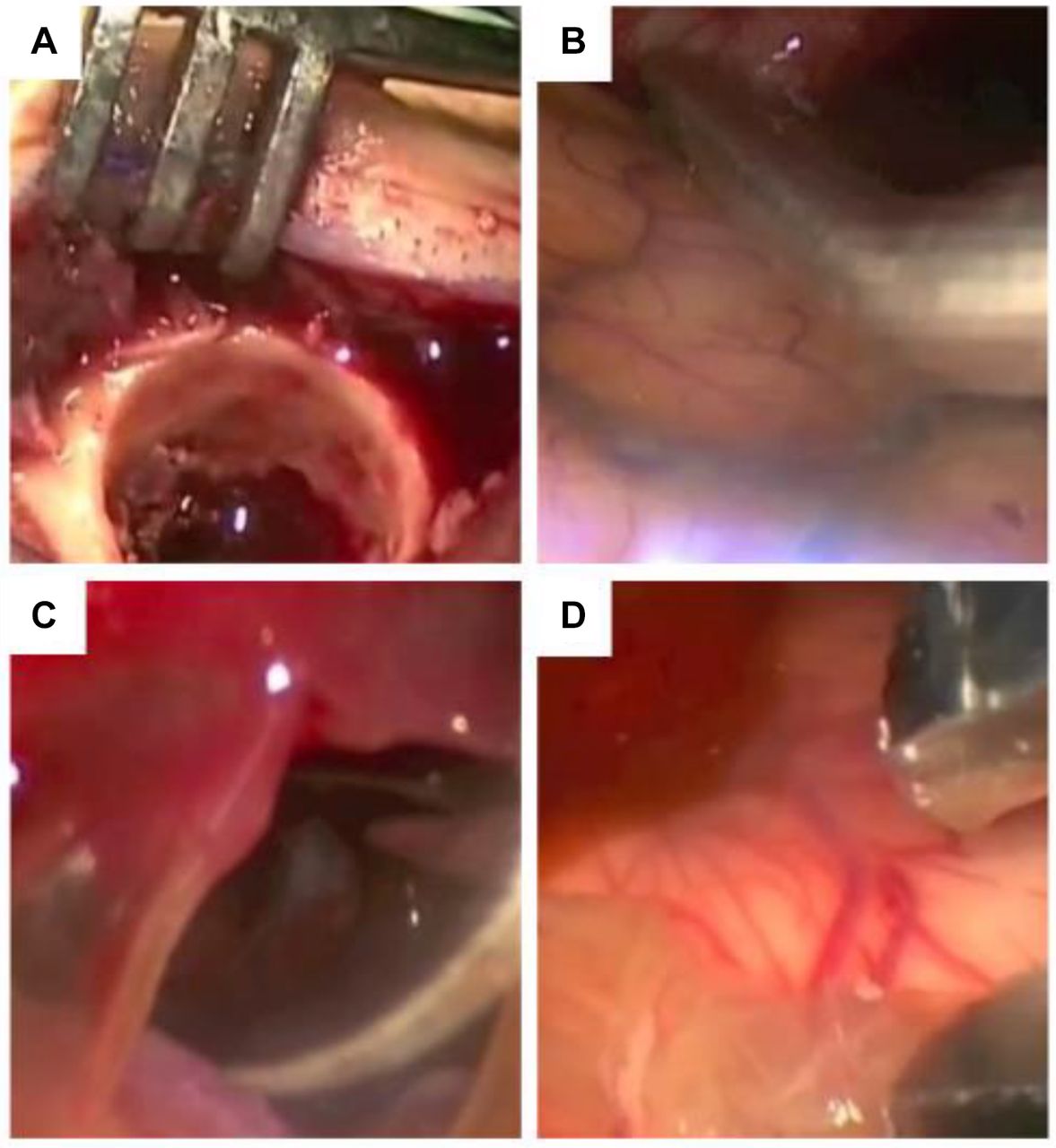
Surgical images were obtained with the assistance of an endoscope. Typical and real-time images acquired using the endoscope are shown in Figure 1. During the endoscopic procedures, a burr hole was made specifically at the morphological center of the hematoma island (Figure 1A). Technically, the temporal base can usually be observed using an endoscope-assisted technique and cannot be visualized using the canonical BHC-D approach. Furthermore, cortical vessels can be vividly observed during the BHC procedure (Figure 1B). As shown in Figure 1C, the septum can be manipulated with an instrument tracking the margins, so that any abnormally organized adhesive separation can be opened up with an arachnoid knife or a bipolar coagulator (Figure 1C). The avascular inner membrane can also be visualized with the assistance of an endoscope, which serves as the main barrier limiting re-expansion of the brain (9) (Figure 1D).

Surgical pictures obtained with the assistance of the endoscope. (A) Typically, an average 3.5 cm burr hole was made specifically at the morphological center of the hematoma island. The figure shows the real image obtained using the rigid endoscope (4 mm, 0 degree). (B) Specifically, the temporal base can only be observed clearly via the endoscope-assisted technique. (C) The abnormally organized septum can be cleared only with the endoscope-assisted technique. (D) Only with the assistant of the endoscope, the inner membrane can be nicely eliminated.
Discussion
For neurosurgeons, unsuccessful treatment usually results in surgical recurrence after CSDH operations (13, 14). The well-known pathophysiology of CSDH indicates that increased osmotic pressure due to fibrinolysis of CSDH leads to hematoma expansion (15). According to the pathophysiology of CSDH, the arachnoid septum or accumulated layered fluid are important factors leading to recurrence. Therefore, the inner membrane and compartment have been the focus of modern surgical treatments for CSDH (16).
Based on the pathophysiology of CSDH formation, outer membrane breakage is not sufficient to avoid CSDH recurrence. However, eliminating the osmotic gradient is the most important factor. Currently, the endoscopic technique prevails over the endoscopic transsphenoidal approach (TSA), and optical technology has enhanced the complete removal of the inner membrane, eliminating the osmotic elevation that leads to recurrence of CSDH. In the current study, in the results of the Endo population, cases of bilateral lesions are lacking (Table II); this may confound or underestimate the recurrence rate. The data indicated that bilateral CSDHs are frequently prone to recurrence, owing to the osmotic imbalance (Table II). Based on our experience, bilateral CSDHs may experience a pressure shift during side-by-side BHC-D. Therefore, we now utilize simultaneous open-up of the outer membranes of bilateral BHC-D, although pneumocephalus remains an issue during post-operative care. We attempted to use one-sided endoscope-assisted membranectomy to pass through the falx cerebri, but in vain, contralateral endoscope-assisted membranectomy was not possible. Hence, we recommend endoscope-assisted membranectomy for one-sided CSDH complicated by septations or compartments. According to the literature, patients on hemodialysis may carry an increased risk of recurrence for CSDH, since the intracranial pressure tends not to be as flexible as that in healthy people according to the Monro-Kellie doctrine (17), whereas our patients on hemodialysis in the Endo group did not show higher recurrence than non-Endo patients (Table I). In addition, it is an unexplainable observation that patients with left-sided CSDH visited our hospital more frequently than patients with right-sided CSDH (Table I). Patients with left-sided CSDH often presented with Wernicke aphasia and were easily identified and sent to hospital. The left site predominance is consistent with previous reports and remains unexplainable and unconcluded (18, 19). One explanation for this may be that the aphasic symptom is more frequently observed by the family than the non-specific presentation of the right-side non-dominant hemisphere. Lastly, taking anticoagulants, such as warfarin or a non-vitamin K antagonist oral anticoagulant (NOAC), may contribute to coagulopathy, leading to chronic inflammation and microbleeding. There is still no solid evidence of the association between anticoagulant agents and CSDH recurrence (20). Neurosurgery for CSDH is relatively emergent, thus it is the best strategy to cut the diagnose-to-treatment time as short as possible (21, 22). Interesting, in the present study, although it seemed to take twice as long to finish the surgery for the Endo group than that of the non-Endo group, the outcome of the Endo group was significantly better than that of the non-Endo group (Table II). The critical point is that the amount of bleeding did not differ between groups. Additionally, surgical complications, such as post-operative acute subdural hematoma and other types of iatrogenic brain damage, did not occur in either group during the patients’ hospital stay. Therefore, we believe that the endoscope-assisted membranectomy maneuver for CSDH provides better outcomes in preventing surgical recurrence, although it may be more time-consuming. Under the National Health Insurance (NHI) system of Taiwan, CSDH patients should be encouraged to undergo endoscope-assisted membranectomy to reduce the risk for recurrence, which also reduces medical expenses. In the current study, we propose an improved method rather than the typical BHC-D method by adopting variable-angled endoscopes to lower the recurrence rate. The preliminary results in Table II show that 13 Endo patients of CSDH were recurrence-free for at least 4 years (Table II). The age and sex ratios are in accordance with the literature published in Asia and other countries (4). However, one limitation is the sample size of the Endo group, and thus studies with higher numbers of patients are urgently required.
Conclusion
Evidence from 229 cases, including Endo and non-Endo patients, suggests the novel incorporation of the endoscopic technique into canonical CSDH to enhance the capacity of separating the septum and inner membrane more efficiently. Emerging endoscope-assisted manipulation is worth validating for its clinical value in modern neurosurgical practices.
Acknowledgements
The Authors thank all patients who participated in the study and the experts who provided their expertise and comments. The help of nurses and colleagues is highly appreciated by all Authors.
Footnotes
Authors’ Contributions
Conceptualization: Hong KT, Tang CT; Data curation: Hong KT, Hsu SW, Chen CH; formal analysis: Hong KT, Hsu SW, Chen CH; Investigation: Hsu SW; Methodology: Chen CH; Project administration: Hueng DY; Resources: Hueng DY, Chen YH, Ju DT, Tang CT; Supervision: Hueng DY, Chen YH, Ju DT, Tang CT; Validation: Tang CT; Writing the original draft: Hong KT, Tang CT, Bau DT; Review and editing: Hong KT, Tang CT, Bau DT.
Conflicts of Interest
All the Authors declare no conflicts of interest regarding this study.
- Received September 16, 2022.
- Revision received September 30, 2022.
- Accepted October 5, 2022.
- Copyright © 2022, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.