


Abstract
Background/Aim: With a rapidly growing number of studies, systematic reviews (SRs) and meta-analyses (MAs) on acupuncture, the level of evidence seems to be high. Yet, traditional Chinese acupuncture is built on concepts which are not in accordance with science-based medicine. Accordingly, our aim was to critically assess the evidence presented in SRs and MAs on xerostomia induced by treatment of head and neck cancer with radiotherapy. Materials and Methods: In February 2022, a systematic search of five electronic databases (Embase, Cochrane, PsychInfo, CINAHL and Medline) was conducted to find SRs/MAs on acupuncture use against cancer-treatment induced xerostomia. We evaluated all SRs/MAs using the AMSTAR instrument, comparing the assessment of the individual studies included and the conclusions drawn by the authors. In case of heterogeneity between the SRs, we evaluated the controversial items of the assessments directly from the studies. Results: Finally, eight SRs/MAs were included. Most of them show methodological drawbacks in several domains of the AMSTAR instrument, which influences the credibility of the results. Conclusion: The evidence on the use of acupuncture as treatment for radiotherapy-induced xerostomia is low. Present SRs/MAs mainly summarize results of a few and mostly small studies. Even though the included studies greatly overlap, the quality of the presentation and interpretation of the authors differs greatly. Therefore, a high quality and conclusive summary of the present evidence on the use of acupuncture to treat radiotherapy induced xerostomia is still missing.
- Systematic review
- meta-analyses
- acupuncture
- methodological evaluation
- complementary medicine
- neoplasm
- review
Acupuncture is a highly controversial topic in complementary medicine. Being an ancient Traditional Chinese Medicine (TCM), it is founded on concepts of health and disease, which have been passed by modern medicine. A central part of this concept is the flow of Qi (energy) in meridians on which there are special points (acupoints) where needles may be inserted to redirect the flow of Qi. Needles inserted may be manipulated manually, electrically or by heat, to tonify, strengthen or reduce Qi dependent on the individual’s deviation from the balanced flow, which led to the disease or problem. From a Western scientific point of view, neither Qi nor meridians or acupoints exist. Furthermore, also the ancient concepts of diseases within the TCM have been overcome by modern understanding of pathologic processes. Nevertheless, acupuncture is attractive for patients and physicians, offering an individualized treatment plan, which often is called holistic treatment of the human being as a whole and not only the disease.
Many varieties of acupuncture have been added including western style acupuncture, acupuncture of the ear, hand or tongue, and electro-acupuncture. Furthermore, acupuncture has been combined with the injection of homeopathic products and others.
Despite the scientific concerns on these methods, many people, including patients and physicians had positive experiences using acupuncture, which is widespread in the treatment of pain. Also in cancer care, acupuncture is propagated and the German S3 guideline on complementary oncology (1) includes several recommendations on acupuncture based on the rapidly growing number of studies, systematic reviews (SRs) and meta-analyses (MAs). Acupuncture is especially attractive to treat side effects of cancer treatment for which standard treatments do not exist or are not as effective as hoped for by the patients. This is the case in neurotoxicity, nausea, pain or xerostomia.
It is still unclear if and how exactly acupuncture may influence xerostomia. Yet, there are hypotheses addressing how acupuncture could increase saliva secretion. Research showed that the functions of the salivary glands are controlled by both the sensory and autonomic nervous systems, while the parasympathetic system exerts the most main influence on the salivary secretion (2-4). It is postulated, that acupuncture could stimulate the parasympathetic and sympathetic nervous systems through neuronal activation (5-7), which then causes the release of neuropeptides, such as vasoactive intestinal peptide and calcitonin gene-related peptide (7). These neuropeptides have anti-inflammatory properties and nutritional effects on the salivary glands and increase the blood flow in the acini.
Both, physicians and patients put high expectations in acupuncture, which may lead to a strong placebo-effect on both sides. For the planning of studies, intervention, control group, randomization, blinding of participants and acupuncturists is crucial. Blinding for the insertion of a needle is hardly possible. Yet, so-called sham-acupuncture either uses sham needles which do not penetrate the skin or sham acupoints which are not related to meridians or are far away from points normally used in the specific situation. Neither a blinding of patients nor physicians is efficacious possible. Blinding remains controversial regarding any design or interpretation of acupuncture studies.
For most physicians and even for most scientists, the ever-growing pool of evidence is hardly accessible. As a result, SRs and MAs formally providing level I evidence are often referred to for treatment decisions, recommendations in guidelines as well as decisions in a health care system.
With a growing number of formal level I evidence, the lack of evidence in the studies summarized in those SRs and MAs may be overlooked. Moreover, the trustworthiness of the SRs and MAs becomes highly important, as most probably no reader assesses the selection and evaluation of the single studies included but only the formal comprehensiveness of the reporting and analysis as, for example, the flowchart of study selection and the risk of bias assessment.
To get a deeper insight into the reliability of SRs and MAs, we chose a well-defined symptom for which standard care is rather ill-defined and has low effectiveness: Dry mouth induced by treatment of head and neck cancer. Xerostomia may be assessed in a study using subjective (self-assessment by the patient) as well as objective (salivary flow rate) instruments.
Materials and Methods
Search strategy and selection of SRs and MAs. A systematic search was conducted in February 2022 using five databases (Medline (Ovid), CINAHL (EBSCO), EMBASE (Ovid), Cochrane CENTRAL and PsycINFO (EBSCO)). For each of these databases a complex search strategy was developed consisting of a combination of MeshTerms, keywords and text words in different spellings connected to cancer, acupuncture therapy and xerostomia (Table I). There was no restriction to the type of cancer. After importing the search results into EndNote X9, all duplicates were removed, and a title-abstract-screening was carried out by two independent reviewers (JD/MF). Inclusion and exclusion criteria are based on a PICO-model (details may be obtained from the authors). We included SRs, which included mainly RCTs and used at least 2 databases with a predefined systematic search method.
Search strategy.
In case of disagreement, consensus was reached by discussion, or a third review author was consulted (JH). When title and abstract did not have sufficient information for screening purposes, the full text copy was retrieved as well. After that, all full texts were retrieved and screened again independently by both reviewers (JD/MF). Additionally, bibliography lists of all retrieved articles were searched for relevant SRs.
For this article, we compared the results of the assessment of the individual studies in the different SRs with our results.
Assessment of risk of bias and methodological quality of the SRs. All characteristics were assessed by two independent reviewers (JD/MF). In case of disagreement a third reviewer was consulted (JH) and consensus was reached by discussion.
The risk of bias (RoB) was analyzed with the AMSTAR-2 instrument for SRs or meta-analyses (8). In addition, comprehensiveness of presentation of results and included studies, consistencies between protocol and article, use of established methods for data extraction and rating of RoB, adequacy of statistical tests and calculation of meta-analysis (MA) and selective outcome reporting were assessed.
Additionally, we thoroughly assessed all studies included with respect to additional aspects which may lead to bias and compared our results to those from the SRs/MAs.
Results
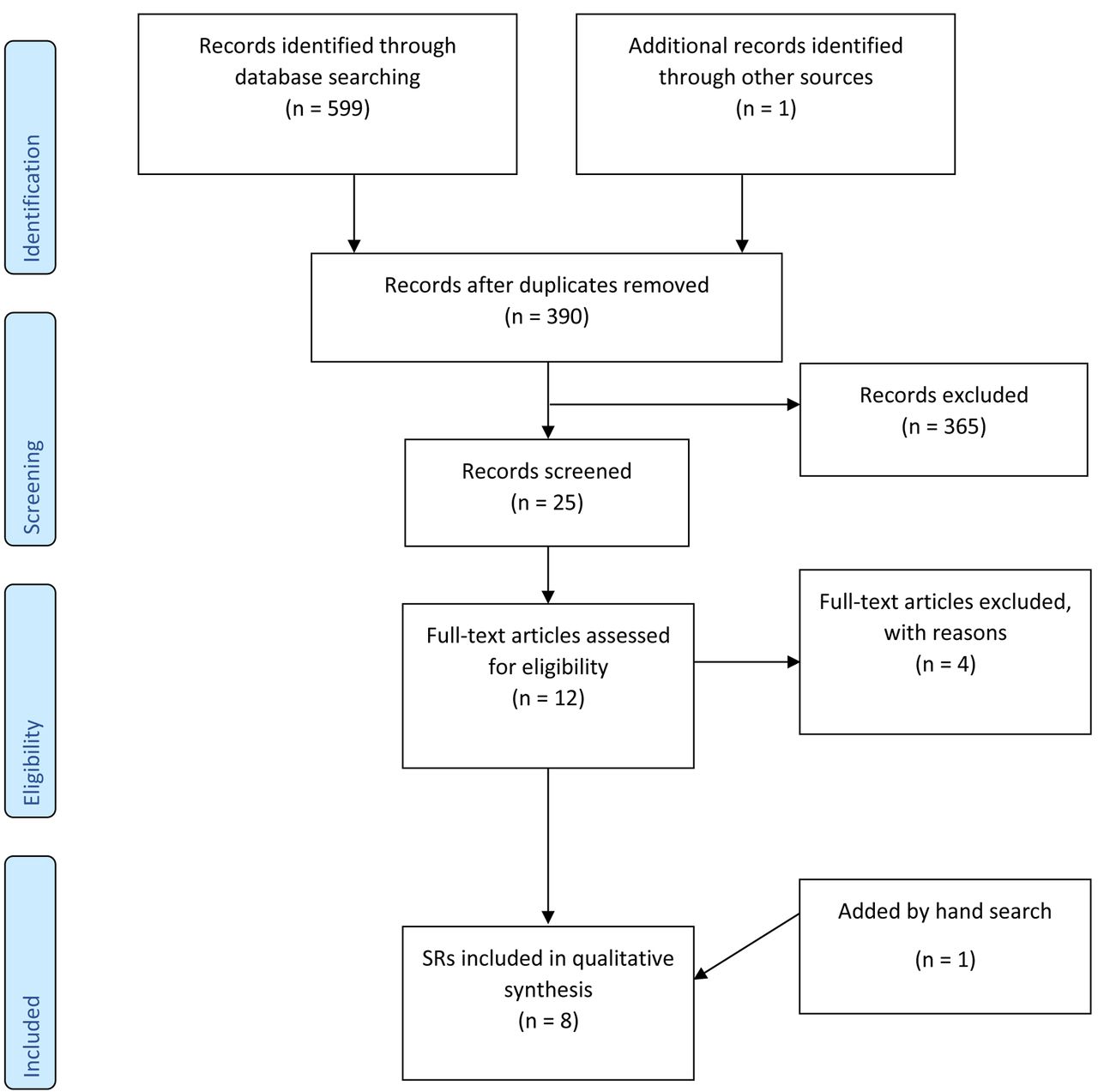
Characteristics of included SRs. The systematic search revealed 599 results. One SR was added by hand search. At first, duplicates were removed leaving 390 publications. After screening title and abstract, 25 SRs remained to complete review (Figure 1). Finally, eight SRs, with 12 different controlled studies were included. One of these controlled studies was excluded, because it measured dysphagia (9). Additionally, 1 controlled study was included by hand search (10). The study by Braga (2011), included by Assy et al. (2018), Ni et al. (2020) and Bonomo et al. (2021) (11-14), was considered an RCT by Ni et al. (2020) and Assy et al. (2018), while it was considered a prospective cohort study by Bonomo et al. (2021). As the authors of the study clearly stated (“patients were assigned”), no randomization process took place.

Consort diagram. SRs: Systematic reviews.
We therefore included eight SRs with 10 RCTs and one CT, as well as one additional RCT as relevant. Detailed characterization of the included SRs can be seen in Table II (A detailed overview of the PICO criteria of the SRs may be obtained from the authors).
Characteristics of included systematic reviews (SRs).
Excluded SRs. We excluded four SRs in the full-text screening, due to no including RCTs (15), being an update of an already included SR with no new RCTs (16) or the authors only searched one database (17, 18) (A list of excluded SRs may be obtained from the authors).
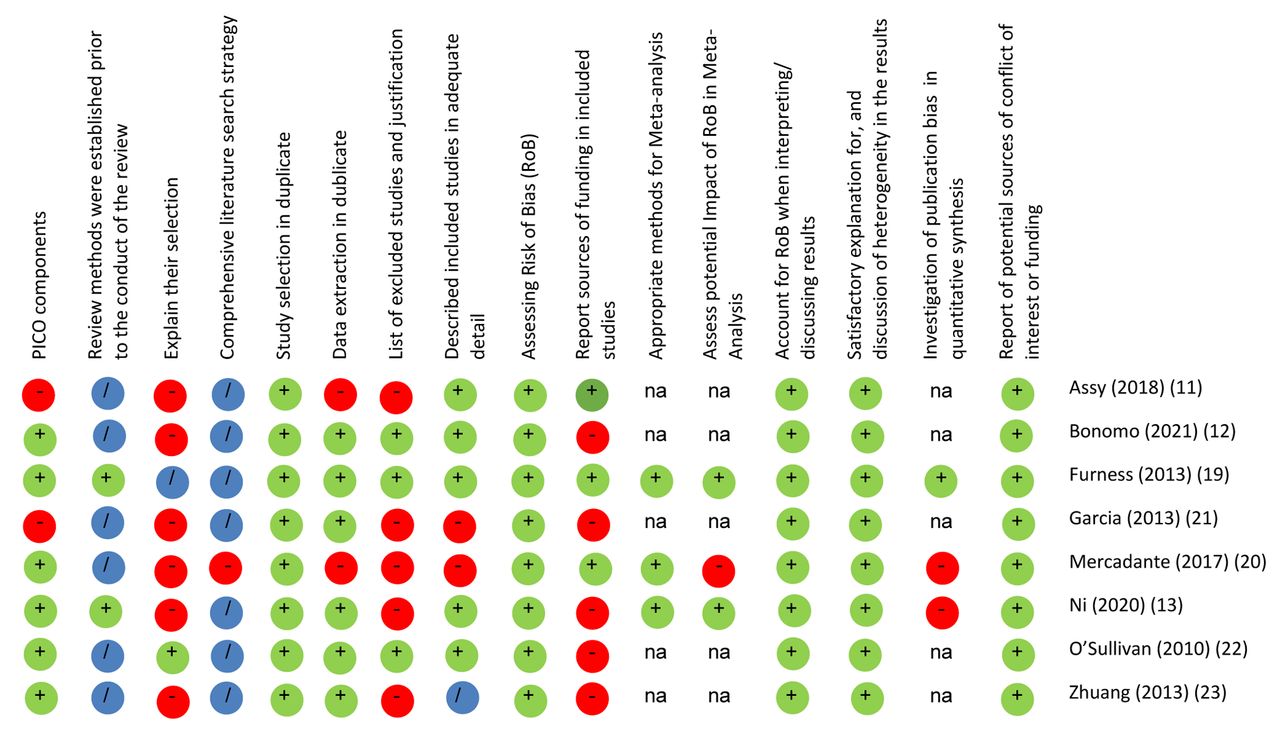
Quality of the included systematic reviews. The methodological quality was assessed with the AMSTAR-2 instrument for SRs or meta-analyses (8). The AMSTAR contains 16 items, covering the most important quality aspects in an SR. Only three out of the eight included SRs conducted a MA and could therefore be assessed in this category (Item 11, 12, and 15). Except for one (19), all SRs showed deficiencies in at least one domain of the AMSTAR-2, with one showing deficiencies in seven domains (20). An overview of the methodological assessment can be seen in Figure 2.

Methodological assessment of included systematic reviews (SRs). +: Yes; −: no; /: partial yes; na: not applicable.
Reporting of PICO criteria and protocol deviations. Except for two, all included reviews described the inclusion criteria according to the PICO-model. Garcia et al. (2013) and Assy et al. (2018) failed to describe the inclusion criteria for the comparison groups in the method section but describe the included comparison groups in the results section (11, 21). Two reviews had a registered protocol in PROSPERO (13, 19), even though we were not able to find the protocol of Furness et al. (2013) online. The review by Mercandante et al. (2017) stated to have developed a protocol, but there was no link in the article, and we were not able to find it online (20). Furthermore, Ni et al. (2020) deviated from their protocol. In the published article, they reported searching eight databases instead of 11, they did not search in trial registers for further studies and most important, they changed the search string, adopting a shorter and less precise than the one planned (13).
Reporting of study selection, search strategy and a list of excluded studies. Only one SR gave an explanation why they exclusively included RCTs (22). All but Mercandante et al. (2017) (20) presented the full search string (13, 19), gave the information to send the full string on request (22) or gave the terms they used (11, 12, 21, 23). Still, none of the SRs fulfilled all criteria to entirely comply with this AMSTAR-item. Drawbacks included not conducting further searches in reference lists (21, 22), grey literature (or explain, why this is not necessary) (11-13, 19-21, 23), in trial/study registers (11, 12, 20-23) or not contacting experts in the field (11-13, 19-23).
Only two SRs provided a list of excluded studies after the full-text screening (19, 22), while one cites the excluded studies in the description of the method section (12). Most SRs only mentioned the number of studies excluded and reasons for exclusion in the text but did not list the respective references (11, 13, 21, 23) and Mercandante et al. (2017) gave information in the text (20). The SR by Bonomo et al. (2021) shows inconsistencies in the description in the text to the reasons for exclusion in the flowchart. Furthermore, the flowchart indicates that additional records were found through Embase, even though Embase was prior stated as one of the used databases in the method section (12).
Reporting of study selection and data extraction in duplicate. Except for Bonomo et al. (2021), all included SRs stated a study selection by two authors. Two reported that a disagreement in study selection was solved by discussion or with a third reviewer (13, 23), while Assy et al. (2018) and Furness et al. (2013) only reported the option of discussion (11, 19). The information in Bonomo et al. (2021) for study selection is unclear (12).
Besides Assy et al. (2018) and Mercandante et al. (2017) (11, 20), all SRs stated a process for data extraction by two independent authors. Three SRs also stated that a third reviewer was consulted in case of disagreement (12) or that a third reviewer was consulted for discussion of the data tables after they were compared between the two extractors (13, 23). Furness et al. (2013) stated the possibility of discussion in case of disagreement (19). No information was given for the process of disagreement in Mercandante et al. (2017), Garcia et al. (2013) and O’Sullivan et al. (2010) for both study selection and data extraction (20-22).
Reporting of study characteristics and heterogeneity in the studies. Five SRs described the studies included (population, interventions, comparator groups, outcomes, study design) in adequate detail (11-13, 19, 22). While three SRs gave insufficient information on the population (20, 21, 23), intervention or comparison group (21) and one gave most of the information about the studies in text-form, but in a rather uncomprehensive way (12).
Furthermore, they discussed or tried to explain the heterogeneity between the studies. Even though Garcia et al. (2013) does only mention heterogeneity briefly, most of the others got more into detail (21). Mercandante et al. (2017) stated in their protocol, how they wanted to assess the heterogeneity of the studies, but no information on that is given in the article (20).
Reporting of study design, intervention, and control group. Extraction tables. To best compare results from different studies, it is desirable to use a standardized approach to extract the data presented in the publications. Due to the heterogeneity and complexity of acupuncture, an extraction providing a detailed insight into the acupuncture intervention and the control group is necessary to analyze, compare, and aggregate data from different studies. The STRICTA checklist (Standards for Reporting Interventions in Controlled Trials of Acupuncture (24) includes the framework of the intervention (type, control/comparator group as well as the background of the practitioner), a structured way to extract the methods and results, as well as methodological components and further information, like funding. Even though a now revised version was already available since 2011, only three of the included SRs used this checklist (13, 22, 23).
Intervention and control group. All SRs included studies which either used usual care/oral hygiene education (11-13, 19-23) or sham acupuncture (either non-penetrating needling at acupoints or needling at non-acupoints) (11-13, 19, 20, 22, 23) as comparators.
None of the included SRs mentioned the different types of acupuncture in the presentation of the results. Except for Furness et al. (2013) (19), all SRs report that there are differences between the techniques used in the studies and all but two (11, 21) report detailed information on the acupuncture techniques used in the studies, including acupuncture points, type of acupuncture and duration in the characteristics of the studies. Yet they all fail to differentiate them in the reporting of the results.
An overview of the presentation of results can be seen in Table III. Garcia et al. (2013) only presented results of two out of four studies they included, but estimated effect sizes for them (21).
Comprehensive presentation of results.
Reporting of endpoints. Except for Garcia et al. (2013) (21), all SRs differentiate between subjective and objective measurement when presenting the results. However, an interpretation of these in relation to an open design or missing blinding in one party is mostly missing.
Quality of meta-analyses. Five SRs concluded that because of this given heterogeneity an MA is not applicable (11, 12, 21-23). Only three SRs conducted an MA, of which Mercandante et al. (2017) stated that only summary data rather than patient level data were available (20), Ni et al. (2020) excluded a study in the MA because no original data was available (13), while Furness et al. (2013) gave no information on that matter (19). All three used aggregated data from the studies and not individual patient data. For only one MA, using the STRICTA Checklist (24), a differentiated approach considering the different types of acupuncture, was planned but not realized in the MA (13).
Only Ni et al. (2020) and Furness et al. (2013) discussed the likelihood of impact of the RoB on the results (13, 19). While Mercandante et al. (2017) gives no information on the attempt to account for a possible publication bias (20), Ni et al. (2020) explains that they were not able to conduct a funnel plot, due to the limited number of included RCTs and therefore concluded, that a publication bias might exist (13). Furness et al. (2013) stated that they wanted to conduct an analysis for publication bias if more than three studies were included in the MA, which was not the case (19).
It remains unclear which criteria did qualify a study to be included in the MA, even though Ni et al. (2020) only included low risk RCTs (13). Mercandante et al. (2017) and Furness et al. (2013) only stated that they included studies which “provided enough data” and “suitable data”, but it remains unclear how this was defined (19, 20). Both MAs included studies with a high risk of bias.
Furthermore, it’s unclear why Mercandante et al. (2017) used an older version of the Cochrane Tool, since the 5.1.0 Version was already available and widely used at the time, they conducted their SR (20). It should be noted that the 5.1.0 Version of the Cochrane Tool has been updated in 2021 (RoB2: Revised Cochrane Risk of Bias Tool for RCTs) and is now more differentiated than the older Versions (especially in separating domains of blinding).
All three MAs differ in their analysis of heterogeneity, which impacts the interpretation of the results. Since Mercandante et al. (2017) found no heterogeneity between the studies the studies may be very similar, and an average effect is interpretable. But Ni et al. (2020) found a heterogeneity of at least 60%, which indicates that the studies indeed do differ, and an average effect should be interpreted with caution. Furthermore, in both MAs the weight of the included studies differs, which further raises the question on how exactly the MAs were assessed and gives reason to doubt the comparability of results between analyses of SRs.
Assessment of risk of bias (RoB). All included SRs used an established method to assess the RoB. In Table IV, all assessments of methodological quality of the included studies are listed in detail. All but one SR used the Cochrane Assessment tool, either the old version from 2008 (21) or the version 5.1.0 from 2011 (11-13, 19, 20, 23). O’Sullivan et al. (2010) used the NHS Critical Appraisal Skills Program (CASP) (22). However, the results of the RoB assessments of the individual studies are very different. All included SRs accounted for the potential impact of the RoB while interpreting/discussing the results.
Risk of bias (RoB) assessment by systematic reviews (SRs) of included single studies (categories in detail see Table V).
Yet, while comparing the results of single studies in different SRs, the high heterogeneity in the rating of all domains of RoB are impressive. In fact, there is no domain with a homogenous assessment. Moreover, the spread between the assessments includes two grades (red to green) for any study with more than one assessment.
Selection bias. Taking a deeper look at the differences in the RoB assessment (Table V), it becomes obvious that for each domain, the authors did not include all aspects listed in the RoB 2.0 version. For example, for selection bias, the question whether baseline differences with respect to salivary flow rates or symptoms of xerostomia between intervention groups suggest a problem with the randomization process is not considered at all but is of high relevance [data missing in Braga et al. (2011) (14), Cho et al. (2008) (25), Meng et al. (2012) (26), and Simcock et al. (2013) (27); Dymackova et al. (2020) (10), Cho et al. (2008) (25) and Meng (2012) (28) with highly important differences between both groups].
Overview of features that have been subsumed in the respective risk of bias (RoB) categories.
Performance bias. For performance bias, some authors only referred to blinding of the participants. Only one study assessed blinding of the participants (28). The authors asked the patients “whether they thought they were in the real or sham acupuncture group, or if they could not tell”. They concluded that the “sham group remained blinded, with all patients in both groups believing they received real acupuncture”. Yet, in case the patients had understood the design of a sham controlled randomized study, an even distribution of believing in being in the verum and the sham group should be recorded.
Moreover, as in all studies the acupuncturist was a well-trained person with long-standing expertise, mostly certified in Traditional Chinese acupuncture, non-verbal interaction between the acupuncturist and the patients may have unblinded the patient to some extent in case of sham acupuncture if the acupuncturist appears less convinced of the effects of the actual treatment.
Detection bias. Also, for detection bias, the SRs focus on blinding of outcome assessment, which at least in the case the main authors and acupuncturists are the same person is not given. Important items as adherence [only reported in Garcia et al. (2019) (29)] are missing. Reasons for drop out are often not presented but may point to relevant problems with implementation and adherence.
Highly important are additional non-protocol interventions. In no study, there was a systematic recording. Yet, Pfister et al. (2010) describes that 40% on the control arm and 20% in the intervention arm used other complementary treatments. In two studies (30, 31) patients reportedly took drugs as pain medication, which may lead to xerostomia but data on whether there was a change in these medications during the course of the study are missing. Most important, radiotherapy may be highly different with respect to dosage, sparing of the glands, combination with different regimens of chemo- and immunotherapy. There is no study with a complete presentation and comparison of these data between the intervention and control arm.
More important, but completely neglected in the SRs, is the evocation of a De Qi sensation in the intervention arm. This feeling most probably is provoked by an irritation of a small nerve ending by the needling process. The needle is put on the skin or inserted and then manipulated until the patient gets a “De Qi feeling”. This allegedly proves the correctness of the individual needling point and the reaction of the body. During this part of the acupuncture treatment a strong interaction between the patient and the acupuncturist develops, which not only entails unblinding but also introduces an additional mental aspect into the treatment. Attrition bias. Considering attrition bias, incomplete outcome data were considered in all SRs. Yet, the authors do not discuss imbalances due to attrition. In Meng et al. (2012) drop out was higher in patients with stage IV disease and women, which might have led to imbalance between both groups, but data is missing (26). In Alimi et al. (2012), from the methods section one learns that the study was interrupted if for example there was a progress of the symptoms leading to a change in the pharmacotherapy. Yet, no data are provided how many participants stopped. But by this, patients with a deterioration could have been removed from the analysis (31). Also, in Meng (2012), in the study protocol, it was written that patients who took medication against dry mouth would be removed from study, which might exclude especially those with worse course. Also, data are missing in the results section (26, 28).
Reporting bias. For reporting bias, the authors of the SRs only considered selective reporting and did not discuss whether assessors were aware of the assignment of the patients. In fact, in no study there is a report that assessors were blinded and/or independent.
Considering the results of a study, clinical significance apart from statistical significance are important. None of the SRs discusses clinical relevance of statistically significant results in detail. Garcia et al. (2013) only state that “eight (studies) reported clinically significant positive within-group findings” without referring to the quality of the studies (21). Mercadante et al. (2017) write for the single study with a statistical positive result (27) clinical significance was unclear (20). Ni et al. (2020) refers to the clinical significance defined in the assessment via the Xerostomia Questionnaire but does not report whether the reduction of the incidence was clinically significant (13). The Cochrane Review by Furness et al. (2013) states that “The clinical importance of this finding is unclear (19). Moreover, none of the SRs deliberates on this issue in a critical summary of the results.
Another issue not discussed in the SRs is the composition of the patient group or the inclusion criteria. In Alimi et al. (2012) also patients with stomach cancer are included. Yet, these patients do not receive any radiotherapy leading to xerostomia. Moreover, more patients with stomach cancer are in the control group (31). In the group of studies conducted at the MD Anderson Cancer Center in USA and at the Fudan University in China, radiotherapy may differ between these countries, with intensity-modulated radiation therapy (IMRT), image-guided radiation therapy (IGRT) and gland sparing techniques more common in the USA. Garcia et al. (2019) reports that in spite of dose sparing on salivary glands, xerostomia was much higher in USA, which also points to the importance of objective measurements and consideration of cultural and social differences leading to different answers to the same instruments used for patient reported outcomes (29).
Discussion
At the first glance the relationship between acupuncture and xerostomia is well studied considering the large number of SRs on this subject. However, by comparing the eight SRs, this statement must be doubted. Altogether only 12 different mostly small studies were included in eight SRs. Thus, the number of SRs almost equals the number of individual RCTs. Even more important, two of these SRs, namely Zhuang et al. (2012) and Garcia et al. (2013) (21, 23) are from authors in the working group of Zhiqiang Meng (University Shanghai Cancer Center), who is also the first author of two single studies included in the SRs (26, 28). Moreover, the data reported by Blom et al. (1996 and 2000) (32, 33), Simcock (2013) (27) and Garcia (2019) (29) stem from one study, as Garcia states that Simcock et al. (2013) (27) and Blom et al. (2000) (33) are preliminary data and Blom et al. (2000) most probably provides the follow-up of the data from the study published in 1996. Moreover, Meng et al. (2012) (26, 28) reports that both trials were registered at ClinicalTrials.gov (NCT00862550 and NCT00430378) and both studies were approved by Institutional Review Boards at MD Anderson Cancer Center and Shanghai University Cancer Center. The MD Anderson Cancer Center is also the affiliation of Garcia who is the first author of one SR published in 2013 (21) and the RCT from 2019 (29), which reports data from USA and China.
In the study protocol to Garcia et al. (2019), published as supplement, the authors describe an RCT they conducted in China at Fudan Cancer Hospital with 85 patients with a positive result. The authors provide 3 references, but none reports these data (29).
Moreover, Garcia and colleagues in 2009 (34) reported the results of an one-armed study including 19 patients at the MD Anderson and report no significant differences for salivary flow rates. For quality of life, many pre-post comparisons were calculated, and some were significant. In the RCT reported in 2019 (29), the authors describe that true acupuncture was significantly better than sham only in China while in the USA, there was no significant difference between true acupuncture and standard care.
All in all, a majority of the studies and SRs was conducted by the same group of authors and does not provide independent evidence. Moreover, there are strong indications that data were not published completely.
Blinding is of high importance in complementary medicine, as the placebo effect may have a strong impact especially in endpoints which are subjectively assessed by the patient, therapist, or assessor. For the latter two, none of the studies provided blinding. In fact, as in all studies, the therapists were highly experienced acupuncturists with certificates and several years of practice, they most probably are convinced of the usefulness of acupuncture. Moreover, in some studies, the main authors were the therapists. Blinding in complementary medicine often is not possible as the patients are actively involved in the treatments. Also, for needling, in spite of concepts of sham acupuncture, it is doubtful whether blinding is successful. In the studies included in this review, non-penetrating needles were used in some studies, and it remains unclear whether patients do not notice the difference. Elaborate designs as in Garcia et al. (2019) (29) try to improve blinding. Yet, also in this study, the De Qi sensation was evoked in the true acupuncture arm.
Considering blinding of the patients, only one study assessed this item (Meng 2012) (28). This study from China states that blinding was perfect as all patients thought they were in the real acupuncture group. Yet this clearly shows that the patients had not understood the randomized trial design. In fact, it is well known, that the randomization process in studies conducted in China is not well established as a part of good scientific practice. As early as in 2007, the authors of a Cochrane review wrote that they contacted the study authors and “discovered that they misunderstood the randomization procedure and the trials were identified as non-RCTs” (35). Moreover, developing Traditional Chinese Medicine in Europe is a goal of high priority for Chinese authorities (36) and fraud within Chinese scientific articles is an issue of raising concern in the scientific community (37). This is even more important, as the number of SRs and MAs from China is raising rapidly for all topics of complementary medicine. Moreover, most of these articles include a growing number of studies published in Chinese journals in Chinese language and only listed in Chinese databases. Accordingly, no control is possible by the reviewer or the reader. This in fact means, that the quality and correctness of this nominally level IA evidence is mostly or only judged from formal characteristics. Yet, if studies of low evidence or even false data are included, this will hardly be discovered. The RoB instruments guide reviewers and review authors through a formal process but as we have shown in this small set of studies, further scrutinizing the publications is needed to detect issues of concern. Moreover, the RoB Tool offers the possibility to state a low risk of bias if the evaluator concludes that missing blinding does not influence the outcome. All in all, concluding the risk of bias is just a suggestion in the tool and may be passed over by the evaluator. Only two SRs evaluated the blinding-domain with a high risk of bias for performance/detection bias (11, 21), while two SRs (13, 23) give low risk evaluations for their placebo-controlled trials. Unfortunately, the authors do not have to provide the specific reasons for these decisions.
Limitations of this work. We only evaluated SRs that included mainly RCTs. Therefore, other publications were not considered, even though their methods might be of good quality. Moreover, we did not assess the single studies but based our final results on the reporting in the SRs. Yet, as all SRs and MAs come to quite similar conclusions, the probability of overlooking a study, false reporting or interpreting is rather low.
Conclusion
To summarize, the evidence on the use of acupuncture as treatment for radiotherapy induced xerostomia is low. There is no evidence for endpoints with objective assessment. For subjective assessment, there are some data which may completely be explained by the placebo effect. Some experts therefore discuss whether acupuncture does not need traditional acupoints but is more or less a question of the setting, the interaction between therapist and patient, the shared believe in De Qi and some self-effectiveness from the side of the patient. Whether needling is needed at all remains unclear and acupressure is established especially in the field of nursing. Acupressure has the advantage of the patient being independent from an acupuncturist. Moreover, it is cheaper, available nearly at any time and place. Yet, the question is whether it is a good idea to teach lay people acupoints belonging to a tradition, which no longer is supported by scientific evidence? Enabling patients to take over responsibility also entails increasing health literacy, medical knowledge, and a notion of evidence-based medicine to really empower patients.
Footnotes
↵Authors’ Contributions
J. Hübner: Supervision of systematic research and selection of studies, reviewing and editing, writing - original draft preparation; J. Dörfler, M. Freuding: Selection of studies, data extraction and evaluation, writing – original draft preparation; C. Zaiser: Data extraction and evaluation; J. Büntzel, C. Keinki, L. Käsmann: Writing – reviewing and editing.
Conflicts of Interest
The Authors declare no conflicts of interest. There was no funding to this work.
- Received July 21, 2022.
- Revision received August 22, 2022.
- Accepted August 31, 2022.
- Copyright © 2022, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.