


Abstract
Background/Aim: In the Japanese Classification of Gastric Carcinoma, T4a gastric cancer is defined as tumor invasion contiguous to the serosa or penetrating the serosa with exposure to the peritoneal cavity. The aim of this study was to assess the impact of T4a subclassification of gastric cancer on survival. Patients and Methods: A total of 326 patients with T4a cancer who had undergone gastrectomy were enrolled. The T4a tumors were classified into two groups: serosa-contiguous or serosa-exposed. Results: The serosa-exposed group had a significantly worse prognosis, and multivariate analysis identified the T4a subclass as an independent prognostic factor. Analysis of the risk factors for recurrence identified the T4a subclass as a significant risk factor for peritoneal recurrence in patients undergoing curative gastrectomy. Conclusion: The serosa-contiguous and serosa-exposed subgroups of T4a gastric cancer showed different biological behaviors. These groups may need to be treated as separate.
Although the prognosis of patients with gastric cancer, which is the fifth most commonly diagnosed malignant tumor in the world, continues to improve, gastric cancer remains the third leading cause of cancer-related death worldwide (1). It is widely accepted that the most important prognostic indicators in patients with gastric cancer are the depth of invasion of the gastric wall and the status of lymph node metastasis (2-4). Therefore, accurate/optimal categorization of the invasion depth and lymph node metastasis is critical for determining the disease extent, treatment planning, and prediction of the outcome (5). In Japan, treatment for gastric cancer is guided by the Japanese Classification of Gastric Carcinoma (JCGC) (6).
In the JCGC, the depth of invasion (T1) is divided into T1a (mucosa, M) and T1b (submucosa, SM). T2 and T3 are defined as invasion up to the muscularis propria (MP) and subserosa (SS), respectively. T4 is divided into T4a (invasion of the serosa, SE) and T4b (invasion of adjacent structures, SI). T4a is defined as tumor invasion contiguous to the serosa or penetrating the serosa with exposure to the peritoneal cavity (6). However, few studies have compared the clinicopathological characteristics of tumors contiguous to the serosa and tumors exposed beyond the serosa in patients with T4a gastric cancer (7). Many studies examining the status of serosal invasion of the tumor have focused on the changes in the macroscopic appearance of the serosa caused by tumor invasion, that is, changes in the color/morphology of the serosal surface (8-11) and/or the width of serosal invasion (12, 13). The objectives of this study were to investigate the clinical significance of subclassification of T4a gastric cancer into two groups: the tumor-contiguous group, with tumor invasion contiguous to the serosa, and the tumor-exposed group, with the tumor invading beyond the serosa and exposed to the peritoneal cavity and to assess the impact of this subclassification on the survival of patients with T4a gastric cancer.
Patients and Methods
Patients. Between January 2006 and June 2020, 1,468 patients with gastric cancer underwent gastrectomy at the Department of Gastroenterological Surgery of Tokai University School of Medicine. Of these, 326 were classified as having T4a cancer based on the tumor invasion depth. In the present retrospective study, we analyzed the data of these 326 patients. The gross classification and histopathological classification were based on the JCGC published by the Japanese Gastric Cancer Association (6). Staging was performed according to the American Joint Committee on Cancer (AJCC) staging manual, eighth edition (14). Patients were mainly followed-up on an outpatient basis at our hospital; however, those who had moved to other institutions were asked relevant questions over the phone. Follow-up was continued until June 2021, with a median duration of follow-up of 1,167 days (range=64-4,901 days). Tumor recurrence was confirmed by relevant investigations in patients in whom it was suspected on clinical grounds. In some patients, the initial recurrence was diagnosed at two or more sites, and in such patients, all of the sites were counted as sites of initial recurrence.
This research was conducted in accordance with the ethical standards of the institutional research committee and the 1964 Declaration of Helsinki and its later amendments. The study design and the informed consent provided by all study subjects were both approved by the institutional review board of Tokai University Hospital (registration number 21R-122).
Definition of the T4a subclasses. The resected stomach was opened and placed on a flat board with the mucosal side up, and fixed in 10% formalin. After fixation, the neoplasm was sectioned along the maximum cross-sectional plane parallel to the lesser curvature, based on the general rules of the JCGC (6). Several additional sections parallel to the maximum cross-sectional plane and one section perpendicular to this plane were prepared to identify the area with the deepest invasion. T4a gastric cancers were subclassified into a group in which the tumor invasion was contiguous to the serosa (serosa-contiguous group) and a group in which the tumor invasion penetrated the serosa and was exposed to the peritoneal cavity (serosa-exposed group), according to the JCGC (6) (Figure 1). One patient in whom the tumor invasion was contiguous to the serosa in one area, but was exposed beyond the serosa in another area was classified into the serosa-exposed group.

Pathological features of T4a gastric cancer (hematoxylin-eosin staining, ×100). A) Tumor invasion was contiguous to the serosa (arrow). B) Tumor invasion penetrated the serosa with exposure to the peritoneal cavity (arrow).
Statistical analysis. The chi-squared test was used to compare categorical data, and the Mann-Whitney U-test to compare continuous variables. Overall survival (OS) was defined as the time period from operation to death from any cause. Survival curves were estimated using the Kaplan-Meier method, and survival times were compared using the log-rank test. Multivariate logistic regression analysis was applied to identify the clinicopathologic factors significantly correlated with recurrence, and a Cox proportional hazards model was used to identify factors significantly correlated with the prognosis. Factors that were identified as being significant on univariate analysis and essential and additional prognostic factors for survival as specified by the AJCC staging manual, eighth edition, were selected as the covariates (14). p<0.05 was considered as being indicative of statistical significance. All the statistical analyses were performed using SPSS, version 26.0J (IBM Corp., Armonk, NY, USA).
Results
Clinicopathologic characteristics according to the T4a subclass. Of the 326 patients with T4a gastric cancer, 93 were classified into the serosa-contiguous group and 233 into the serosa-exposed group. We compared the clinicopathological factors between the two groups (Table I). As compared with the serosa-contiguous group, the serosa-exposed group showed significantly higher frequency of the macroscopic infiltrative type of tumor (p=0.001), a larger tumor diameter (p=0.001), a higher frequency of patients with more advanced disease stage (p=0.001), and a higher frequency of patients with residual tumor (p=0.001).
Association between clinicopathological parameters and T4a subclass.
Correlation of the T4a subclass with prognosis. The 5-year OS rates in the serosa-contiguous and serosa-exposed groups were 51.1% and 23.8%, respectively, indicating a significantly worse prognosis in the serosa-exposed group as compared with that in the serosa-contiguous group (p=0.001) (Figure 2). The prognostic impact of the T4a subclass was evaluated by univariate and multivariate analyses (Table II). Univariate analysis identified the gross tumor type, tumor size, lymphatic invasion, lymph node metastasis, distant metastasis, residual tumor, and T4a subclass as significant prognostic factors. Multivariate analysis identified distant metastasis and the T4a subclass as independent prognostic factors.

Kaplan-Meier curves and log-rank test for overall survival (OS) of all patients according to the T4a subclass. The prognosis was significantly worse in the serosa-exposed group than that in the serosa-contiguous group (p=0.001).
Univariate and multivariate analyses of prognostic factors for overall survival of all patients.
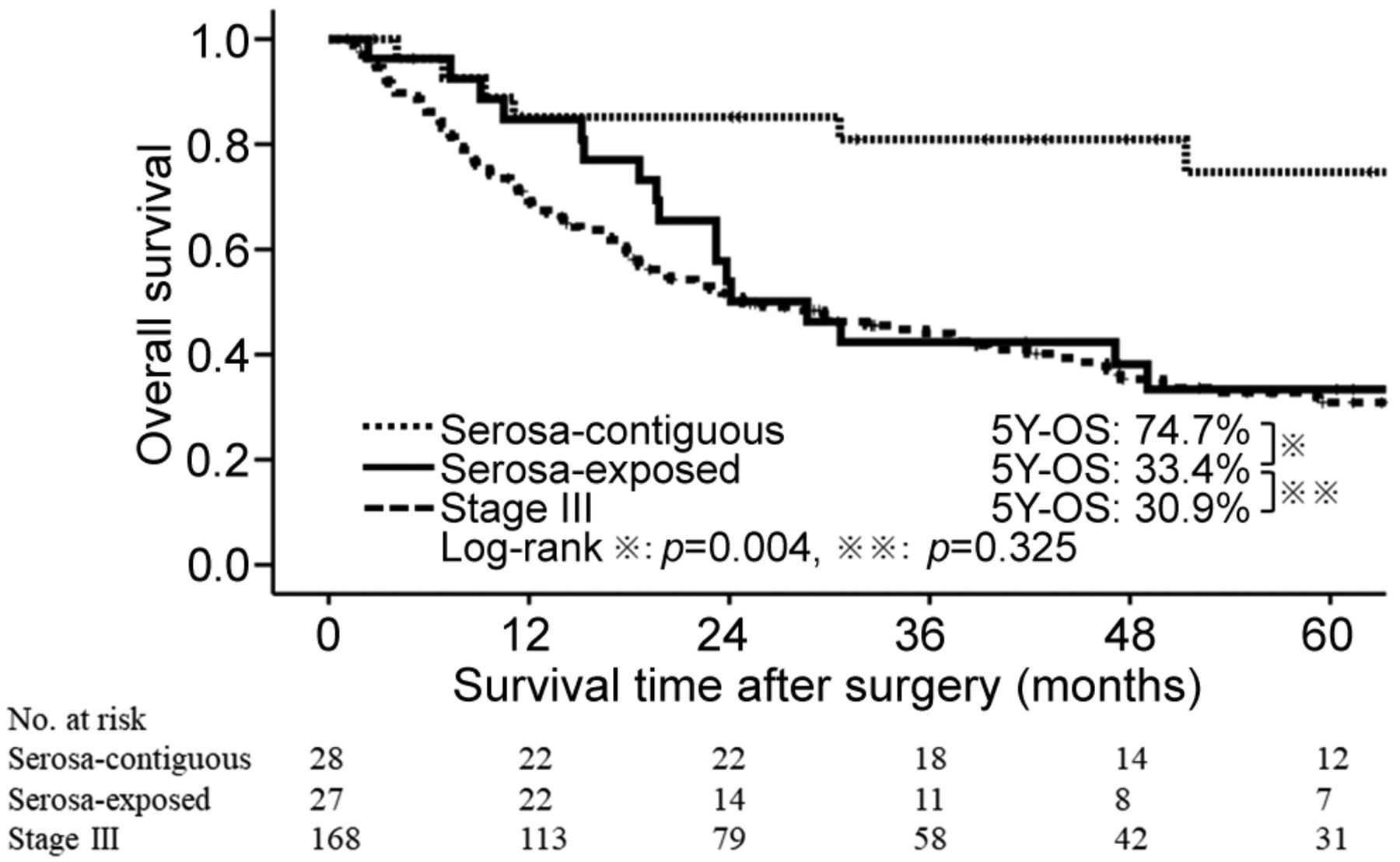
Relationship between the T4a subclass and the prognosis by disease stage. The prognostic impact of the T4a subclass for each disease stage was evaluated. There were 55 stage II patients, including 28 in the serosa-contiguous group and 27 in the serosa-exposed group. Univariate and multivariate analyses identified the T4a subclass as the only independent prognostic factor (Table III). Next, the prognosis of the stage II patients, including the serosa-contiguous and serosa-exposed groups, was compared with that of the 168 stage III patients. The 5-year survival was 74.7% in the stage II serosa-contiguous group, 33.4% in the stage II serosa-exposed group, and 30.9% in the stage III patients. Thus, in stage II patients, the prognosis was significantly worse in the serosa-exposed group than in the serosa-contiguous group (p=0.004), and the serosa-exposed group and stage III patients showed overlapping survival curves and no significant difference in the prognosis (p=0.325) (Figure 3). Of the 168 stage III patients, 52 were classified into the serosa-contiguous group and 116 into the serosa-exposed group. Univariate and multivariate analyses were performed to identify the prognostic factors. Univariate analysis identified the gross tumor type, lymph node metastasis, and T4a subclass as significant factors influencing prognosis. Multivariate analysis identified the resection type and lymph node metastasis as independent prognostic factors (Table IV). Only 12 stage IV patients underwent curative resection; therefore, they were not evaluated for prognostic factors.
Univariate and multivariate analyses of prognostic factors for overall survival of stage II patients.

Kaplan-Meier curves and log-rank test for overall survival (OS) in the stage II serosa-contiguous group, stage II serosa-exposed group, and stage III patients. The stage II serosa-exposed group had a significantly worse prognosis than the stage II serosa-contiguous group (p=0.004). The stage II serosa-exposed group and stage III patients showed no significant difference in prognosis (p=0.325).
Univariate and multivariate analyses of prognostic factors for overall survival of stage III patients.
Relationship between the T4a subclass and recurrence pattern. The relationship between the T4a subclass and the recurrence pattern was examined in the stage II and III patients. Of all the patients, 80 were classified into the serosa-contiguous group and 143 into the serosa-exposed group. The recurrence rate was 33.8% (27/80) in the serosa-contiguous group and 62.9% (90/143) in the serosa-exposed group, indicating a significantly higher incidence of recurrence in the serosa-exposed group (p=0.001). Analysis according to the recurrence pattern revealed that the incidence of peritoneal recurrence was 21.3% (17/80) in the serosa-contiguous group and 36.4% (52/143) in the serosa-exposed group; the incidences of lymph node recurrence were 13.8% (11/80) and 20.3% (29/143), and those of hematogenous recurrence were 15.0% (12/80) and 18.9% (27/143) in the two groups, respectively. Thus, the peritoneal recurrence rate was significantly higher in the serosa-exposed group (p=0.019). The impact of the T4a subclass on the likelihood of peritoneal recurrence was evaluated by univariate and multivariate analyses. The T4a subclass and histologic type were identified as independent risk factors for peritoneal recurrence (Table V).
Univariate and multivariate analyses of risk factors for peritoneal recurrence of stage II-III patients.
Discussion
Even with the development of standardized D2 lymphadenectomy (15) and postoperative adjuvant chemotherapy (16, 17) for advanced gastric cancer, the survival outcomes still remain unsatisfactory, with gastric cancer accounting for a third of all cancer-related deaths worldwide (1). Patients, especially those with T4 disease, often suffer from recurrence within the first 5 years after curative resection. A better understanding of the prognostic factors and recurrence patterns in patients with T4 gastric cancer will help clinicians adopt more intensive treatment strategies for high-risk patients. In the JCGC, T4 gastric cancer is divided into T4a and T4b; T4a gastric cancer is defined as tumor invasion contiguous to the serosa or penetrating the serosa with exposure to the peritoneal cavity (6). That is, the biological behaviors of the tumors are considered to be comparable between the serosa-contiguous group and serosa-exposed groups of patients with T4a gastric cancer. However, few studies have investigated the differences in the clinicopathological characteristics between these groups (7), and the findings of present study are expected to be useful for elucidating the pathogenesis of T4 gastric cancer.
The analyses in this study revealed that in patients with T4a gastric cancer, the serosa-exposed group had a higher frequency of patients with more advanced stage and residual tumor, and worse 5-year survival rates as compared with the serosa-contiguous group. Multivariate analysis identified the serosa-exposed T4a subclass as an independent poor prognostic factor, suggesting different biological behaviors of the tumors between the serosa-contiguous and serosa-exposed groups. The serosa is a visceral peritoneal layer covering the surface of the stomach that is lined by mesothelial cells, a basement membrane, and a submesothelial layer and only allows passage of water, electrolytes, urea, and small molecules. Therefore, in theory, an intact serosa can limit the progression of cancer and prevent cancer cells from entering and becoming implanted into the peritoneal cavity (7). It is the disruption of this serosal barrier that is considered to result in the worse prognosis in the serosa-exposed group as compared with that in the serosa-contiguous group.
In the analysis by disease stage, multivariate analysis identified the T4a subclass as an independent prognostic factor in patients with stage II disease: the serosa-exposed group had a significantly worse prognosis than the serosa-contiguous group. In addition, the prognosis of the serosa-exposed stage II patients was equivalent to that of the stage III patients, suggesting that it might be better to treat this group of patients as cases of stage III disease. According to the guideline, tegafur-gimeracil-oteracil (S-1) monotherapy is recommended as postoperative adjuvant chemotherapy for stage II gastric cancer patients, while oxaliplatin-based combination therapy is recommended as postoperative adjuvant therapy for stage III gastric cancer patients in Japan (18). The results of the present study suggest that the serosa-exposed stage II patients should receive oxaliplatin-based combination therapy as postoperative adjuvant chemotherapy, like patients with stage III disease, rather than S-1 monotherapy. In stage III patients, univariate analysis identified the T4a subclass as a significant prognostic factor, while multivariate analysis did not identify the T4a subclass as an independent prognostic factor. To date, few studies on the degree of serosal invasion in T4a gastric cancer have investigated whether the degree of serosal invasion is a prognostic factor or not in each disease stage, as in the present study (19). In Japan, postoperative adjuvant chemotherapy regimens vary among the disease stages. Therefore, the proposal of the present study, that stage II patients with a relatively poor prognosis should be extracted and administered postoperative adjuvant chemotherapy regimens as for stage III disease, appears to be suitable for clinical practice and immediately implementable.
In the assessment of the risk factors for recurrence, multivariate analysis identified the T4a subclass as an independent risk factor for peritoneal recurrence. Many studies on the relationship between the degree of tumor serosal invasion and recurrence have stated that macroscopic serosal change is a risk factor for peritoneal recurrence (8, 12, 20). However, reported macroscopic serosal findings may vary among surgeons. Furthermore, although studies have examined macroscopic serosal changes since the 1990s (21), no diagnostic criteria have been established. Therefore, the diagnostic accuracy of macroscopic serosal changes has been reported to be 74% by Yura et al. (19), 82% by Kang et al. (22), and 88% by Jeong et al. (23), with differences among institutions. The evaluation criteria used in the present study were defined by the JCGC and do not appear to vary among institutions. The Japanese Gastric Cancer Treatment Guidelines propose performing computed tomography or ultrasonography every 6 months for 3 years after surgery in patients with stage II/III gastric cancer (18). The present study suggests that it is necessary to use imaging modalities, including positron emission tomography and magnetic resonance imaging, at even shorter intervals in the serosa-exposed group, because this group appears to have a significantly higher incidence of peritoneal recurrence. In stage III patients, the T4a subclass was not a significant prognostic factor, but was found to be a significant risk factor for peritoneal recurrence. Therefore, it is considered necessary to subclassify T4a gastric cancer for postoperative follow-up, even in stage III patients.
This study had some limitations. First, it was a retrospective single-center study with a small sample size. Second, whole sections of primary tumors were not used; therefore, the serosa-contiguous group may have included some patients who should actually have been included in the serosa-exposed group. The JCGC prescribes that when the resected stomach is sectioned in cases of early gastric cancer, whole sections of the tumor should be cut at 5-mm intervals. It also prescribes that when the resected stomach is sectioned in cases of advanced gastric cancer, the area of deepest invasion of the tumor should be sectioned parallel to the lesser curvature; it does not prescribe for whole sections of the lesion to be cut (6). In the present study, the recommendations of the JCGC were followed for the preparation of tissue sections. In the future, it may be necessary to investigate how sections should be cut in order to determine the area of the lesion showing the greatest depth of invasion without having to prepare whole sections.
In conclusion, T4a gastric cancer is defined as a tumor contiguous to or exposed beyond the serosa, and these tumors are treated as equivalent entities by the JCGC guideline. Our findings revealed that in patients with T4a gastric cancer, the serosa-exposed group had a significantly worse prognosis than the serosa-contiguous group; that is, the T4a subclass was an independent prognostic factor. The analysis by stage also showed that the T4a subclass was an independent prognostic factor as well as a risk factor for peritoneal recurrence. Therefore, we concluded that the biological behaviors of the tumors differ between the serosa-contiguous group and serosa-exposed group of patients with T4a gastric cancer, and that, therefore, these two groups may need to be treated as being separate, unlike the recommendation in the JCGC guideline.
Footnotes
Authors’ Contributions
Conception and study design were conducted by NK, NE, and KK. Data collection and literature search were done by NK, TK, OM, and HH. Data analysis and interpretation were performed by NK and NK. The article was drafted by NK and KK. Finally, the article was revised and approved by all investigators.
Conflicts of Interest
The Authors declare that they have no conflicts of interest in regard to this study.
- Received March 9, 2022.
- Revision received April 20, 2022.
- Accepted April 21, 2022.
- Copyright © 2022, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.