


Abstract
Background/Aim: Supra hemodiafiltration with reinfusion of the endogenous ultrafiltrate (Supra-HFR) is a dialysis technique used to improve uremic toxin removal in the range of the middle molecular weight molecules. Supra-HFR does not require the preparation and online infusion of high-purity dialysis water because it allows the production of an endogenous ultrafiltrate that undergoes detoxification through an adsorbing resin. Patients and Methods: We investigated the ability of Supra-HFR to remove fibroblast growth factor 23 (FGF23), interleukin 6 (IL-6), tumor necrosis factor alpha (TNF-alpha), interleukin 8 (IL-8), and transforming growth factor alpha (TGF-alpha) after a single session dialysis in nine patients affected by end stage renal disease (ESRD). The same patients underwent a single session of online hemodiafiltration (OL-HDF) to evaluate possible differences in FGF23 and IL-6 levels. Results: A significant reduction in FGF23 was observed with both Supra-HFR (p=0.001) and OL-HDF. As for TNF-alpha and TGF-alpha, which were measured using Supra-HFR only, their percentage values were significantly lower at the end of dialysis than at the start (p=0.0028 and p=0.03, respectively). This did not change with post-dialysis rebound. Supra-HFR was found to have no effect on IL-6 and IL-8. Interestingly, the removal rate for FGF23 and IL-6 was similar to that observed with OL-HDF. Conclusion: Supra-HFR was not superior to OL-HDF, with suboptimal convective volume in the removal of the molecules tested, especially FGF23, which is considered a large middle molecular weight uremic toxin.
Online hemodiafiltration (OL-HDF) combines diffusive and convective clearance of uremic toxins, thus allowing a markedly enhanced removal of middle molecular weight molecules. For this reason, it has been associated with better cardiovascular outcomes than standard hemodialysis (1-7). However, several pre-conditions need to be met to perform an effective OL-HDF, and not all hemodialysis patients are eligible for this treatment. Two main reasons prevent a broader application of OL-HDF: i) an inadequate vascular access (when blood flow is below 350 ml/min) (7); ii) a water treatment system unable to provide ultrapure water (8). Supra hemodiafiltration with reinfusion of the endogenous ultrafiltrate (Supra-HFR) seems to be a valid alternative, as it has been reported to effectively remove middle molecular weight uremic toxins without albumin loss and without the need of preparing and online infusion of high-purity dialysis fluid. However, despite encouraging data, additional studies are needed to confirm these findings (9-12).
The present study evaluated the efficacy of a single session of Supra-HFR in terms of removal of fibroblast growth factor 23 (FGF23) and inflammatory markers in the range of middle molecular weight molecules, namely interleukin 6 (IL-6), tumor necrosis factor alpha (TNF-alpha), interleukin 8 (IL-8), and transforming growth factor alpha (TGF-alpha). After the evaluation of Supra-HFR, a single session of OL-HDF was performed on the same patients, to check its efficiency in removing FGF-23 and IL-6.
Patients and Methods
Patients. The study included 9 hemodialysis patients from the Nephrology, Dialysis and Renal Transplant Unit of S. Orsola University Hospital of Bologna, Italy. The selection criteria were: age ≥18 years, urine output <200 ml/day, intermittent hemodialysis therapy for at least 6 months. Patients with systolic blood pressure before dialysis <90 mmHg, vascular access blood flow <250 ml/min, a current infection, or an active immunological disease were excluded, together with those who refused to participate in the study. Table I describes the main demographic and clinical characteristics of the patients.
Main demographic and clinical characteristics of the 9 enrolled patients. Data are given as median (minimum and maximum; interquartile range), or as absolute number (%).
A written informed consent was obtained from all the patients before inclusion. The study was carried out in accordance with the Declaration of Helsinki and approved by AVEC Ethics Committee for Bologna (code n°38/2017/U/sper) on March 14th, 2017.
Study design. This study investigated the ability of a single session of Supra-HFR to remove middle molecules, specifically FGF23, IL-6, TNF-alpha, IL-8, and TGF-alpha. The principal features of the selected molecules are shown in Table II.
Characteristics of the middle molecular weight molecules studied.
The patients, usually treated with high-flux bicarbonate dialysis, were shifted to a single 4-h-long mid-week Supra-HFR dialysis session. After two more weeks of high-flux bicarbonate dialysis, they underwent a single 4-h-long session of OL-HDF. This schedule was designed to assess possible differences in the FGF-23 and IL-6 removal capabilities of a single session of Supra-HFR vs. a single session of OL-HDF. Ultrafiltration was settled according to the usual prescription. The anticoagulation therapy consisted of low molecular weight heparin enoxaparin sodium (Clexane™, Sanofi-Aventis, Milan, Italy), administered in a single bolus at the start of dialysis in the arterial line of the extracorporeal circuit. The dose of enoxaparin was based on each patient’s weight: <50 kg=2,000 IU, 51-90 kg=4,000 IU, and >90 kg=6,000 IU. The dialysate flow was 500 ml/min. Ultrapure dialysis water was used according to the Italian guidelines on water and solution for dialysis (11). All the procedures were performed using Flexya dialysis machines (Bellco/Medtronic, Mirandola, Italy) for Supra-HFR and Fresenius 5008 (Fresenius Medical Care, Bad Homburg, Germany) for OL-HDF.
Blood samples were collected before the dialysis session (T0), at the end (T1) and 15 min after the end to evaluate toxin rebound (T2). Rebound was defined as the solute increase from T1 to T2. The values measured at T1 and T2 were corrected for hemoconcentration due to the patient’s weight loss, assuming monocompartimental behavior of solutes, according to the Bergström and Wehle formula (13):
Tx–corr = Tx/{1+(ΔBW/(0.2×BWpost))} [1]
where Tx is the blood solute concentration at T1 or T2, Tx-corr is the concentration of solutes at T1 or T2 corrected for the hemoconcentration, ΔBW (body weight) is the intradialytic weight loss, and BWpost is the body weight at the end of dialysis.
The stop dialysate flow method, that also involves the slow blood flow before blood drawing, was used to avoid blood recirculation into the vascular access (14). The reduction rate per session (RR) for the time point T1 was calculated as follows:
RR=(T0-T1-corr)/T0×100 [2]
Data measured at T1 and T2 were also given as percentage variation in comparison to T0 using the following formula:
Tx٭100)/T0 [3]
where Tx is the solute level at T1 or T2.
Supra-HFR. Supra-HFR (Bellco/Medtronic) uses a double chamber filter (Figure 1). The filter consists of a super high flux hemofilter (Synclear 02) with an ultrafiltration coefficient (Kuf) of 36 ml/h/mmHg, a surface area of 0.7 m2a membrane cut-off value of 45 kDa. The endogenous ultrafiltrate rate (Q plw) of 60 ml/min is obtained automatically, by means of the transmembrane pressure levels in the hemofilter. These are calculated from two pressure sensors: the first is placed on the arterial bubble chamber and the second before the roller pump of the ultrafiltrate. The ultrafiltrate is driven from this hemofilter to a 50 g neutral styrene resin with an adsorbing area of 35,000 m2. After adsorption, the ultrafiltrate is added to the whole blood that, in turn, passes through the second HFR filter, a polyphenylene low-flux filter (Kuf 13 ml/h/mmHg, surface area 1.7 m2) where the weight loss and the diffusive depuration take place.

Supra hemodiafiltration with reinfusion of the endogenous ultrafiltrate scheme. Δ body weight: the intradialytic weight loss; kDa: kilodaltons; Qb: blood flow rate; Qdin: dialysate inflow: SC: sieving coefficient; Qdout: dialysate outflow; Qplw: plasma water flow rate; QR: plasma water reinfusion rate; M.W.: molecular weight.
OL-HDF. OL-HDF was carried out with a standard high-flux filter (FX100 Cordiax, Helixone, Fresenius Medical Care, Bad Homburg, Germany, Kuf 73 ml/h/mmHg, surface area 2.2 m2 cut-off 30 kDa). The convective volume was suboptimal because it was maintained above 18 l/session, it was less than 23 l/session and it was not adjusted to the patients’ body surface area, as suggested by Peters et al. (2).
Laboratory assays. Blood samples were drawn into 9 ml lithiumheparin tubes (green-top). Plasma aliquots were immediately stored at –80°C and thawed at room temperature prior to the assays. Quantitative determination of FGF23, IL-6, TGF-alpha, IL-8 and TNF-alpha was performed in duplicate using Luminex®×MAP® system (Luminex, Austin, TX, USA). A multiplex panel was created by combining two commercially available simplex kits: Human Custom 19-Plex ProcartaPlex Panel (Cat. No. PPX-19-MXRWE2G; Invitrogen by Thermo Fisher Scientific, Waltham, MA, USA) and Human High Sensitivity T Cell (Cat. No. HSTCMAG-28SK; Merck Millipore, Darmstadt, Germany). Details including assay protocol, standards and sensitivity are available on the manufacturer’s website (15, 16). Concentrations were calculated using a standard curve obtained through serial dilutions and, finally, the plates were read on a Luminex MAGPIX system, and the data analysed with xPONENT® software (Luminex).
Statistical analysis. Continuous variables are reported as median (minimum and maximum, interquartile range) or as mean±standard deviation (SD), categorical variables are reported as absolute numbers with percentages.
The comparisons were made using parametric tests (multiple regression, ANOVA) for normally distributed variables and Mann-Whitney or Wilcoxon test, in case of paired data, for skewed distributions. Fisher’s exact test was used to evaluate the categorical variables. A p-value <0.05 was considered significant. Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS™ for Windows Software Package, version 9.0.1; Chicago IL, USA). Images were generated using GraphPad Prism™ (version 8 for Apple, GraphPad Software Inc., CA, USA).
Results
All treatments with Supra-HFR were well-tolerated. The efficacy in the solute removal of FGF23, IL-6, TNF-alpha, IL-8, and TGF-alpha was analyzed in the nine ESRD patients after a single dialysis session. The median blood flow rate was 290 ml/min (range=250-300 ml/min) and the median endogenous reinfusion rate was 13 l/session (range=10-15 l/session). The same patients underwent, two weeks later, a single session of OL-HDF to evaluate potential differences in post-dialysis FGF23 and IL-6 levels. For OL-HDF, the median blood flow was 300 ml/min (range=250-300 ml/min) and the median convective volume was 20 l/session (range=18-22 l/session).
Table III presents the circulating levels at T0 of FGF23, IL-6, TNF-alpha, IL-8, and TGF-alpha before the Supra-HFR session and those of FGF23 and IL-6 before OL-HDF; it also includes the RR% per session, calculated according to formula [2] mentioned above. The RR of FGF23 and IL-6 achieved with Supra-HFR and OL-HDF did not differ significantly.
Solute values at T0 and RR% per session, calculated as (T0-T1-corr)/T0×100. Data are given as median (minimum and maximum; interquartile range). Comparisons of RR between Supra-HFR and OL-HDF were analysed by Mann-Whitney nonparametric test.
Table IV presents solute values at T1 and T2, with percent rebound calculated according to formula [1]. Again, no significant differences were found between the two techniques in terms of FGF23 and IL-6 post-dialysis rebound.
Univariable and multivariable logistic regression analysis of the primary outcome measure intraventricular hemorrhage. The outcome parameters of the total collective of neonates delivered at 28-34 weeks of gestational age are shown.
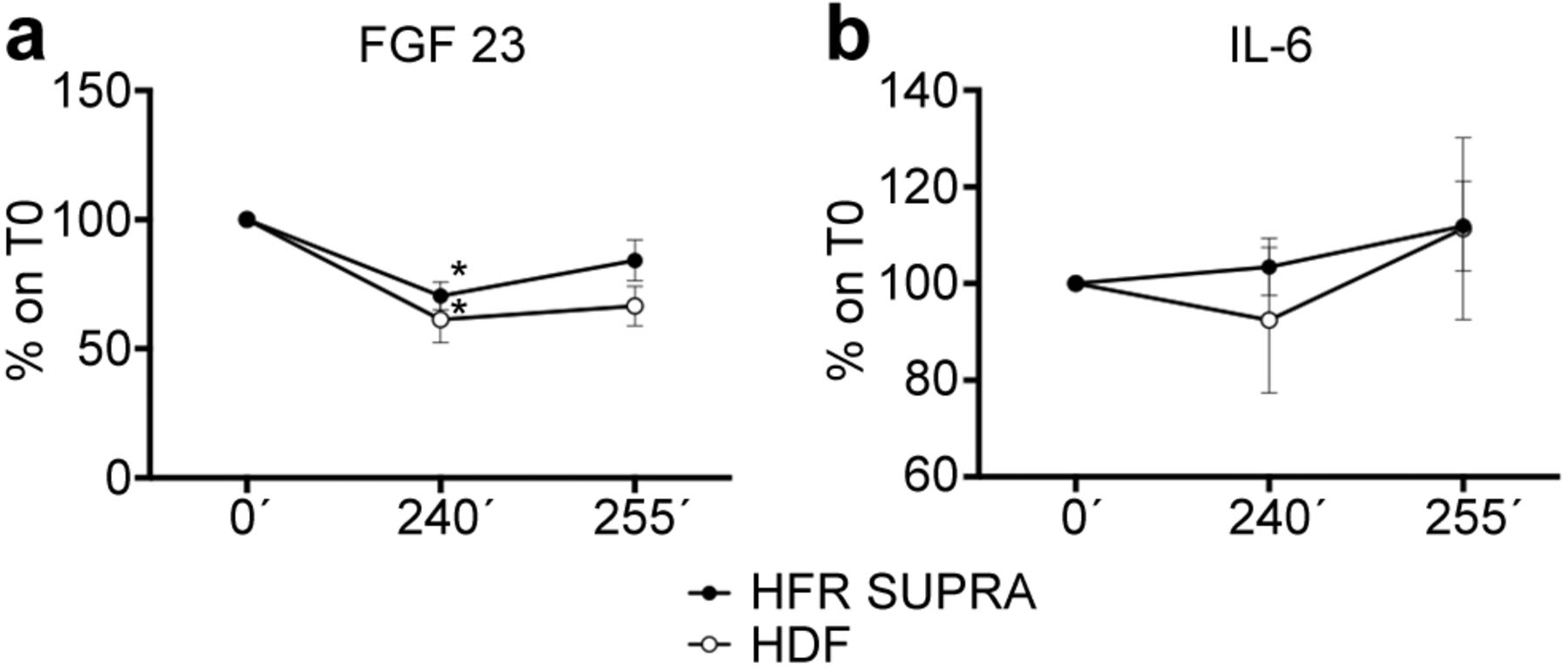
Figure 2 illustrates the trends in FGF23 and IL-6 with both Supra-HFR and OL-HDF at T0 (before starting the dialysis session), T1 (at the end of the dialysis session), and T2 (15 min after the end of the session, to evaluate toxin rebound). A significant reduction in FGF23 was observed between T0 and T1 with both Supra-HFR (p=0.001) and OL-HDF (p=0.04), while no differences were found for IL-6. At T2, only IL-6 showed a slight, although not significant, postsession rebound, regardless of the technique.

FGF23 (A) and IL-6 (B) trends at the three experimental time points in Supra-HFR and OL-HDF. Values are expressed as median with interquartile range of 9 treatments for both techniques. Significance is reported for T1 vs. TO: p=0.001 for Supra-HFR and p=0.04 for OL-HDF. No significant differences are reported between the two techniques. All the comparisons were analyzed by Mann-Whitney nonparametric test. HFR: Hemodiafiltration with reinfusion of the endogenous ultrafiltrate; OL-HDF: online hemodiafiltration.
Figure 3 describes the changes in TNF-alpha, IL-8, and TGF-alpha over time in relation to the Supra-HFR treatment. Percent delta variations at T1 and T2 normalized to T0 were calculated according to formula [3] mentioned above. The removal efficiency at T1 was significant for TNF-alpha (p=0.0028) and TGF-alpha (p=0.03), while the decline of IL-8 levels did not reach statistical significance. Comparing T2 and T0, the effectiveness of Supra-HFR in clearing solute was confirmed only for TNF-alpha (p=0.03) and TGF-alpha (p=0.02).

TNF-alpha (A), IL-8 (B) and TGF-alpha (C) trends at the three experimental time points. Values are expressed as median with interquartile range and represent 9 treatments with Supra-HFR. HFR: Hemodiafiltration with reinfusion of the endogenous ultrafiltrate.
Finally, albumin levels remained stable between T0 and T1 both with Supra-HFR (3.3±0.37 gr/dl vs. 3.2±0.35 gr/dl, p=n.s.) and with OL-HDF (3.4±0.33 gr/dl vs. 3.2±0.32 gr/dl, p=n.s.). No differences in albumin levels were found at any point in time, when comparing the two techniques.
Discussion
The removal of uremic toxins in the range of the middle molecular weight molecules during hemodialysis is pursued as a challenge to prevent cardiovascular risk and chronic inflammation, commonly found in ESRD patients.
Supra-HFR was effective in achieving a significant reduction of some, but not all, the markers we examined, namely FGF23, TNF-alpha and TGF-alpha. The Supra-HFR cartridge is able to deliver a sorbent-based detoxification therapy. The neutral styrene resin in this cartridge consists of granules with a single particle diameter of about 100 μm and inner pores measuring between 20 and 50 Å (macroporous). Such resin has a high affinity for several uremic toxins in the range of the middle molecular weight molecules, including beta 2-microglobulin, homocysteine, parathyroid hormone, and many cytokines (17-19). The chemical nature of the neutral styrene resin of the Supra-HFR cartridge can thus explain our results, in particular the significant reduction in FGF23, TNF-alpha and TGF-alpha which is in line with what has been previously described for other middle molecular weight molecules (11).
The increase of serum FGF23 seen in the uremic status has been associated with a higher risk of cardiovascular mortality, due to its direct and causal role in secondary cardiac hypertrophy, arterial stiffness, vascular calcification, and inflammation (20, 21). We found only two other studies emphasizing the effectiveness of different dialysis techniques, OL-HDF and hemodialysis with medium cut-off dialyzers (MCO-HD), in removing FGF23. Potier et al. demonstrated the superiority of post-dilution OL-HDF over high-flux hemodialysis, mixed OL-HDF and pre-dilution OL-HDF in achieving effective solute clearance. In particular, the removal of FGF23 approached 55% of the initial value in 6 hemodialysis patients during a single OL-HDF session. With a mean blood flow of 350 ml/min, the convective volume was 30 L per session (1). Belmouaz et al. recently compared the effectiveness of MCO-HD and high-flux dialysis (HF-HD) in removing the middle molecular weight molecules in 40 patients during a 3-month observation period. The authors found a significantly higher RR for FGF23 with MCO-HD than with HF-HD (41±22% vs. 20±21%,p<0.0001) (22).
To the best of our knowledge, this study is the first to describe successful FGF23 removal using Supra-HFR, with an intradialytic RR of 40.6% (median value). FGF23 showed a tendency to increase again 15 min after the end of the dialysis session, although this trend did not reach statistical significance between T1 and T2 for both techniques. However, it led to a non-significant reduction of FGF23 between TO and T2 (Figure 2). The explanation for this slight rebound might lie in different factors: i) a failure of the single-compartmental model to estimate FGF23 clearance (3); ii) an intradialytic generation rate and intercompartmental transport of FGF23 that is greater than dialytic clearance; iii) a suboptimal production and detoxification of the endogenous ultrafiltrate; iv) the erythropoietin i.v. injection at the end of dialysis that can increase the FGF23 mRNA expression in the bone marrow (23).
IL-6 is a well-known proinflammatory cytokine, mainly secreted by macrophages, referred to as a key driver in the inflammatory response of the liver. Bologa et al. indicated IL-6 as an independent predictor of mortality in hemodialysis patients (24). Several other authors tried to achieve a significant reduction in IL-6 during dialysis, focusing on the dialysis technique itself and, in particular, on the removal efficiency of HFR. In a randomized crossover study by Panichi et al., a previous version of HFR with a charcoal-based resin was able to significantly reduce IL-6 in comparison to low-flux hemodialysis, while no difference was found between HFR and OL-HDF in terms of IL-6 removal (25). A more recent study by Tessitore et al., comparing Supra-HFR to low-flux hemodialysis in 28 chronic hemodialysis patients, failed to highlight significant reductions in IL-6 levels with both dialysis techniques (26). Few other authors considered the efficiency of Supra-HFR in cytokine removal during a single HFR session. Our findings are consistent with a previous report by Riccio et al., where no difference was observed between IL-6 levels measured before and after a single Supra-HFR session. Nonetheless, a significant IL-6 reduction was found during Supra-HFR, after the resin cartridge, at 15 min and after 225 min from the dialysis start, mirrored by a parallel decrease of IL-6 mRNA expression and protein release (27). Recently, Chen et al. confirmed that IL-6 remained unchanged in 37 hemodialysis patients after one session of Supra-HFR. The experimental times considered were 15 min before and after dialysis (28). All these data are in line with our findings, since we were not able to detect significant changes in IL-6 values using Supra-HFR. The results obtained here with Supra-HFR did not differ from those with OL-HDF. However, the convective dose achieved with OL-HDF did not reach the threshold of 23 L adjusted for the body surface area, suggested by Peters et al. (2). The main reason for this drawback was the vascular access: it did not allow a blood flow >300 ml/min. It is also of note that in the study by Panichi et al. the mean convective volume during OL-HDF was 18 l/session (25).
TNF-alpha is a relevant inflammation marker in the uremic population, and its increased levels have been associated with malnutrition, inflammation and higher cardiovascular and all-cause mortality (29). The two studies by the Tessitore and Chen mentioned above reported a significant reduction of TNF-alpha associated with the use of Supra-HFR, but lacked an assessment of TNF-alpha postdialysis rebound (26, 28). In our patients, the rate of TNF-alpha rebound after dialysis did not influence the RR of TNF-alpha levels obtained with Supra-HFR.
This is the first study to assess the role of Supra-HFR in removing the chemokine IL-8, which is a uremic toxin correlated with increased all-cause and cardiovascular death (29). Unfortunately, our results did not confirm our expectations about the efficacy of Supra-HFR in removing IL-8, which was based on its molecular weight. This unsatisfactory result might be due to IL-8 generation rate being higher than its removal rate.
TGF-alpha is not currently considered a uremic toxin, but some evidence exists on its pathophysiological role in parathyroid hyperplasia during ESRD (30). TGF-alpha molecular weight falls within the range of middle molecules, and Supra-HFR was indeed effective in its removal, with no rebound after dialysis.
Although OL-HDF with a convective flux >23 l per session adjusted for the body surface area, which is related to a better survival of the patients in comparison to bicarbonate dialysis (2), can be achieved when the vascular access allows a blood flow >350 ml/min, the use of a lower total convective volume, as in our case, is not uncommon. The DOPPS study assessed that a fluid replacement volume >20 l/session was achieved in only 50% of 2,012 patients on HDF (31). This is true in particular for patients with greater comorbidities, who are less likely to achieve high convective volume exchanges (2, 32). Since the high clearance of middle molecular weight molecules provided by OL-HDF with optimal convective replacement volume may likely improve the clinical outcome, the hypothesis tested in the present study was that Supra-HFR may provide a more adequate removal of the middle molecular weight molecules than OL-HDF with a suboptimal convective flow (31).
A convective replacement fluid >23 l/session can be obtained by increasing the vascular access blood flow during OL-HDF but not for Supra-HFR, where the endogenous ultrafiltrate (or plasmatic water) produced by the first filter is then regenerated by adsorption. Decreased adsorption efficacy is often observed when the flow of endogenous ultrafiltrate is too fast (33). The relationship between the endogenous ultrafiltrate flow rate and the resin cartridge diameter (called linear velocity) translates in a balance between the volume of endogenous ultrafiltrate and the contact time with the resin (34). An endogenous ultrafiltrate flow >60 ml/min is therefore not currently allowed by the Supra-HFR System as also reported by other authors (26-28).
Lastly, even considering the higher costs of Supra-HFR compared to OL-HDF (about 50 €/session vs. 25 €/session, respectively), it should be underlined that Supra-HFR can represent a valid option in some cases, because it can overcome the limitations arising from a malfunctioning vascular access (35-37).
Our hypothesis that the use of Supra-HFR might be better than OL-HDF with suboptimal convective replacement volume was not confirmed by our results. This study did not include experiments; its explorative design and the small number of cases investigated restrict generalization and prevent us from drawing firm conclusions at present. In particular, the limited sample size precluded the possibility to test the assumption of normality and to apply parametric tests, thus most of our data are given as median with IQR. Other limitations include the restriction of the marker molecules assessed and the lack of a randomization.
However, balancing strengths and weaknesses, we can conclude that this study represents a “real-life” observation of the efficiency of Supra-HFR in patients with several comorbidities and after the administration of drugs commonly in use during hemodialysis. Further studies, carried out on a larger population and analyzing the longterm effects of Supra-HFR, are required to better assess its efficiency and benefits in uremic patients who require an efficient removal of the middle molecular weight molecules.
Acknowledgements
The Authors are grateful to Dr. Bianca Gualandi for revising the article.
Footnotes
Authors’ Contributions
Conceptualization, writing, original draft preparation: G.D., A.A., M.C.; methodology on nephrological aspects: C.G., A.S.; data collection: L.G.; M.Z.; M.M.; methodology on laboratory: C.D.; main supervision: G.L.M. All Authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
The Authors declare no conflicts of interest in relation to this study.
- Received March 25, 2022.
- Revision received April 21, 2022.
- Accepted April 26, 2022.
- Copyright © 2022, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.