


Abstract
Background/Aim: This is a report of the first clinical implementation of 99mTc-labeled diethylene triamine pentaacetate-galactosyl human serum albumin (99mTc-GSA) single-photon emission computed tomography (SPECT) image-guided inverse planning into palliative radiotherapy (RT) for diffuse liver metastases. Case Report: A 48-year-old man developed chemo-refractory diffuse liver metastases from thymic carcinoma characterized by abdominal pain and distension. Palliative RT was performed with a total dose of 20 Gy in five fractions using double arc volumetric modulated arc therapy to reduce the dose to functional liver defined by 99mTc-GSA SPECT images. His symptoms were immediately relieved after RT and did not experience radiation-induced liver disease. Both Functional Assessment of Cancer Therapy (FACT)-G and FACT-Hep total scores improved after 2 weeks of RT initiation and did not become worse than baseline scores. Conclusion: The 99mTc-GSA SPECT image-guided palliative RT is an effective and safe treatment for patients with diffuse liver metastases.
- Metastatic liver tumor
- radiotherapy
- palliative treatment
- volumetric modulated arc radiotherapy
- single-photon emission computed tomography
- functional imaging
The liver is one of the most common sites of tumor metastases (1). Local treatment, such as surgery and radiotherapy (RT) with or without systemic therapy, has been performed for the limited size and number of lesions; however, patients frequently progress to end-stage disease because of disease refractory to systemic therapy (2). Such cases have diffuse liver metastases and the liver parenchyma is replaced by metastatic tumors (3). Diffuse liver metastases often cause liver dysfunction and symptoms, such as abdominal pain and distension, nausea, and vomiting (2). Traditionally, low-dose whole liver RT has been performed as a palliative treatment for diffuse liver metastasis. More intensive RT dose prescription is preferable for better palliative effect; however, it is difficult because of the lower dose tolerance limit of the whole liver (4).
The combined use of single-photon emission computed tomography (SPECT) and 99mTc-labeled diethylene triamine pentaacetate-galactosyl human serum albumin (99mTc-GSA), which specifically binds to the asialoglycoprotein receptor in the liver, provides three-dimensional information about regional liver function (5). A recent study suggested that introduction of the functional information of 99mTc-GSA SPECT into inverse RT planning identifies the dosimetric benefits for the target volume coverage and sparing of the functional liver (6, 7). In this case report, 99mTc-GSA SPECT image-guided inverse planning was implemented for the first time into palliative RT for diffuse liver metastases in clinical practice.
Case Report
Clinical findings. A 48-year-old man was diagnosed with thymic carcinoma, cT4N2M0 Stage IVB, 3 years before presentation. He underwent surgery but still developed lymph node, pleural, and thoracic wall metastases 5 months postoperatively. He underwent chemotherapy and RT for brain and bone metastases; however, liver metastases occurred 2 years postoperatively. His liver metastases were chemo-refractory, which resulted in abdominal pain and distension. Therefore, functional preservation palliative RT was planned as a treatment option for diffuse liver metastases in addition to low-dose whole liver RT and observation. After obtaining a full informed consent, 99mTc-GSA SPECT image-guided palliative RT was performed.
RT treatment planning. 99mTc-GSA SPECT/Computed tomography (CT) and planning simulation CT imaging were performed. The detailed SPECT/CT imaging procedure is described elsewhere (5-7). For the planning simulation CT imaging, a Discovery RT CT scanner was used (GE Healthcare, Chicago, IL, USA). Four-dimensional CT images were obtained at 120 kV, 70 mA, 0.5 s rotation, and 2.5 mm slice thickness (8, 9). The average intensity projection (AIP) of CT images was generated from the projection data of all respiratory phases.
SPECT/CT and planning AIP of CT images were exported to Velocity AI (version 3.2.1; Varian Medical Systems, Palo Alto, CA, USA). After SPECT and CT images were registered by hardware arrangement, fused planning CT and SPECT/CT images were generated through the CT–CT rigid registration (5-7). The optimization of the functional liver structure (FLS) was decided using a SPECT threshold at 60% of the maximum pixel value (6). FLS was confirmed to adequately cover non-cancerous liver parenchyma. Planning CT images with FLS were transferred to the RT treatment planning system (Eclipse version 15.6; Varian Medical Systems). Structures of the target volume and organs at risk (OARs) were delineated on planning CT images. A gross tumor volume was defined as metastatic liver tumors. An internal target volume (ITV) based on the AIP images was defined as the whole liver minus FLS. Isotropic planning target volume margins of 5 mm were added to the ITV. The RT plan was created to use a double arc volumetric modulated arc therapy (VMAT) with photon energy of 6 MV using a linear accelerator (Clinac iX; Varian Medical Systems). The total prescribed dose was 20 Gy in five fractions. The FLS dose was reduced as low as possible (Figure 1). Image-guided RT based on the cone-beam CT was performed for irradiation.
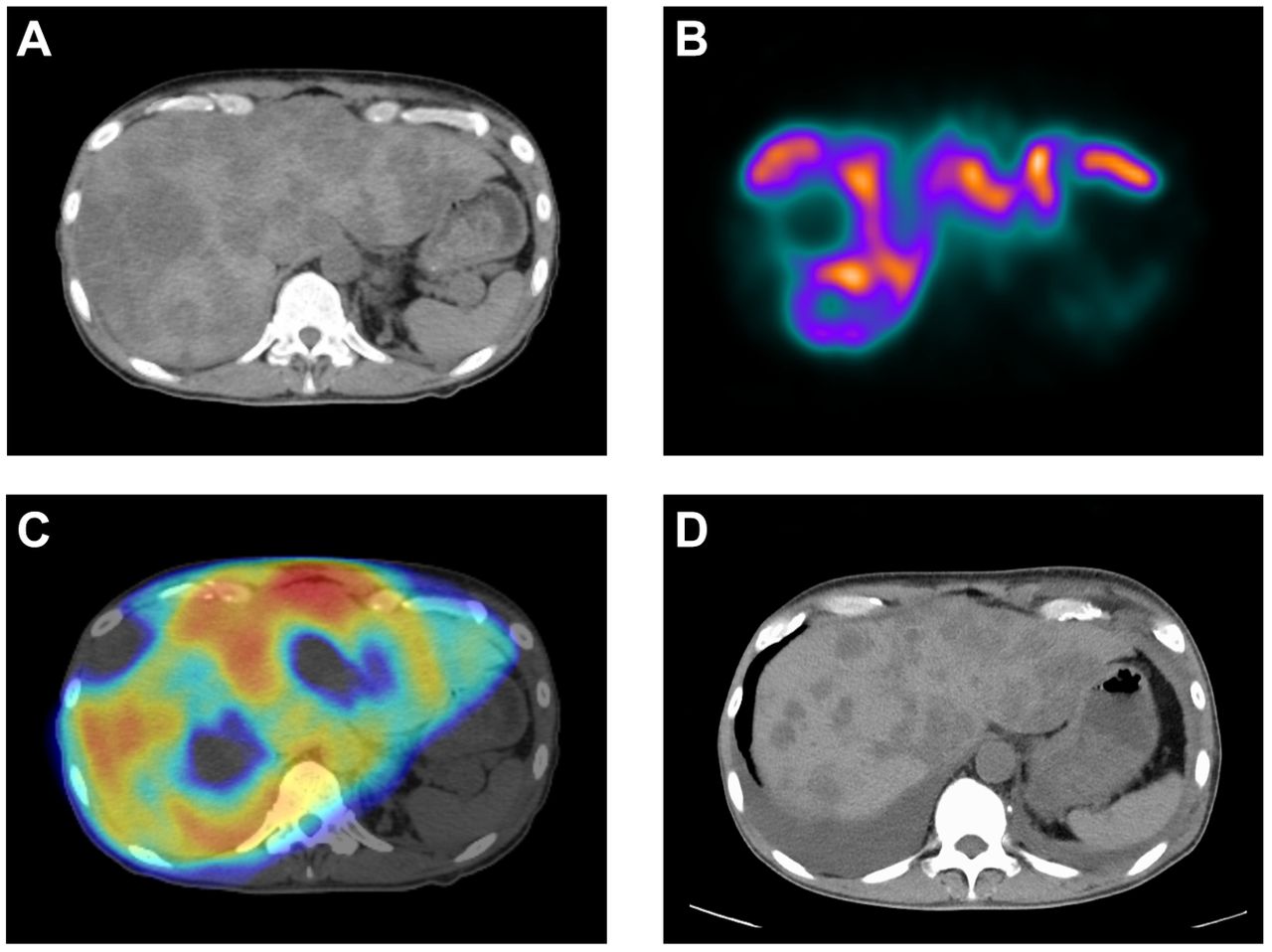
Computed tomography (CT) and 99mTc-labeled diethylene triamine pentaacetate-galactosyl human serum albumin (99mTc-GSA) single-photon emission computed tomography (SPECT) images. (A) Planning CT simulation image. The volume of the whole liver was estimated based on diagnostic CT was 3,593 cm3. (B) 99mTc-GSA SPECT image. Liver metastases and non-cancerous liver parenchyma (functional liver) can be easily distinguished. (C) Dose distribution of the volumetric modulated arc therapy. Dose to non-cancerous liver parenchyma was reduced by inverse planning. (D) Diagnositic CT image at 5 weeks after radiotherapy. Tumor response and volume reduction of the whole liver were observed. The volume of the whole liver was 2,754 cm3.
Patient outcome. His symptoms were relieved immediately after RT. Blood test and Functional Assessment of Cancer Therapy (FACT) questionnaire results are shown in Table I and Table II, respectively. After the RT initiation, liver function test values had improved for approximately 4 weeks. Both FACT-G and FACT-Hep total scores had improved after 2 weeks of the RT initiation and did not become worse than baseline scores. CT images at 5 weeks after RT revealed tumor shrinkage and volume reduction of the whole liver (Figure 1). After 7 weeks of the RT, chemotherapy was discontinued, and the patient died due to pulmonary lymphangitic carcinomatosis a week after.
The blood test results before and after palliative radiotherapy.
The results of Functional Assessment of Cancer Therapy Questionnaire before and after palliative radiotherapy. The higher the score, the better the quality of life.
Discussion
Although low-dose whole liver RT is one of the treatment options for diffuse liver metastases, the palliative effect is insufficient. RT of 20-30 Gy with fraction size of 1.5-3 Gy has been traditionally performed for diffuse liver metastasis. Symptom relief was achieved in approximately 55%-70% of the treated patients (10, 11). Since the 2000s, hypofractionated RT had been used to treat diffuse liver metastases. Bydder et al. analyzed 28 patients prospectively treated with whole- or partial liver palliative RT with a total RT dose of 10 Gy with a fraction size of 5 Gy for the symptomatic liver metastases (12). Symptom responses were obtained in approximately 55%-65% of patients. Soliman et al. performed a phase II study of the whole liver RT with 8 Gy in one fraction for 41 patients with hepatocellular carcinoma or liver metastasis symptoms. At 1 month, 48% of patients achieved an improved symptom. Higher RT dose prescription may yield more palliative effects.
The primary difficulty in more intensive treatment with high RT dose prescription for diffuse liver metastases is due to the lower dose tolerance limit of the whole liver; the estimated tolerance doses of the whole liver are suggested to be 30 Gy in 2-Gy fractions and 21 Gy in 3-Gy fractions (2, 4). As the tolerance dose of partial irradiation of the liver is higher than the whole liver irradiation because of the volume effect, intensive and effective treatments can be realized using the selective RT dose to the target volume (4, 13); however, it had been technically difficult because of the following two technical problems: difficulty in extracting liver metastases and non-cancerous liver parenchyma from the whole liver in conventional CT images and difficulty in irradiating liver metastases while reducing the dose to non-cancerous liver parenchyma by two- or three-dimensional conformal RT based on forward planning because the shapes of these structures are very complex and adjacent with each other. A recent technical development can resolve these problems. The former problem can be resolved by introducing 99mTc-GSA SPECT images into RT planning CT images, which can easily define both liver metastases and non-cancerous liver parenchyma based on the setting threshold value (5-7). The latter problem can be resolved by intensity-modulated RT or VMAT based on inverse planning that allows dose escalation to the target volume while reducing the dose to OARs (8). We believe that the combination of these techniques promises more effective palliative treatment effects than conventional low-dose whole liver RT without developing radiation-induced liver disease in patients with diffuse liver metastases.
In summary, we reported the first clinical implementation of 99mTc-GSA SPECT image-guided inverse planning into palliative RT for diffuse liver metastases. This novel approach is an effective and safe treatment for patients with diffuse liver metastases.
Acknowledgements
This work was supported by JSPS KAKENHI Grant Number 21K07180.
Footnotes
Authors’ Contributions
RT developed the project, treated the patient, performed radiotherapy planning, analyzed and interpreted data, and wrote the manuscript. TW and S.Saeki treated the patient. YK and YS performed radiotherapy planning. TM, YF, and TM developed the project. S. Shiraishi developed the imaging protocol. TS, TH, and NO supervised the project. All Authors have read and approved the final manuscript.
Conflicts of Interest
The Authors declare that they have no conflicts of interest regarding this study.
- Received March 3, 2022.
- Revision received March 26, 2022.
- Accepted March 28, 2022.
- Copyright © 2022, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).




{kind=link}