


Abstract
Background: Comorbidity and frailty are relevant limitations of normofractionated combined radiochemotherapy for squamous cell head and neck cancer (HNSCC), especially in elderly patients. This retrospective study aimed to evaluate the efficacy and toxicity of moderately hypofractionated radiotherapy (HRT) without chemotherapy in patients ineligible for concurrent radiochemotherapy. Patients and Methods: Between 2011 and 2018, 51 elderly/frail patients with HNSCC were treated with either definitive (n=23) or adjuvant (n=28) moderate HRT. A dose of 45 Gy was given to the primary tumour region and cervical nodes with a sequential boost up to 50 in the adjuvant and 55 Gy in the definitive cure setting (2.5 Gy/fraction). Patient outcomes of locoregional control, overall survival, and acute and late toxicity were analysed. Results: After a median follow-up of 6 months for the definitive HRT group and 28.5 months for the adjuvant HRT group, we found a median overall survival of 6 vs. 55 months (log-rank test: p<0.001) and a median locoregional control of 9 months vs. not reached (log-rank test: p=0.008), respectively. The 2-year rates of locoregional control were 28.5% for the definitive HRT group vs. 75.2% for the adjuvant HRT group. No acute or late grade 4-5 toxicity occurred; grade 3 toxicity was rarely documented. Conclusion: HRT in elderly/frail patients with HNSCC who are unfit for chemotherapy leads to acceptable local control with moderate toxicity in a short overall treatment time. Especially in the postoperative situation, HRT can be considered an appropriate alternative to normofractionated radio(chemo)therapy. Definitive HRT can be a treatment alternative, especially for multimorbid patients.
- Squamous cell head and neck cancer
- moderately hypofractionated radiotherapy
- elderly patients
- adjuvant radiotherapy
- definitive radiotherapy
Head and neck cancer represents the sixth most common malignant tumour worldwide, with an annual incidence of approximately 630,000 new cases diagnosed per year (1). In Germany, head and neck cancer was responsible for 17,500 cases according to data available from 2017 (2). In addition to tobacco and alcohol consumption, infection with high-risk types of human papillomavirus is an exogenous risk factor (3). More than 90% of cases are squamous cell carcinomas (HNSCCs), mostly presenting as locally advanced disease with lymph node metastases (1, 4). Tumours without distant metastases are treated with curative intent. Apart from surgery (followed by adjuvant radio(chemo)therapy for locally advanced tumours), definitive radiochemotherapy is also recommended for curative-intent treatment, mainly for inoperable, locally advanced cases (5).
Due to physical and pharmacokinetic changes, a high burden of comorbidities and possibly increased toxicity, the choices of chemotherapy are limited in elderly and frail patients (6). The selection of treatment in these patients should be based primarily on comorbidities and functional status rather than on age (7). Moderately hypofractionated radiotherapy (HRT) alone can be a therapeutic approach in this subset of patients, as tumour regression can be achieved within a short overall treatment time with moderate toxicity. HRT is already a successfully established therapy for localized prostate cancer and is an adjuvant breast cancer treatment (8-12). Concerning head and neck cancer, some studies have already shown that the use of moderately HRT is feasible in terms of local control and toxicity (13-18). Based on these encouraging data, we conducted a retrospective study to analyse whether moderate HRT is an appropriate treatment alternative for elderly and frail patients deemed unfit for chemotherapy. The purpose was to evaluate locoregional control (LRC), overall (OS), and acute and late treatment-related toxicities in both definitive and adjuvant settings.
Patients and Methods
Between January 2011 and October 2018, 51 patients with HNSCC without distant metastases received either definitive (n=23) or adjuvant (n=28) moderately HRT at the Department of Radiation Therapy and Special Oncology, Hanover Medical School. All patients were allocated to moderately HRT due to age, comorbidity, or refusal of chemotherapy. All patients in the definitive group had an indication for concurrent chemotherapy but were unable to receive it because of advanced age (10 patients), comorbidities (9 patients) or refusal (4 patients). In the adjuvant group, five patients did not have an indication for simultaneous chemotherapy because of negative resection margins and negative lymph node status or lymph nodes without extracapsular spread. As a consequence of positive lymph node status with extranodal spread, extranodal spread or positive resection margins, all other patients had an indication for concurrent chemotherapy. However, they were unable to receive chemotherapy due to age (11 patients), comorbidities (5 patients) or refusal (7 patients). All patients had passed an inhouse interdisciplinary board of otolaryngologist, radiologist, radiotherapist, pathologist, and medical oncologist. Not only age but also the high burden of comorbidities and poor performance status were reasons for these patients to be considered frail. Therefore, the individual burden of comorbidities was quantified with the Charlson Comorbidity Index (CCI). Diseases such as diabetes, myocardial infarction, heart failure, peripheral artery disease, additional tumours, liver diseases and age are captured by the CCI (19). All patients were classified according to the seventh edition of the Union for International Cancer Control TNM classification (20). Three patients in the definitive group and two in the adjuvant group withdrew consent for RT soon after beginning it and were included in the analysis. All included patients received the planned radiation dose. Twenty-two percent of the definitive HRT group and 21% of the adjuvant HRT group had a percutaneous endoscopic gastrostomy tube in place before the start of RT. The patient characteristics are summarized in detail in Table I.
Patient characteristics by treatment regimen.
Data on patient characteristics, radiation treatment plans and follow-up were obtained retrospectively from databases of established practices and the Departments of Radiation Oncology, Otolaryngology and Oral and Maxillofacial Surgery of Hanover Medical School. The Institutional Ethics Committee reviewed and approved the completion of this study, waiving the need for ethical approval due to anonymisation of patient data.
RT was delivered by a linear accelerator (Versa HD or Synergy; Elekta, Stockholm, Sweden) using 3D conformal or (after 2016) volumetric modulated arc therapy. Moderate HRT was defined as a single 2.5-Gy dose. In the definitive group, the primary tumour and cervical bilateral lymph nodes received a total dose of 45 Gy, and an additional sequential boost (primary and involved nodes) up to a cumulative dose of 55 Gy was applied. The adjuvant group’s treatment consisted of 45 Gy to the former tumour bed and cervical lymphatic drainage area, followed by a sequential boost (to the former primary tumour region and the involved neck regions with extracapsular spread) up to a total dose of 50 Gy. Patients were immobilized using a custom-made thermoplastic mask (ITV-Völp, Innsbruck, Austria). All treatment plans were calculated using Monaco software (Elekta).
The gross target volume enclosed the primary tumour and pathological lymph nodes. The clinical target volume consisted of the gross target volume plus a 5-mm margin and the cervical lymphatic pathways. The planning target volume included the clinical target volume plus a 4-mm margin.
Patients’ acute side-effects were recorded weekly during RT. A clinical evaluation regarding the tumour response and late toxicity was performed every 3 months after the completion of RT in the Departments of Radiation Therapy, Oral and Maxillofacial Surgery, or Otolaryngology, as well as in established local practices. Acute toxicity was categorized according to Common Terminology Criteria for Adverse Events v. 4.03 (21), and late side-effects were classified by the LENT-SOMA score (22).
The endpoints of the study were LRC, OS, and acute and late toxicity. LRC was defined as the time from the first day of treatment to local or regional progression, or recurrence. OS was defined as the time from the first day of RT to death from any cause. Descriptive statistics were used to summarize the patient characteristics and toxicity. Survival rates were calculated using the Kaplan-Meier method. The OS and LRC differences between the two groups were compared using the log-rank test. Statistical significance was defined as p<0.05. Statistical analysis and graphics were conducted with SPSS Statistics 26.0 (IBM, Armonk, NY, USA).
Results
The median follow-up was 6 months (range=1-38 months) for the definitive HRT group and 28.5 months (range=1-87 months) for the adjuvant group. At the time of the analysis, two patients in the definitive group and eight in the adjuvant HRT group were still alive, while 14 and 11 patients, respectively, had died from their tumours, whilst three and six patients had died from comorbidities. Four patients in the definitive HRT group and three in the adjuvant HRT group were lost to follow-up.
The median OS was 6 months (range=3.9-8 months) for the definitive HRT group and 55 months (range=24.6-85 months) for the adjuvant HRT group. For the definitive HRT group, the 1-year and 2-year OS rates were 26.3% and 15.8%, respectively, while they were 84% and 63.2%, respectively, for the adjuvant HRT group.
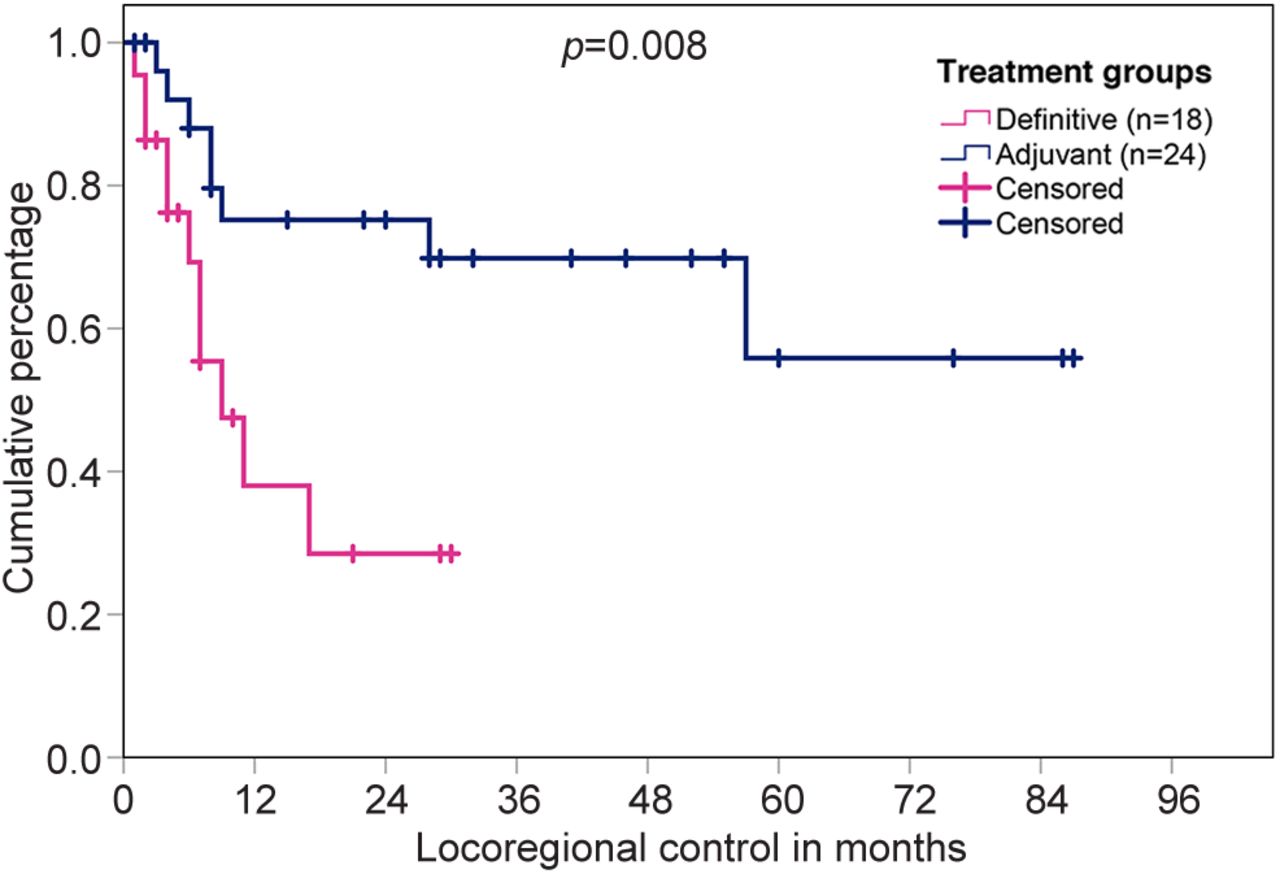
The median LRC was 9 months (range=3-15 months) for the definitive HRT cohort. In this group, 11 patients (47.8%) had locoregional progression, nine developed distant metastases, and six developed a second primary cancer (three lung, one breast, one anal, and one unknown primary). The 1- and 2-year LRC rates were 38% and 28.5%, respectively.
In the adjuvant HRT group, locoregional recurrence occurred in eight patients (28.6%), nine (32.1%) developed distant metastases, and three developed a second primary tumour (two lung and one malignant melanoma). The LRC rates were 75.2% at 1 and 2 years.
The log rank-test was used to evaluate the differences regarding OS and LRC between the two treatment groups. As shown in Figure 1 and Figure 2, OS (p<0.001) and LRC (p=0.008) were significantly better for those treated with adjuvant HRT.
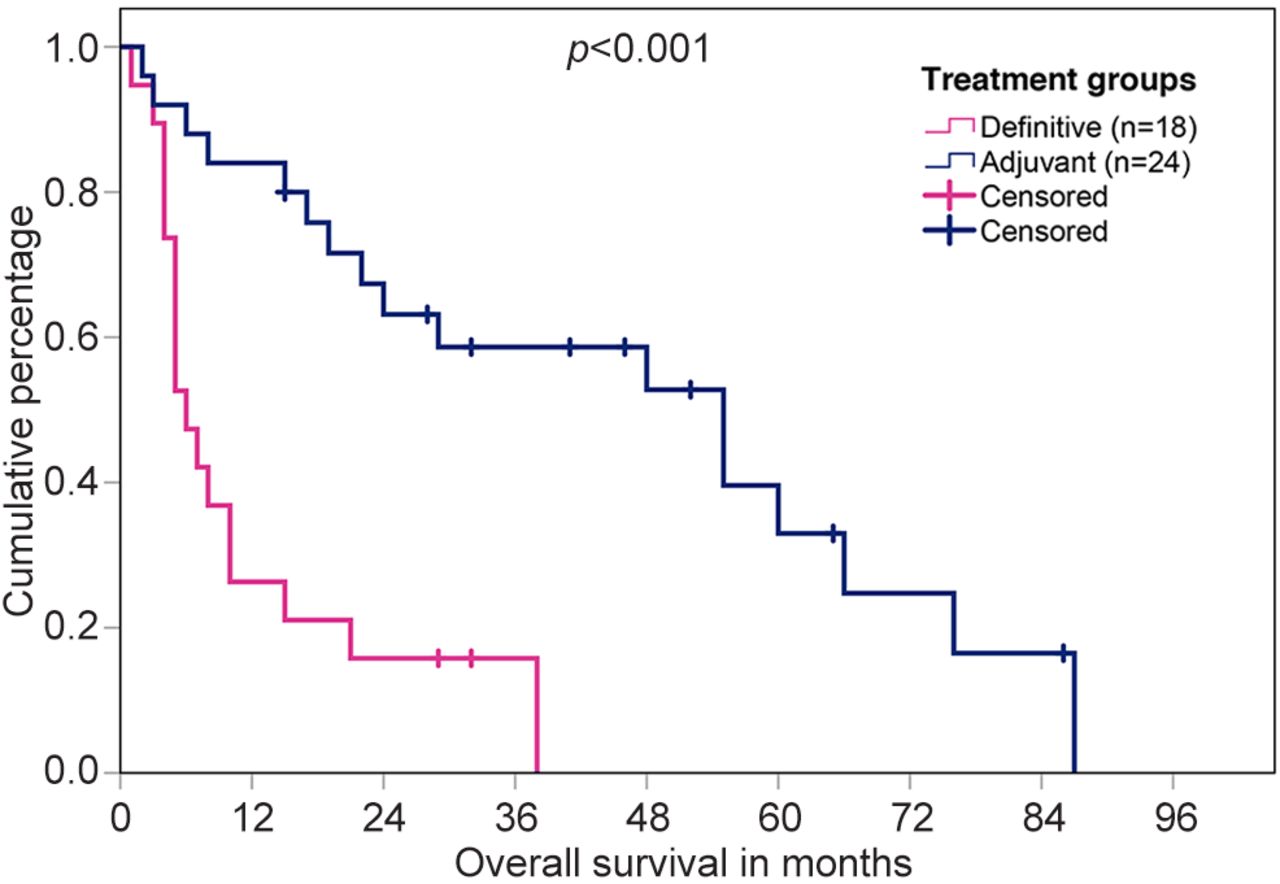
Kaplan-Meier analysis for overall survival in the definitive and adjuvant hypofractionated radiotherapy groups.

Kaplan-Meier analysis for locoregional control in the definitive and adjuvant hypofractionated radiotherapy groups.
Side-effects are reported in Table II. None of the patients developed grade 4 or 5 adverse events. Prior to RT, three patients in the definitive group and four in the adjuvant group suffered from hoarseness. Except for one patient in the definitive HRT group, the severity of their symptoms decreased under irradiation: 95.7% with grade zero hoarseness in the definitive group and 96.4% with grade zero hoarseness in the adjuvant HRT group. The most common acute toxicities were grade 1 dermatitis (56.5% in the definitive HRT group vs. 78.6% in the adjuvant HRT group) and grade 1-2 mucositis (82.6% in the definitive HRT group vs. 75% in the adjuvant HRT group). Grade 3 acute toxicities were rarely documented; the incidence of grade 3 dysphagia was 21.7% in the definitive HRT group and 21.4% in the adjuvant HRT group. Three patients in the adjuvant HRT group and one in the definitive HRT group suffered from grade 3 oral mucositis.
Acute hypofractionated radiotherapy (HRT)-related toxicity according to Common Terminology Criteria for Adverse Events version 4.03 (21).
As shown in Table III, late toxicities of grade 3 were rarely observed. In the definitive HRT group, grade 3 dysphagia was found in two patients, and grade 3 hoarseness was found in one patient. In the adjuvant HRT group, grade 3 osteoradionecrosis occurred in two patients
Late hypofractionated radiotherapy (HRT)-related toxicity according to LENT-SOMA tables (22).
Discussion
Approximately 50% of untreated patients with head and neck cancer die within 4 months from advanced disease (23). Historically, definitive RT has been used as the principal treatment option for patients with inoperable disease, achieving LRC rates of 50 and 70% and 5-year survival rates of 10-30% (24, 25). However, the prognosis of patients with locally advanced disease after RT alone remains poor: After 5 years, only 30-35% of patients are still alive (26). Since most patients die due to locoregional progression, several treatment alternatives have been tested to improve tumour response.
Regarding RT alone, accelerated hyperfractionated irradiation has been shown to be superior to normofractionated irradiation in terms of local control and OS (27, 28). However, in terms of toxicity, hyperfractionation is significantly more toxic (27, 29). Meta-analyses have shown a survival benefit for the addition of cisplatin-based chemotherapy to definitive RT in locally advanced HNSCC (30, 31). According to Pignon et al., OS is improved by 4.5% at 5 years regardless of the type and timing of chemotherapy, and concomitant chemotherapy leads to a survival benefit of 6.5% at 5 years (30). In the primary setting, the epidermal growth factor receptor (EGFR) antibody cetuximab is an alternative to concomitant chemotherapy. After 3 years, an absolute improvement in OS of 13% was shown (32). This is thought to be due to radiosensitizing effects in tumour cells with EGFR overexpression (33).
In the postoperative situation, risk factors such as advanced tumour stage, positive resection margins or a positive lymph node status often led to the recurrence of advanced HNSCC after surgery alone (34, 35). Therefore, the use of adjuvant RT is recommended to reduce the local recurrence rate and thus improve OS (34-37). Mostly, these are conventional fractionated RT regimes (38-41). At 5 years, survival rates of 30-45% can be achieved (40-42). However, patients with close surgical margins and extracapsular extension of nodal disease should also receive concomitant cisplatin-based chemotherapy in the postoperative situation. With 5-year survival rates of 53-64%, there is a significant benefit in terms of local control and OS in favour of postoperative combined radiochemotherapy (38, 41, 43).
For elderly and frail patients, as was the case in our study, neither combined radiochemotherapy nor hyperfractionated accelerated irradiation nor concomitant EGFR therapy can be considered a suitable therapeutic approach. Due to their poor general condition and multiple morbidities, moderate HRT alone was the only therapeutic option for our subset of patients from our point of view, as irradiation in these patients needed to be carried out within the shortest possible treatment time with the lowest possible toxicity. From a logistical point of view, a reduced number of fractions minimizes the burden of daily trips for treatment.
Based on the advantages mentioned above, selected elderly and frail patients received either definitive or adjuvant therapy with a moderate HRT scheme in our study. By doing so in the definitive setting, we achieved reasonable LRC rates comparable to those in the literature. Nevertheless, the OS rates were rather poor. The toxicity was acceptable and quite comparable to the grades of acute toxicity reported in other HRT studies (13, 15, 16, 44, 45). Regarding late toxicity, eight patients in the definitive HRT group and seven in the adjuvant HRT group were lost to follow-up due to impaired mobility, frailty, or non-compliance.
Al-Mamgani et al. observed even higher rates of acute toxicity (grade ≥3 skin and mucosal toxicity of 45% and 65%, respectively) using an HRT regimen consisting of 50 Gy applied in 16 fractions of 3.125 Gy (13), presumably due to a higher biological equivalent dose. They also described acceptable response rates and good symptom control in patients unsuitable for combined radiochemotherapy or surgery. Furthermore, disease-free and OS rates were lower patients for burdened with major comorbidities (32% and 23% at 1 year, respectively). Our observations confirm this, as our multimorbid cohort reached similar LRC and OS rates. Agarwal et al. evaluated 40 Gy in 16 fractions (2.5 Gy each) as an effective treatment approach for symptom control for patients with advanced stage HNSCC, achieving a 1-year progression-free survival rate of 55.1% (16). Lok et al. treated patients with incurable head and neck cancer using the QUAD-shot regimen: the treatment consisted of three cycles of 3.7 Gy delivered twice a day over 2 days per cycle up to a total dose of 44.4 Gy. They achieved a median OS of 5.7 months (44). Similar results were found in our study. Bonomo et al. treated elderly patients unfit for standard curative treatment with 40 Gy in 16 fractions (2.5 Gy per fraction). The 1-year LRC and OS rates were 28% and 50%, respectively (15). In this way, they verified that moderate HRT was able to improve LRC and thus achieve a longer OS in this frail subset of patients. While the 1-year LRC (38%) was higher for our definitive cohort, the 1-year OS rate of 26.3% was lower, presumably due to a higher proportion of tumour entities that have poor outcomes, such as hypopharyngeal cancer.
Only a few studies have examined HRT schemes in the postoperative setting (17, 18). In the study of Mastronikolis et al., 50 Gy in 20 fractions (2.5 Gy per fraction) were given postoperatively to 73 patients with advanced HNSCC, and 2-year LRC and OS rates of 70% and 65% were found, respectively (18). With an LRC rate of 75.2% and an OS rate of 63.2% at 2 years, we achieved comparable results. Unfortunately, Mastronikolis et al. did not provide any acute toxicity data. Tobias et al. achieved a 1-year OS of 75% and a 2-year OS of 60% in the group that received postoperative RT alone (17). The 2-year OS (63.2%) was comparable in our group, but the 1-year OS (84%) was better. Our LRC rate of 75.2% at 1 and 2 years was better than their corresponding event-free survival rates of 62% and 55%, respectively. However, it should be noted that event-free survival includes not only LRC but also overall recurrence, second primary disease, and death from other causes. This might be a reason why their event-free survival rate was lower than our LRC rate. Tobias et al. included both conventional and HRT schemes in their analysis. An interesting aspect is that we achieved almost the same median OS (5 vs. 4.6 years for our group) and higher OS and LRC rates using solely HRT schemes. Especially in this frail subset of patients burdened with many comorbidities, this might be an approach to obtain similar results in a shorter overall treatment time. Regarding acute toxicity, our RT scheme led to equivalent results.
Table IV gives an overview of our data concerning oncological results (OS, LRC) and toxicity in comparison to the literature.
Studies of hypofractionated radiotherapy (HRT), for head and neck tumours organized by definitive/adjuvant setting.
Nevertheless, several limitations must be considered when interpreting our data: All of the data were collected retrospectively, and the small sample size of both cohorts may have limited the power of our results.
In summary, the present study shows that moderate HRT in elderly and frail patients with HNSCC who are unfit for chemotherapy leads to acceptable local control with moderate toxicity in a short overall treatment time. Especially in the postoperative adjuvant situation, our RT regimen can be considered an appropriate alternative treatment to normofractionated radio(chemo)therapy for this patient cohort. Definitive HRT can be a treatment alternative, especially for multimorbid patients. Treatment of patients with advanced HNSCC who are unfit for standard therapy remains challenging. Particularly with regard to the definitive treatment setting, future investigations are required.
Acknowledgements
The Authors acknowledge support by the German Research Foundation (DFG) and the Open Access Publication Fund of Hannover Medical School (MHH).
Footnotes
Authors’ Contributions
Conceptualization, AF, RM and HC; methodology, AF and RM; software, AF; formal analysis, AF and IB; writing-original draft preparation, AF; writing-review and editing, RM, JW, FT, MD and HC. All Authors read and agreed to the published version of the article.
Conflicts of Interest
The Authors declare that they have no competing interests.
- Received February 5, 2022.
- Revision received March 1, 2022.
- Accepted March 10, 2022.
- Copyright © 2022, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.