


Abstract
Background/Aim: COVID-19 started to spread as a pandemic in December 2019 and COVID-19 vaccination has been initiated worldwide. The efficacy of vaccination has been scientifically proven, but it might cause axillary lymph node swelling. To diagnose patients with axillary lymph node swelling caused by COVID-19 vaccination, we herein reviewed existing literature on this symptom. Case Report: We report the case of a 70-year-old woman with a breast tumour. She had undergone cecum cancer surgery and regular computed tomography (CT). During breast tumour follow-up, she received scheduled CT that indicated severe axillary lymph node swelling mimicking breast cancer metastasis. We performed aspiration biopsy cytology of that lymph node, and determined this was not cancer metastasis but an effect of the COVID-19 vaccine. We confirmed this diagnosis at one month after computed tomography showed that the lymph node swelling had improved. Conclusion: Axillary lymph node swelling can occur after COVID-19 vaccination. Therefore, it is important to consider the effect of the COVID-19 vaccination on axillary lymph node swelling when diagnosing breast tumours.
SARS-CoV-2 infection disease was first reported in Wuhan in December 2019 (1) and we are still in effect of this pandemic both in Japan and globally. Of note, cancer patient diagnoses and treatment are being formed under these pandemic conditions. SARS-CoV-2 vaccines were rapidly developed, including the mRNA vaccine (2), which has specific side-effects including fever, general fatigue, and upper arm swelling in the region of the vaccine injection.
In Japan, the vaccination of medical staff and elderly people started in February 2021. Currently, there are increasing numbers of people who have received vaccination twice. Therefore, the chance of encountering double vaccinated people in daily clinical practice is increasing. There are some guidelines for the timing of the vaccine injection for cancer patients, such as the National Comprehensive Cancer Network guidelines (3), but it is still not clear how these vaccines might influence cancer diagnosis and treatment, especially for breast cancer. Herein, we present a case with severe axillary lymph node swelling thought to be caused by the COVID-19 vaccine injection, which was similar to breast cancer metastasis observed by computed tomography (CT), and present a literature review of the effect of COVID-19 vaccination on axillary lymph nodes.
Case Report
The patient was a 70-year-old woman who was diagnosed with cecum cancer in December 2019, and who underwent surgery in February 2020. The pathological finding was adenocarcinoma, t=25 mm, with no lymph node metastasis. She received no adjuvant therapy. A follow-up of cecum cancer by enhanced CT in July 2020 indicated a left breast tumour. Then, she was introduced to the breast surgery clinic. She had no palpated mass, had focal asymmetric density in the left upper outer quadrant of the mammogram, and the tumour in her left breast appeared benign by ultrasonography at the first visit to the breast surgery clinic. We planned a follow up. On June 2021, she received an enhanced CT to check for distant metastasis related to cecum cancer, and severe swelling of levels I and II was observed in the axillary lymph node (Figure 1A and B). However, the tumour in her left breast did not get larger. We considered that precise checking was required, so we called her to the breast surgery clinic earlier than originally suggested. She came to our clinic in July 2021, 2 weeks after undergoing CT.

Enhanced computed tomography (CT) (June 2021) shows severe axillary lymph node swelling mimicking breast cancer metastasis at level I (B) and level II (A).
The patient underwent a medical interview and we performed local palpation, mammogram, and ultrasonography. In addition, we performed aspiration biopsy cytology (ABC) of the left breast tumour and the swollen left level I axillary lymph node. The medical interview indicated that 3 days before she underwent the CT, she received a second COVID-19 vaccination on her left upper arm and developed low grade fever, upper arm pain, and swelling as a side effect of the vaccination. Local palpation indicated no abnormalities and there was no palpable lymph node in her left axilla. The mammogram showed a left upper outer mass that had not changed from one year before retrospectively (Figure 2A and B). Ultrasonography showed the left breast mass had not changed in size or shape from one year before (Figure 2C); however, it indicated a new swollen left axillary lymph node (Figure 2D and E). Except for this swollen lymph node of level II, the appearance of most lymph nodes indicated they were undergoing an inflammatory response because they maintained the structure of the cortex and medulla. The ABC of the breast tumour specimen was inadequate and it was negative for the axillary lymph node. A blood exam performed on the same day as the enhanced CT in June 2021 showed CRP was slightly high at 1.82. We diagnosed the swollen lymph nodes as a vaccine side-effect. We planned to follow-up the patient as before. We also performed a simple CT to check the axillary lymph nodes on the same day as these precise checks in July 2021 and found the swelling had improved (Figure 3A and B).
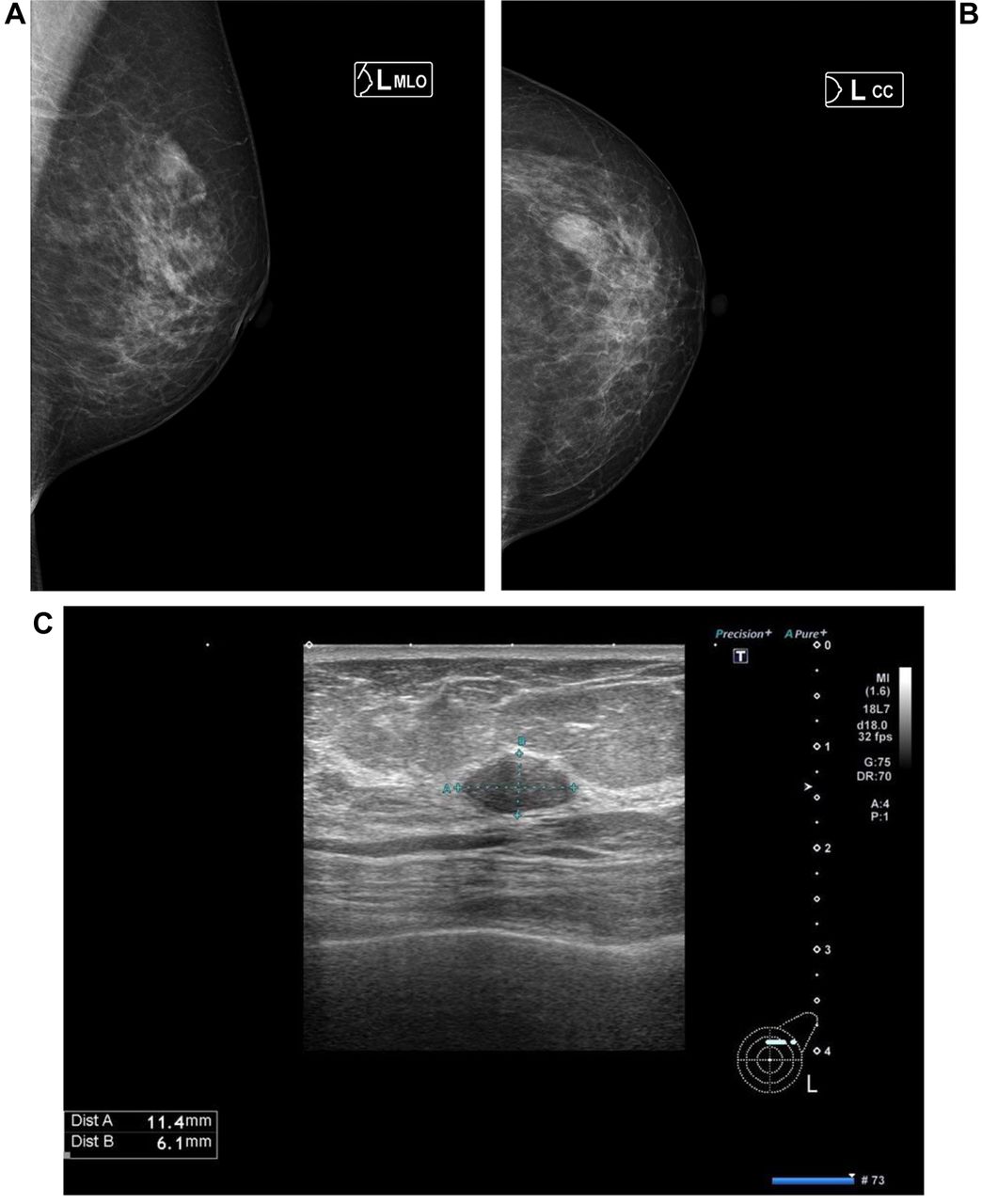

Mammogram and ultrasonography (July 2021). The mammogram shows a left upper outer mass (A, B). Ultrasonography (US) shows an oval mass in the left C area (C) and lymph node swelling at level I (D) and level II (E). We performed US guided aspiration biopsy cytology for this breast mass and level I lymph node.

Simple computed tomography (CT) (July 2021) shows the axillary lymph node swelling had improved at both level I (B) and level II (A).
Written informed consent was obtained from the patient for the publication of this Case Report and any accompanying images. This was a case report and therefore we did not require additional permission from our review board.
Discussion
In Japan, the number of COVID-19 patients increased again in July 2021, which was called “the 5th wave” in the Tokyo metropolitan area. Of note, the COVID-19 vaccine injection became popular among elderly people. Although the number of COVID-19 patients is increasing, the number of elderly patients is decreasing. The COVID-19 vaccine is the first approved mRNA vaccine and although it reduces the risk of COVID-19 infection (2) it causes specific side-effects such as fever, general fatigue, and upper arm swelling that have not been experienced with other vaccines. In breast tumour diagnosis, axillary lymph node information is very important; if they are swollen it is important to determine whether they are malignant. When we encountered this patient, it was not well known in Japan that axillary lymph node might swell after COVID-19 vaccination. This was the main reason of misconception for this patient. From this point of view, previous reports indicated a hot spot present in the area of axillary lymph nodes by PET-CT (4-8). In this case, CT was used to determine severe axillary lymph node swelling mimicking breast cancer metastasis; however, we did not diagnose breast cancer metastasis but rather the influence of the COVID-19 vaccine on the basis of the following: ultrasonography indicated normal lymph node structure including the cortex and medulla; CRP was evaluated on the same day as the enhanced CT was performed (June 2021); and the lymph node size was reduced at the follow-up CT, which is more objective than ultrasonography.
In Israel, a massive vaccination program was started in December 2020, relatively earlier than in other countries. Faermann et al. reported the analysis of 163 cases who presented with ipsilateral lymphadenopathy and history of a recent COVID-19 vaccination in the ipsilateral arm. They showed lymph node cortical thickening was significantly thinner 4-5 weeks after the 2nd vaccination dose (9). This point might be useful for different diagnosis, as in our case. These findings might help us avoid unnecessary biopsies as suggested by Ozutemiz et al. (10). Therefore, we should try to reduce patient anxiety but also avoid further delays in vaccinations and breast cancer screening (11). Furthermore, another study reported cervical or neck lymphadenopathy (12-13), or 18F-FDG PET/CT uptake in a subdiaphragmatic lymph node (14) after vaccination against COVID-19. Currently, the optimal timing for breast cancer surgery and COVID-19 vaccination are still under discussion (15). In the first place, fatality rate of COVID-19 seems to be different from country to country. Greece is the lowest actual number of deaths among European countries with a comparable population (16).
The major limitation of this case report was that only one case was analysed. There might be many cases of breast cancer that lack severe axillary lymph node swelling after COVID-19 vaccination. It is hoped that we can collect data for more cases with a breast tumour or breast cancer, which will allow us to achieve the correct diagnosis.
Conclusion
Vaccination is important for the control of COVID-19 infection. At the same time, clinical oncologists, and especially breast oncologists, should carefully diagnose breast tumours because COVID-19 vaccination could bring on axillary lymph node swelling that is mimicking breast cancer metastasis, as in the case presented herein.
Footnotes
Authors’ Contributions
Research design: Yoshimoto N; collection and analysis of data: Yoshimoto N, Takura K, Yanagi A; all Authors read and approved the final article.
Conflicts of Interest
The Authors report no conflicts of interest.
- Received November 2, 2021.
- Revision received November 20, 2021.
- Accepted December 10, 2021.
- Copyright © 2022, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}
{kind=link}
{kind=link}
{kind=link}