


Abstract
Background/Aim: The effect of β-adrenergic blockers on everolimus-eluting stent (EES) implantation is unknown. We aimed to investigate how β-blockers affect the outcomes of EES by using the Tokyo-MD PCI registry data and analyse real-world data in this drug-eluting stent era in Japan. Patients and Methods: We selected 1,899 patients who underwent EES implantation. We compared patients with β-blocker administration versus those without, at follow-up regarding the incidence rate of ischemia-driven target lesion revascularization (ID-TLR), all-cause death, cardiac death, acute myocardial infarction (AMI), and stent thrombosis (ST). Results: Patients in the β-blocker group had higher coronary risks than those in the non-β-blocker group. Although no significant difference was observed in the five-year incidence of all-cause death, cardiac death, AMI, and ST between the two groups, the incidence of ID-TLR was significantly lower in the β-blocker group (4.5% vs. 6.6%; p=0.04). β-Blocker administration (hazard ratio=0.61; p=0.016) was negatively associated with ID-TLR via multivariate analysis. Conclusion: β-Blocker administration reduced ID-TLR after percutaneous coronary intervention using an EES despite the greater comorbid risks and more severe disease lesions.
- Everolimus-eluting stent
- β-blocker
- interventional cardiology
- target lesion revascularization
- coronary artery lesion
In the history of percutaneous coronary intervention (PCI) with coronary stenting for the treatment of coronary artery disease (CAD), stent restenosis has always been a major problem (1-3). Drug-eluting stents (DES) first emerged in the 2000s with great impact on improving clinical outcomes including a dramatic reduction in stent restenosis rate compared to bare metal stents (BMS) (4, 5). However, delayed healing, which includes delayed re-endothelialization, continuous chronic inflammation, and fibrin deposition, was revealed to be the next problem. The outcomes of DES were improved by changing the polymer and stent design. Everolimus-eluting stents (EES) are one of the most widely used devices worldwide and are generally accepted and favored by Japanese cardiologists with long-term excellent performance within the recent decade (6, 7).
β-Adrenergic blockers (β-blockers) are predominantly used to manage abnormal heart rhythms and to protect the heart from myocardial infarction after an initial heart attack event in what has been termed as “secondary prevention.” They are also widely used for treating hypertension and are recommended as first-line drug for single-drug use in the Japanese guidelines; however, they are not recommended for use in combination with other hypertensive drugs. Therefore, the proportion of β-blockers used in Japan is lower than that of calcium channel blockers (CCBs), angiotensin II receptor blockers (ARBs), and angiotensin-converting enzyme inhibitors (ACEIs).
The Tokyo-MD PCI study was a physician-initiated, multicenter, observational study that was conducted to evaluate real-world data of Japanese patients who underwent EES. Current guidelines for the treatment of CAD recommend daily oral administration of β-blockers as long as there are no contraindications (8-10). β-Blockers were reported to have a secondary effect in reducing the incidence of restenosis after PCI (11), which might be another reason for prescribing β-blockers in this cohort.
Herein, we investigated how β-blockers affected the outcomes of EES using the Tokyo-MD PCI registry data and analyzed real-world data in this DES era in Japan.
Patients and Methods
Study population. The Tokyo-MD PCI study consisted of data from 1,925 patients with 2,330 lesions undergoing EES [XIENCE V (Abbott Vascular, Santa Clara, CA, USA), or Promus stent (Boston Scientific, Natick, MA, USA)] implantation across 22 institutions between January 2010 and December 2011. There were no exclusion criteria for patient selection. Patient demographic and other clinical characteristics were retrospectively collected from hospital charts or clinical databases. Adverse events were searched for up to five years after EES implantation. This study was approved by the institutional ethical review board at Tokyo Medical and Dental University and was conducted according to the Ethical Guidelines for Epidemiological Research. We published all relevant details of this study after obtaining informed consent.
Definition of terms. Current smoking, hypertension, diabetes mellitus, dyslipidemia, chronic kidney disease (CKD) with or without hemodialysis, peripheral artery disease, prior myocardial infarction (MI), prior PCI, prior coronary artery bypass grafting, and family history of CAD were regarded as present when these diagnoses were recorded in hospital charts. Obesity was defined as having a body mass index of ≥25 kg/m2. Acute MI (AMI) was defined as ischemic symptoms, followed by a typical rise in concentrations of troponin above the 99th percentile upper reference limit or as an increase in creatine kinase (CK) or CK-MB to more than double the normal value. Acute coronary syndrome (ACS) included ST-segment elevation MI (STEMI), non-STEMI, and unstable angina pectoris. Cardiogenic shock was defined as having a systolic pressure ≤90 mmHg lasting over 30 min due to cardiac dysfunction in the presence of adequate intravascular volume and left ventricular filling pressure. Left ventricular systolic dysfunction was defined as having a left ventricular ejection fraction (EF) ≤35% on contrast left ventriculography or echocardiography during the hospital stay. All lesion characteristics were diagnosed by physicians within each hospital based on coronary angiograms and imaging devices, such as intravascular ultrasound and optical coherence tomography. Lesion type was defined according to the American College of Cardiology/American Heart Association (ACC/AHA) classification.
All deaths were regarded as cardiac deaths unless unequivocal non-cardiac causes could be identified. Stent thrombosis (ST) was defined according to the Academic Research Consortium definition. Target lesion revascularization (TLR) was defined as revascularization post-stenting within the stent or within the 5-mm borders adjacent to the stent. Ischemia-driven TLR (ID-TLR) was defined as revascularization of the target lesion based on clinical features of ischemia.
Statistical methods. Normally distributed continuous variables were presented as mean±standard deviation (SD) and were compared using the Student’s t-test. Non-normally distributed variables were presented as the median and interquartile range (IQR) and were compared using the Mann-Whitney U-test. Categorical data were presented as percentages. Comparisons of proportions were analyzed using the chi-square test or Fischer’s exact test if the sample size was small. Cumulative incidence of clinical events was estimated by the Kaplan-Meier method, and differences were assessed using the log-rank test. The incidence of ID-TLR was analyzed per lesion. The Cox proportional hazard model was used to assess the covariates with β-blockers for ID-TLR. Univariate analysis was performed for each of the variables listed in Table I and Table II. The frequency of CKD with hemodialysis was excluded because it was included in the CKD frequency. Multivariate analysis was performed for variables with p<0.05. Hazard ratios (HRs) were reported with corresponding 95% confidence intervals. All analyses were performed using JMP® 10.0 (SAS Institute Inc., Cary, NC, USA). All reported p-values were two-sided and p<0.05 was regarded as statistically significant.
Clinical Characteristics of included patients.
Lesion and procedural characteristics.
Results
Baseline characteristics. Among the 1,925 patients who underwent PCI with EES from the Tokyo-MD PCI study, we were able to analyze data from 1,899 patients after excluding patients whose data regarding β-blocker use was missing. By the time of their last follow-up, a total of 918 patients received a β-blocker prescription (β-blocker group, 48.3%) and 981 patients did not (non-β-blocker group, 51.7%). Patients in the β-blocker group had a higher frequency of hypertension, CKD with hemodialysis, ACS, left ventricular systolic dysfunction, prior MI, and multivessel disease. Almost all patients were on aspirin (β-blocker group, 99.7% vs. non-β-blocker group, 99.6%; p=0.771) and thienopyridine (98.4% vs. 9.48%; p=0.996). The percentage of patients on anticoagulant agents, statins, ACEIs, and ARBs was significantly higher in the β-blocker group (Table I).
Lesion and procedural characteristics. A total of 1,133 lesions in the β-blocker group and 1,172 lesions in the non-β-blocker group were analyzed. In the β-blocker group, there was a greater percentage of left main coronary artery lesions, ostial lesions, and ACC/AHA classification type B2/C lesions. Furthermore, in the β-blocker group, the number of stents used, total length of stent, and patients using the 2.5 mm diameter stent was higher than in the non-β-blocker group. In both groups, imaging devices were used at high rates for stent placement (94.5% vs. 93.8%; p=0.439) (Table II).
Clinical outcomes. The median follow-up duration was 1,910 days (IQR=1.222-2.193). There was no significant difference between the two groups regarding five-year cumulative incidence of all-cause death (12.4% vs. 13.5%; p=0.585), cardiac death (4.8% vs. 6.0%; p=0.265), AMI (3.4% vs. 4.0%; p=0.516), and ST (3.1% vs. 3.0%; p=0.897). However, the cumulative incidence of ID-TLR was significantly lower in the β-blocker group (4.6% vs. 6.8%; p=0.047) (Table III and Figure 1). The following variables had significant difference by univariate analysis for the effect on ID-TLR: diabetes mellitus (HR=2.73; p=0.001), CKD (HR=2.94; p=0.001), cardiogenic shock (HR=4.07; p=0.049), left ventricular systemic dysfunction (HR=2.39; p=0.019), peripheral artery disease (HR=2.49; p<0.001), previous PCI (HR=1.46; p=0.049), multivessel disease (HR=1.75; p=0.003), use of β-blocker (HR=0.67; p=0.046), use of statin (HR=0.60; p=0.024), ostial lesion (HR=1.87; p=0.010), restenosis lesion (HR=3.10; p<0.001), and severe calcified lesion (HR=2.07; p=0.001). Multivariate analysis using these variables demonstrated that β-blockers significantly reduced the risk of ID-TLR (HR=0.61; p=0.016) (Table IV).
Clinical outcomes.
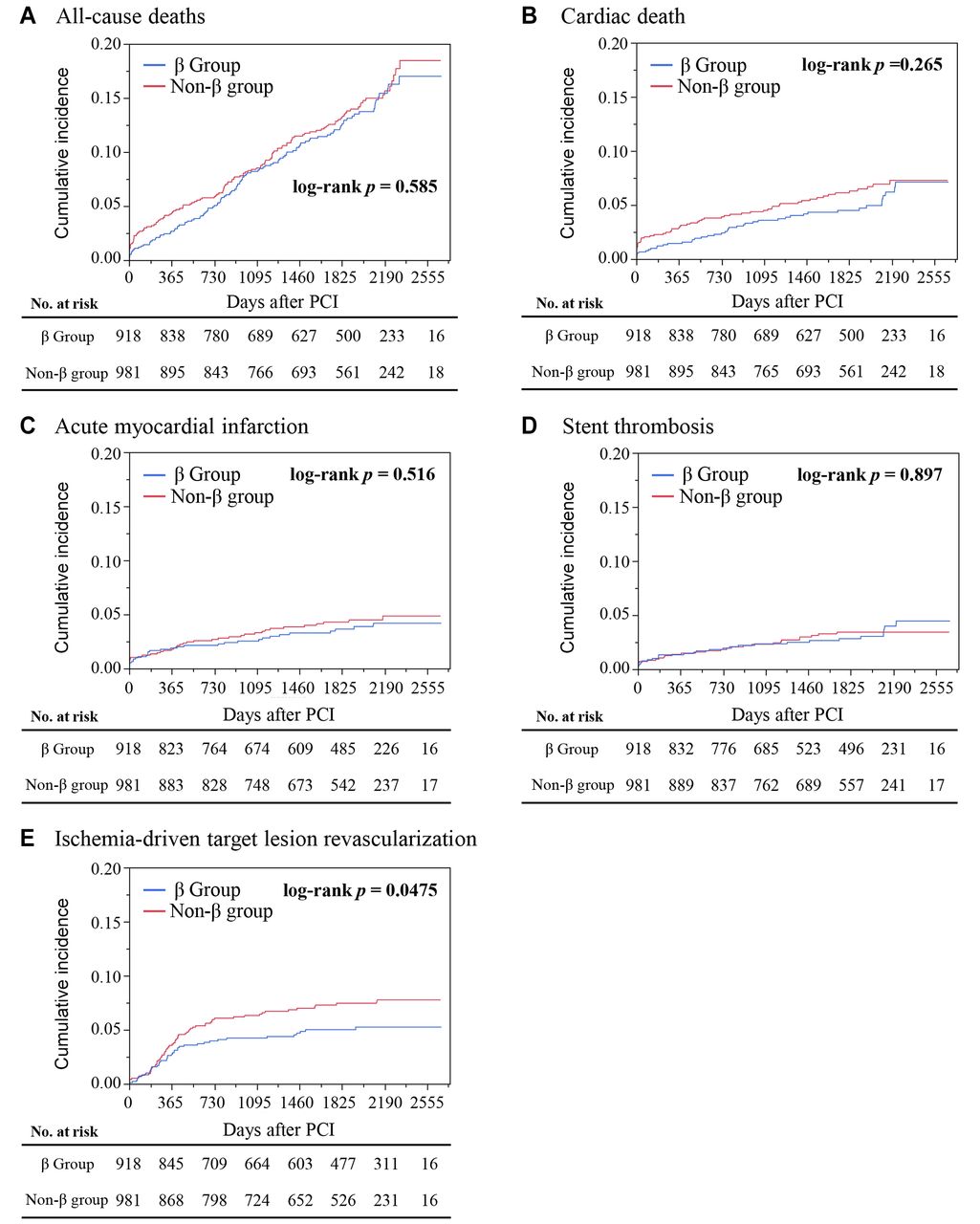
Comparison of (A) all-cause death (B) cardiac death (C) acute myocardial infarction (D) stent thrombosis and (E) ischemia-driven target lesion revascularization between the β-blocker group and the non-β-blocker group.
Multivariate analysis for ID-TLR.
Discussion
In our observational study of patients who had undergone EES, the β-blocker group had more comorbid risks, including hypertension, ACS, history of MI, and multivessel disease compared to the non-β-blocker group; however, medications including statins, anticoagulants, ACEIs, and ARBs were more frequently used. In the β-blocker group, lesions that were difficult to treat (left main coronary artery and ostial lesions) were more frequent, and accordingly, the number and length of stents were greater than those in the non-β-blocker group. Nevertheless, outcomes, including all-cause death, cardiac death, AMI, and ST were comparable to those of the non-β-blocker group and ID-TLR was lower in the β-blocker group. Among the factors associated with ID-TLR via multivariate analysis, a prescription of β-blockers significantly reduced the risk of ID-TLR. These results may prompt the consideration of the administration of β-blockers after PCI in the second-generation DES era.
Previous in vitro studies have shown that β-blockers inhibit vascular smooth muscle cell (VSMC) proliferation and migration, as well as neointimal formation after vessel injury (12, 13). β-Blockers also have an antiplatelet effect that reduces platelet aggregation and deposition on the vessel wall (14-18); however, previous clinical studies from the 1990s had been inconsistent in demonstrating the benefits of β-blockers on restenosis rates. Johansson et al. compared 455 patients treated with β-blockers after percutaneous transluminal coronary angioplasty (PTCA) and 86 patients without β-blockers after PTCA and found no favorable effect on the restenosis rate. However, angiographic success was achieved in 78% of the patients (19). In a prospective, double-blind, randomized, placebo-controlled trial reported in the 2000s, β-blockers were scheduled to be administered pre- and post-successful procedures, which were then compared to placebo groups. Even in this highly technical and well-scheduled cohort study, there was no difference found regarding the restenosis rate between β-blockers (carvedilol) versus placebo in patients undergoing directional coronary atherectomy (DCA) (20). In the 2010s, Jackson et al. showed that β-blockers reduced the six-month TLR in patients who underwent PCI (7.8% in the β-blocker group vs. 10.2% in the without β-blocker group; odds ratio 0.75, p=0.006) (11). The relatively higher TLR compared to our study might be due to the lower frequency of stents (approximately 60%) and the greater variety of procedures studied, such as angioplasty, DCA, and stent implantation in this study. The evolution of endovascular devices may also contribute to the improvement in TLR.
Intimal hyperplasia after stent implantation is caused primarily by VSMC proliferation and is regarded as the main factor for in-stent restenosis (21-23). In the 1990s, restenosis rates after BMS implantation was as high as 20% (1-3). DES, whose stent struts were coated with antiproliferative drugs, theoretically inhibited VSMC proliferation and prevented restenosis. The first-generation DES, sirolimus-eluting stents (SES), drastically reduced the rate of stent restenosis compared to BMS (21, 24). However, restenosis was not completely abolished, and intimal hyperplasia was still thought to cause a high restenosis rate clinically (25). Furthermore, despite the benefits of first-generation DES in reducing the risk of restenosis, two notable problems remain. Poor intimal coverage of stent struts due to too a strong inhibition of VSMC proliferation by long release agents (25) and allergic inflammation against the polymers used in the first-generation DES both caused late stent restenosis (26). The second-generation DES was developed to overcome these problems and EES has successfully reduced the rate of ST and restenosis thanks to improved strut thickness, drug release durations, and biocompatible polymers (5, 6, 27). de la Torre Hernández et al. have reported that the percentage of uncovered struts was only 0.8% at one-year follow-up by optical coherence tomography analyses (28). Furthermore, Otsuka et al., in their autopsy study, reported that significantly fewer uncovered struts were seen in patients with EES implantation compared to those using SES (2.6% in EES vs. 18.0% in SES, p<0.001) and that less inflammation was seen in patients with EES, although 25% of patients with SES and 16% of patients with EES experienced stent-related deaths (29). One of the pleiotropic effects of β-blockers was improving the length of the angina-free exercise period, which might positively influence the outcomes of ID-TLR in our study.
In patients with SES after STEMI, Ozasa et al. reported that β-blockers were not able to reduce the three-year rate of TLR, neither in patients with low EF (β-blocker group 17.7% vs. non-β-blocker group 22.2%, p=0.410) nor in preserved EF patients (12.0% vs. 12.2%, p=0.83) (30). In our study, we set the EF threshold at 35%. There were only 107 patients whose EF was less than 35%. Therefore, we did not perform the subanalysis.
Based on this evidence, we assumed that the additional antiproliferative potential of β-blockers may affect outcomes, including TLR, on the condition that the stenotic lesion was fully intervened using recent technology. EES have thinner struts, more biocompatibility, and shorter drug release duration, all of which may lead to adequate intimal coverage, and thus, allow β-blockers to positively influence the sequence of neointimal formation, resulting in a reduction in ID-TLR in our study.
Recently DES-induced vasospastic angina has focused on as a novel complication, and β-blockers may promote “vasospasm” theoretically. However, the multicenter prospective randomized trial compared the effects of β-blockers and CCBs on coronary events after second-generation DES implantation revealed that the incidence of acetylcholine-induced coronary artery spasms did not differ between these groups at 9 months after PCI. In addition, the incidence of two year major adverse cardiovascular events (MACE) was lower in the β-blocker group (31). Among the factors comprising MACE, only the “coronary revascularization for stable CAD” was statistically significant, which might support our results of beneficial effect of β-blocker on ID-TLR.
Our study had some limitations. First, the Tokyo-MD PCI study was an observational, nonrandomized registry. For the current study, we excluded patients with missing data regarding β-blocker prescription, which amounted to 2% of the patients in the registry. Thus, selection bias may have influenced the results of this study. Second, although the coronary risk of the β-blocker group was higher, the medications including statins, anticoagulants, ACEIs, and ARBs being used by patients in this group benefitted them. Therefore, baseline comorbid risks of the β-blocker group should not be overemphasized. Third, we did not evaluate objective quantitative data from coronary arteriography or coronary imaging, and we used ID-TLR as a surrogate measure of restenosis. ID-TLR is not equivalent to restenosis; however, we assumed that the decision of additional intervention was a more objective and relevant endpoint to assess clinical effects than restenosis. Fourth, we did not study the types and dosages of β-blockers prescribed, mainly because of the multiple combinations possible. The types and doses of β-blockers might affect restenosis; however, the majority of β-blockers used for ischemic heart disease patients in this study were carvedilol and bisoprolol, likely reflecting general beta-blocker usage trends in Japan. Fifth, we analyzed only the patients with EES implantation to eliminate the influence of differences in stent types; therefore, the effect of β-blockers shown in our study cannot be extended to patients using other second-generation DES. Further studies are needed to determine the pharmacological mechanism by which β-blockers reduce ID-TLR after DES implantation.
In conclusion, we found that β-blocker administration reduced ID-TLR after PCI using an EES. Although the β-blocker group had more comorbid risks and more severe disease lesions, ID-TLR was less than that in the non-β-blocker group and the outcomes including mortality and stent coronary events were comparable.
Acknowledgements
We thank the members of the cardiac catheterization laboratories of the participating centers. The list of participating investigators and centers is as follows:
Shigeo Shimizu, Daisuke Ueshima, Ome Municipal General Hospital, Hiroaki Yamaguchi, Okubo Hospital, Kazuo Kobayashi, Toru Miyazaki, Kashiwa Municipal Hospital, Akihiko Matsumura, Kameda Medical Center, Yasuhiro Sato, National Disaster Medical Center, Junichi Nitta, Saitama Red Cross Hospital, Masahiko Furubayashi, Hidenobu Takei, Sanraku Hospital, Tsuyoshi Tokunaga, JA Toride Medical Center, Michio Usui, Social Insurance Chuo General Hospital, Ryo Goto, Shuuwa Medical Hospital, Hiroshi Inagaki, Soka Municipal Hospital, Tsunekazu Kakuta, Tsuchiura Kyodo General Hospital, Go Haraguchi, Yuji Konishi, Tokyo Medical and Dental University, Hiromasa Adachi, Tokyo Kyosai Hospital, Akihiro Hata, Toshima Hospital, Nobuhisa Obuchi, Tokyo Metropolitan Otsuka Hospital, Yuko Onishi, Hiratsuka Kyosai Hospital, Takanobu Miyamoto, Musashino Red Cross Hospital, Hiroyuki Hikita, Shigeki Kimura, Yokosuka Kyosai Hospital, Manabu Kurabayashi, Yokohama City Minato Red Cross Hospital, Hiroyuki Fujii, Yokohama Minami Kyosai Hospital, and Atsuyuki Ono, Otaki Yoichi, Kasai Shoikai Hospital.
Footnotes
Authors’ Contributions
Conceptualization, T.F. and T.A.; methodology, T.A.; validation, K.H. and T.S.; formal analysis, T.A.; investigation, T.S.; data curation, T.S., K.K., S.Y. and H.I.; writing—original draft preparation, T.F.; writing—review and editing, K.H.; visualization, T.F.; supervision, T.S.; project administration, T.S. All Authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
The Authors have no association with industry that could constitute a conflict of interest.
- Received October 13, 2021.
- Revision received November 8, 2021.
- Accepted November 17, 2021.
- Copyright © 2022 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.