


Abstract
Background/Aim: Post-operative radiotherapy for breast cancer can increase cardiac disease in a dose-dependent manner. In this study we show the reduction of dose to heart and left anterior descending artery (LAD) which can be achieved by using “Deep inspiration breath-hold” (DIBH) technique. Patients and Methods: Tangential 3D-planned radiation was delivered to 357 patients with left-sided breast cancer, 159 of them with the DIBH technique. A distinction was made according to fractionation scheme. Results: The mean heart dose was significantly reduced by DIBH from 2.64 Gy to 1.39 Gy (p<0.001). The mean dose to the LAD was significantly reduced from 5.68 Gy to 3.88 Gy (p<0.001). Mean dose and volume receiving 5, 10 and 15 Gy of ipsilateral lung were higher with both hypofractionated schedule and conventional fractionation in the DIBH group. Conclusion: DIBH in left-sided breast irradiation is an effective method of reducing the radiogenic heart dose.
One of the most common malignant tumours in women is breast cancer (1). After surgical therapy, postoperative radiotherapy reduces the risk of local recurrence and is therefore an obligatory part of breast conserving therapy. While long-term survival has been shown to be improved (2), long-term cardiac toxicity of different therapeutic approaches requires greater attention.
In left-sided breast cancer, adjuvant radiotherapy may be associated with an increased risk of cardiac injury (3). Conventional tangential treatment technique may influence potential cardiac risk when parts of the heart and in particular the left anterior descending artery (LAD) are located within the treatment field. Any reduction in radiation exposure to the heart may lower the risk of ischemic heart disease. One simple and readily available method to reduce the dose to the heart is the deep inspiration breath-hold technique (4).
The objective of this analysis was to evaluate treatment planning and compare dosimetry plans in free breathing; non-deep inspiration breath-hold (nDIBH) and deep inspiration breath-hold (DIBH), with the aim to validate the findings of Darby in 2013 (3) within our own cohort of patients based on individual CT-based three-dimensional treatment planning. In order to define acceptable doses for the heart and LAD, it is necessary to evaluate potential dosimetric benefits of DIBH while maintaining acceptable lung toxicity.
This will be achieved, in this retrospective study, using comparison of quantitatively dose-volume exposure of the heart and LAD as well as the ipsilateral lung. This study included patients with left-sided breast cancer receiving postoperative radiotherapy with 3D-planned tangential fields at our Department using either DIBH or nDIBH. The key issue is whether the systematic application of DIBH could consistently reduce radiation exposure of the heart and LAD below the postulated dose limits by Darby (3) and whether this also applies to modern hypofractionated radiation schedules. Consequently, two different time periods, before and after the publication of Darby in 2013 (3) were compared, resulting in more awareness of avoiding radiation exposure to the heart and subsequent use of the DIBH technique in left-sided breast cancer patients.
Patients and Methods
Patient characteristics, radiation treatment plans and information on cardiac risk factors were collected retrospectively from databases of the department of radiation oncology of the Hannover Medical School. The conduct of the study was reviewed and approved by the local ethics committee.
In total, 357 ongoing patients with left-sided breast cancer were included in the study; of which 159 were irradiated using DIBH technique. Inclusion criteria for this study was 3D-planned tangential radiotherapy (3D-CRT) in case of curative breast conserving therapy (n=302; 168 in the nDIBH group and 134 in the DIBH group) or mastectomy (n=55; 30 in the nDIBH group; 25 in the DIBH group), respectively. The ipsilateral periclavicular lymph nodes without internal mammary nodes were irradiated in 76 patients (45 in the nDIBH group and 31 in the DIBH group). All patients were irradiated postoperatively in supine position. Patients receiving partial breast irradiation or re-irradiation were excluded from the study.
Patients with left-sided breast cancer were grouped according to their respective time period of radiation treatment. First group included a total of 198 patients irradiated without DIBH (nDIBH) between 01/2011 and 06/2013, second group included a total of 159 patients irradiated with DIBH between 01/2017 and 12/2019 after consequent clinical implementation of DIBH technique. Within the same period a transition took place from conventional fractionation (CF) to more routinely application of hypofractionated radiotherapy schedules (HF) according to changes of clinical practice guidelines. Baseline clinical and treatment related parameters of patients in both groups (nDIBH and DIBH) are listed in Table I.
Patient baseline characteristics of the study cohort (n=357).
All patients received a noncontrast enhanced free-breathing planning computed tomography (CT) scan in supine position with 3 mm axial slice thickness. Postoperative surgical scars were marked with radiopaque material. From 2017 onwards all patients with left-sided breast cancer with close positional relationship of the heart to the chest wall received a second planning CT scan with DIBH during the same appointment. Decision to use DIBH was based on a visually expected benefit compared to free breathing. Main criterion for choosing DIBH technique was whether the medial aspects of the anticipated tangential radiation field borders would cross the heart in free breathing planning CT.
A simple breath-hold technique (non-computer controlled) was used during radiotherapy. After initial patient coaching amplitude of breath-hold was monitored by visual control via camera outside by medical staff (audio-visual guidance). For consistency and to reduce inter observer variability the heart, LAD and lungs were retrospectively delineated on planning CT by the same physician (Anne Caroline Knöchelmann). The heart as well as the LAD was delineated according to the CT-based atlas by Feng (5). The cranial border of the heart was contoured beginning underneath the pulmonary trunk, ascending aorta and superior vena cava. The lower border of the heart was the caudal myocardial border near the diaphragm. All fatty tissue within the pericardium was contoured because of the presence of cardiac vessels. The LAD was contoured from the left coronary artery underneath the right pulmonary vessel running between right and left ventricle to cardiac apex. Therefore, on some images the LAD was not visible in noncontrast enhanced CT scan. The location of the LAD was then inferred using visible landmarks. Contouring of the left lung was carried out excluding the bronchial tubes.
Clinical target volume (CTV) was delineated according to Radiation Therapy Oncology Group breast cancer atlas (6). The CTV included all ipsilateral breast tissue except muscles below and adjacent skin. In case of chest wall irradiation, the posterior border of the CTV ended at the anterior pleural surface including the ribs and intercostal muscles. The margin for the planning target volume (PTV) was 5-10 mm taking into account adjustments on the medial and lateral as well as inferior and superior borders. A sequential radiation boost was applied in patients younger than 50 years or presence of risk factors (e.g., poor grading). The boost volume was delineated on the basis of available pre-operative imaging supported by radiopaque marking of surgical scars.
All patients were treated with 3D-CRT by tangential fields using a linear accelerator with individual multileaf collimation. Tangential irradiation beams, with segmental fields for dose homogenization if necessary, were used for breast or chest wall treatment with 6 MV photons and if necessary 15 MV photons for partial fields in selected cases.
Quantitative dose-volume parameters of heart, LAD and ipsilateral lung were extracted from the treatment planning system (Oncentra® by Elekta, V4.3). To analyse differences between the dose-volume parameters in the nDIBH and DIBH group, statistical analyses were performed. The following parameters were derived from the dose-volume histogram of each treatment plan: absolute volume of contoured heart, the mean heart dose (MHD) as well as partial volume parameters of the heart receiving 5 Gy (V5), 10 Gy (V10) and 25 Gy (V25); For LAD we sampled the absolute volume of LAD as well as maximum dose (LAD Dmax) and mean dose (LAD Dmean); for the lung the volume of the ipsilateral lung was sampled, mean dose of ipsilateral lung (MLD) and relative volume of the ipsilateral lung receiving 5 Gy (V5), 10 Gy (V10), 15 Gy (V15) and 20 Gy (V20). Details are displayed in Table II and Table III.
Volumes of organs at risk (volume in cm3).
Dosimetric parameters of heart, LAD and ipsilateral lung.
All data were tested for normal distribution using the Kolmogorov Smirnov test (α=0.05). Variables with normal distribution were analysed using unpaired t-test. Variables without normal distribution were analysed using Mann-Whitney U-test. Values of p<0.05 were considered to be statistically significant. Correlations between different parameters were determined using linear regression and quantified as Pearson´s correlation coefficient. SPSS Statistics 28 was used for the statistical analysis.
Results
Main findings regarding comparative dose exposure of heart, LAD and left lung are described below. Detailed results are shown in Table II, Table III and Table IV. For the complete cohort of patients mean heart volume was 502±135 cm3 (range=195-1,099 cm3) and mean volume of LAD was 2.93±0.89 cm3 (range=0.76-6.02 cm3). Mean lung volume was 1,614±573 cm3 (range=630-3,435 cm3) (Table II).
Dosimetric parameters of heart, LAD and ipsilateral lung depending on fractionation regimen (Conventional fractionation and hypofractionated schedule).
In the nDIBH group the MHD was 2.64±1.26 Gy and in the DIBH group the MHD was 1.39±0.47 Gy (Table III). Taking into account the fractionation scheme, in patients with conventional fractionation (CF), MHD in the nDIBH group was 2.84±1.32 Gy and in the DIBH group 1.81±0.52 Gy. In patients with hypofractionated schedule (HF), the MHD in the nDIBH group was 2.03±0.81 Gy and in the DIBH group 1.31±0.42 Gy (Table IV).
Using DIBH resulted in a significant reduction in MHD in both CF (reduction of 1.03 Gy; p<0.001) and HF (reduction of 0.72 Gy; p<0.001) using DIBH (Table IV; Figure 1). In the nDIBH group, 42 patients (21%) received a MHD greater than 3.0 Gy and 9 patients (5%) received more than 5.0 Gy. By contrast, in the DIBH group only 2 patients (1%) received a MHD greater than 3.0 Gy. Both latter patients received postmastectomy irradiation, one of them with CF and the other with HF. Besides the reduction of MHD, the volumes of the heart receiving 5 Gy and 10 Gy (V5 and V10) were significantly reduced by DIBH (p≤0.001), while V25 was significantly reduced in patients with HF only (Table IV).

Mean heart dose (MHD) in DIBH compared to nDIBH. Gy: Gray; CF: conventional fractionation; HF: hypofractionated schedule; nDIBH: non-deep inspiration breath-hold; DIBH: deep inspiration breath-hold.
In the nDIBH group the LAD Dmean was 5.68±5.24 Gy and in the DIBH group it was 3.88±2.59 Gy (Table III). In the CF/nDIBH group, LAD Dmean was 6.30±5.73 Gy and in the CF/DIBH group 4.41±2.04 Gy. In the HF/nDIBH group, LAD Dmean was 3.75±2.45 Gy and in the HF/DIBH group 3.79±2.67 Gy (Table IV).
In the nDIBH group the LAD Dmax was 12.43±12.18 Gy and in the DIBH group the LAD Dmax was 11.05±9.18 Gy (Table III). In the CF/nDIBH group, LAD Dmax was 13.59±12.96 Gy and in the CF/DIBH group 13.43±10.31 Gy. In the HF/nDIBH group, LAD Dmax was 8.82±8.47 Gy and in the HF/DIBH group 10.63±8.94 Gy (Table IV).
A positive linear correlation was found between LAD Dmean and MHD in all subgroups (Figure 2). In nDIBH, the linear gradient between the LAD Dmean and MHD was 3.2 in CF and 2.3 in HF, respectively. In DIBH, the linear gradient between the LAD Dmean and MHD was 2.5 in CF and 4.8 in HF. A high positive correlation (Pearson’s correlation coefficient r>0.7) was found except in the subgroup CF/DIBH. Altogether, eight patients with a MHD below 3.0 Gy exhibited a LAD Dmean>10.0 Gy: four patients in subgroup HF/DIBH and four patients in subgroup CF/nDIBH.
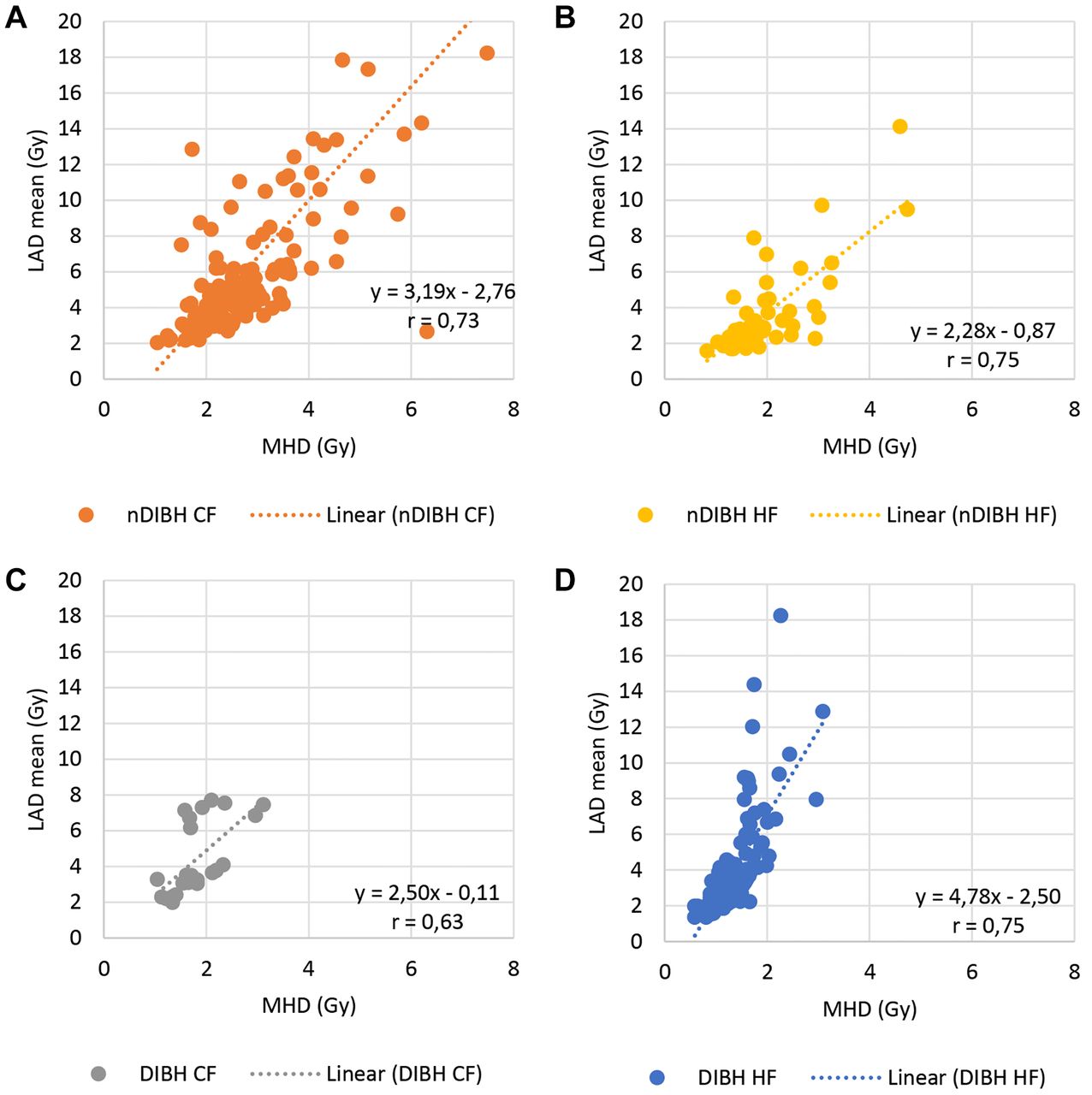
Correlation between LAD Dmean and MHD. (A) and (C) conventional fractionation without and with DIBH; (B) and (D) hypofractionation schedule without and with DIBH. LAD: Left anterior descending artery; MHD: mean heart dose; CF: conventional fractionation; HF: hypofractionated schedule; nDIBH: non-deep inspiration breath-hold; DIBH: deep inspiration breath-hold.
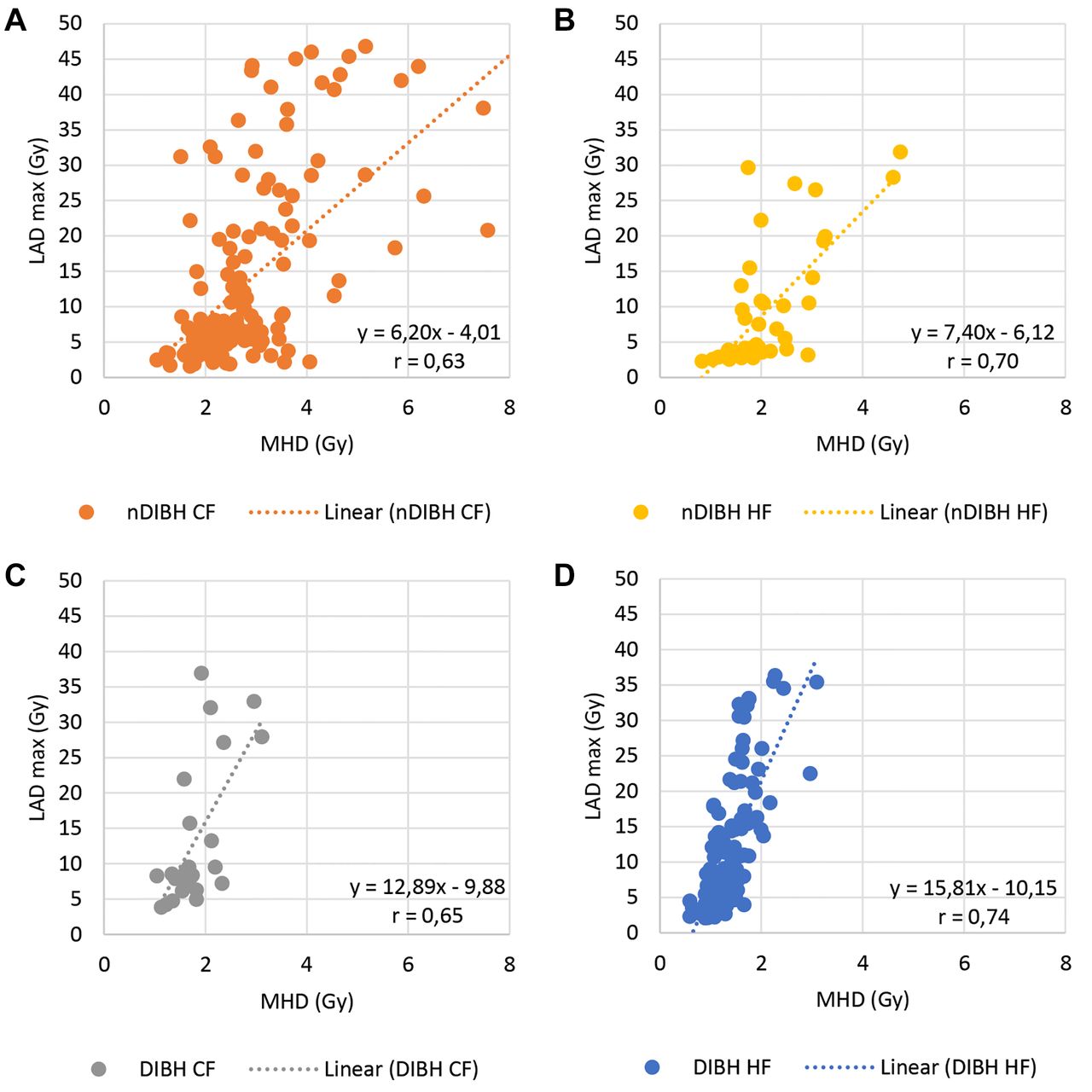
Our data showed a moderate linear correlation between LAD Dmax and MHD in the nDIBH group as well as in the DIBH group (Figure 3). In the nDIBH group, the linear gradient between LAD Dmax and MHD was 6.2 in CF and 7.4 in HF, respectively. In the DIBH group, the linear gradient between LAD Dmax and MHD was 12.9 in CF and 15.8 in HF. In HF this resulted in a high positive correlation (r>0.7 in both DIBH and nDIBH) whereas in CF this correlation was moderately only (r=0.65 in DIBH and r=0.63 in nDIBH).
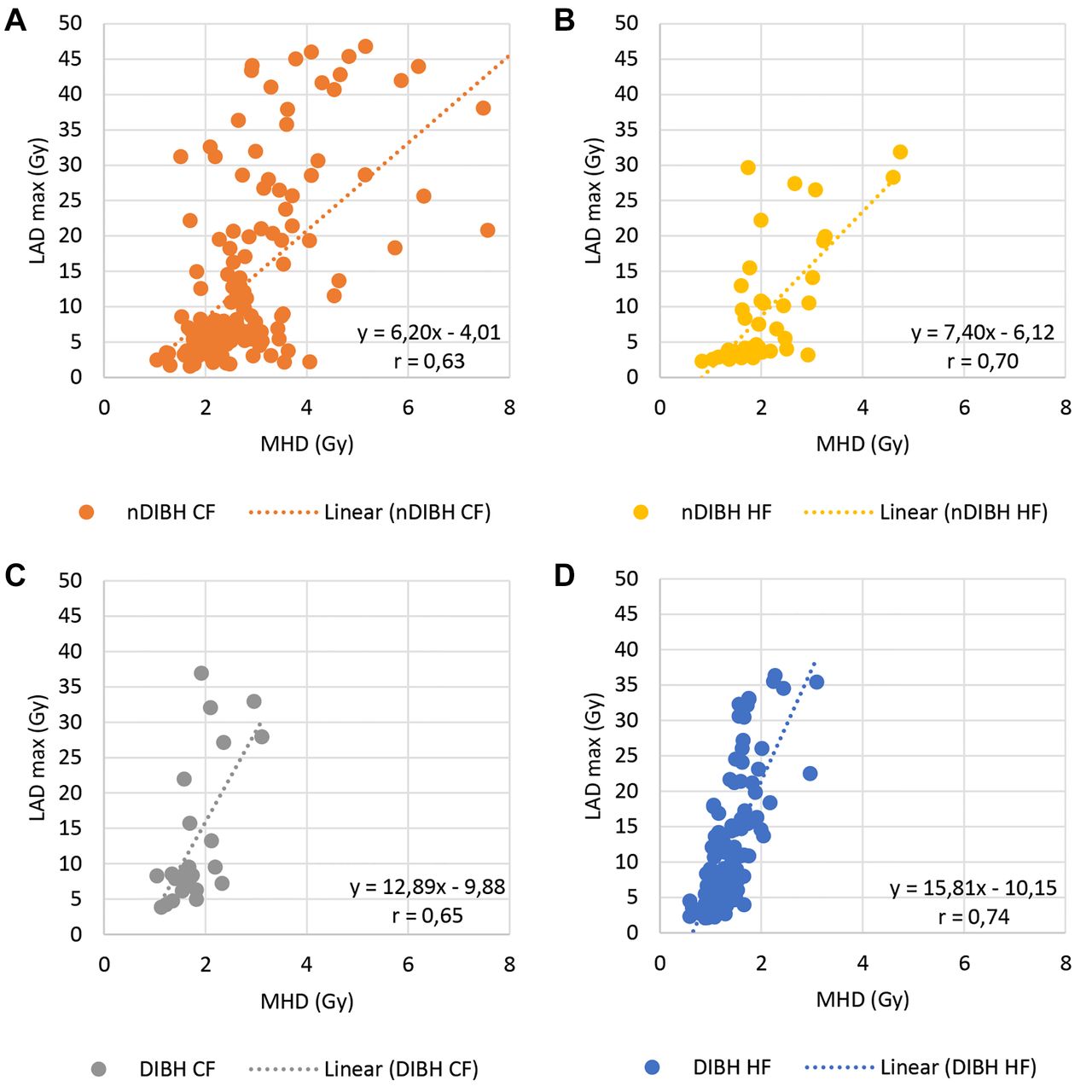
Correlation between LAD Dmax and MHD. (A) and (C) conventional fractionation without and with DIBH; (B) and (D) hypofractionation schedule without and with DIBH. Gy: Gray; LAD: left anterior descending artery; MHD: mean heart dose; CF: conventional fractionation; HF: hypofractionated schedule; nDIBH: non-deep inspiration breath-hold; DIBH: deep inspiration breath-hold.
Mean dose of the ipsilateral lung (MLD) was significantly higher in DIBH compared to nDIBH in both CF (DIBH 8.53±2.24 Gy vs. nDIBH 7.03±2.94 Gy; p=0.007) as well as HF (DIBH 5.46±1.90 Gy vs. nDIBH 4.80±1.50 Gy; p=0.017) (Table IV). Similarly, ipsilateral lung volumes receiving at least 5 Gy, 10 Gy and 15 Gy (V5, V10, V15) were significantly higher in DIBH compared to nDIBH in both fractionation schemes (p<0.05).
Discussion
Radiation exposure of the heart is a risk factor for the occurrence of coronary disease in oncological therapy. A recent analysis of a large data set from the Surveillance, Epidemiology, and End Results database (SEER) revealed an increased relative mortality in patients with left-sided breast cancer who received radiation before 1990 (7), especially in younger women and when chemotherapy was also given. After 1990 several studies showed no evidence of increased cardiac mortality for left-sided radiotherapy (8). However, there is still no proven relationship between the cardiac dose and the risk of cardiac mortality after several years of latency with an increase in relative risk of 4.1% per Gy mean cardiac dose (9). Pre-existing heart disease might increase the risk of acute cardiac events in a curative setting of oncologic treatment. In some cases, cardiac comorbidities may not be known at the time of treatment. Further systemic therapy (anthracyclines, taxanes, trastuzumab) increases the probability of cardiotoxicity (7). In these cases, it is essential to select patients, who could receive a significant dose to critical structures of the heart, namely the LAD, and then to offer them cardiac sparing radiotherapy with e.g., DIBH to avoid any additional increase in cardiac risk exposure.
Darby (3) found MHD being a predictor of major coronary events. This frequently cited study suggests that the risk of cardiac events is proportional to MHD with a relative increase of 7.4% per Gy of mean heart dose in the rate of major acute coronary events starting within the first five years after radiotherapy with no threshold. Considering this, our data showed that almost all patients (99%) with DIBH had a mean MHD below 3.0 Gy and even 74% patients with free breathing (nDIBH) had a mean MHD below 3.0 Gy. This already shows excellent heart protection in our cohort even before the publication of Darby (3). However, we found a significant further reduction of mean MHD from 2.64 Gray (Gy) in patients irradiated without DIBH compared to 1.39 Gy with DIBH (47% relative reduction).
In a review by Drost et al. (10) the cardiac dose is described in case of whole breast irradiation except brachytherapy or proton radiotherapy between January 2014 and September 2017. On average, they could find that the MHD decreased between 2014 (4.6 Gy) and 2017 (2.6 Gy). Regimens with breathing control had a lower MHD (1.7 Gy) compared to regimens without breathing control (4.5 Gy). This is in line with our results as described above. A significant dose reduction due to breath-hold technique could be found in several studies with conventional fractionation regimens for MHD (11-13) as well as LAD (14, 15).
When interpreting data from different treatment periods, it should be taken into account that nowadays almost exclusively hypofractionated treatment schedules are used. Our data showed a significant dose reduction in MHD in both conventional fractionation and hypofractionated schedules. Therefore, the existing dose recommendations for the heart need to be reconsidered in the era of hypofractionated schedules due to the radiobiological effect of fraction size. To correct dose distributions of hypofractionation treatment plans to equivalent dose in 2 Gy fractions, the linear quadratic model is used. This results in a lower biologically equivalent cardiac dose in HF compared to CF (16, 17).
Furthermore, to date no increased cardiac mortality has been observed in the current studies on hypofractionation (18). Heart and LAD are located in the low dose range of the irradiation fields. While the heart is a complex organ at risk and α/β value should be used with caution (19), we need more long-term follow-up data in hypofractionated breast radiotherapy to adapt existing cardiac dose constraints especially in case of ultra-hypofractionated schedules.
This study found no significant reduction in LAD Dmean by using DIBH. This might lead to the assumption, that DIBH technique may not necessarily lead to further reduction in the dose to the LAD. However, we observed a correlation of LAD Dmean with MHD in all subgroups with a linear correlation coefficient r>0.6. Per 1.0 Gy in MHD the LAD Dmean increased by at least 2.0 Gy. This correlation was also described by Evans (20). Their data showed an increase in LAD Dmean by 4.82 Gy per 1.0 Gy in MHD. The authors concluded that the LAD may not need to be contoured separately when conventional tangential treatment technique is used. Having in mind that our collective of patients included some patients with high LAD Dmean and LAD Dmax despite low MHD, in our opinion it is not enough to contour the heart only as an organ at risk. Regarding the literature, it remains unclear, whether LAD Dmean is of relevance with respect to radiogenic cardiac events (21, 22). Based on this fact and on our findings, LAD should be additionally delineated as an organ at risk.
Furthermore, using MHD as the most important predictor for late cardiac toxicity disregards the fact that dose distribution within the heart is not homogenous. High radiation dose exposures can be observed in the apex of the heart as well as in the apical-interior segment, where the LAD originates (23, 24). In another study, an increase of stenosis in the LAD in hotspot areas resulting in an increased risk of coronary artery stenosis in the LAD was shown (25). This leads to the assumption that LAD Dmax may equally play an important role in the development of late cardiac events. Our data show a correlation between MHD and LAD Dmax in all subgroups. An increase of more than 6.0 Gy in LAD Dmax per Gy MHD in all subgroups was seen. To avoid additional risk of adverse cardiac events, the hotspot areas to the LAD represented by LAD Dmax, should be kept as low as possible, accordingly.
Despite breath-hold technique, there is an intrinsic cardiac motion that should be considered in radiation planning. Wang (26) found that the major displacement of the heart occurring in the posterior area, which is unlikely to affect the heart dose received from tangential radiation. Displacement of the LAD was shown in 10% of the patients with at least 30% volume shift. This underlines the importance of protecting the LAD even when DIBH is used.
Due to the small volume of contoured LAD an underestimation of dose actually received to LAD may occur. There are several contouring atlases suggesting slightly different cardiac delineation. This results in a large variability in contouring heart and LAD. Lorenzen (27) showed large inter-observer variation in delineation of the LAD even using contouring guidelines. To enhance consistent delineation of organs at risk, in our study delineation of organs at risk (heart, LAD, lung) was performed by the same physician. This is in accordance to Feng (5) as well as other studies (4, 28-30). Nevertheless, our data show a large variance in volume of the LAD with an overall small volume of contoured LAD independent of the DIBH technique (nDIBH: 2.95±1.01 cm3, DIBH: 2.9±0.71 cm3). Additionally, the slice thickness of our planning CT-scans (3 mm) might have resulted in uncertainty in LAD delineation. Some authors (31) generated an additional planning structure around the LAD with a width of 5 mm anterior-posterior and 10 mm left-right around the LAD considering the uncertainties of contouring. They concluded that even rough contouring is sufficient to assess the dose of the LAD but with the recommendation to carefully contour the specific cardiac substructures such as LAD, while Dmean of the heart is not specific enough.
Dose distribution is also influenced by the radiation technique. Some studies show a dose reduction in heart and LAD using intensity modulated radiotherapy (IMRT) plans (32, 33). In elderly breast cancer patients, there was shown a significant dose reduction in LAD Dmean and LAD Dmax without a significant difference in heart sparing (34). Despite a low MHD achievable in IMRT plans there is still a risk of hot spots within the LAD making additional contouring of LAD mandatory for IMRT plan optimization (35). Mast (29) demonstrated that the reduction in LAD Dmean using DIBH was marginally greater in 3D-CRT compared with IMRT.
Overall, there is a small difference between 3D-CRT and IMRT in terms of reducing MHD and LAD Dmean using DIBH. In the era of IMRT and volumetric arc therapy (VMAT) techniques, it is justified to use conventional tangential treatment technique because the modern techniques take longer in applying irradiation and the patients need to hold their breath for a longer time. In some selected cases it might be well founded to use IMRT or VMAT technique to lower the dose to the heart as well to the LAD. Using IMRT or VMAT, it should be kept in mind that there can potentially be an increased risk of secondary cancers due to change of dose distribution and increase in monitor units (36). According to national treatment guidelines (37), radiation with tangential fields is still considered standard of care and IMRT techniques should be limited to patients with special conditions like larger breast volume or deviating anatomy of breast or thoracic curvature.
Apart from the heart, the lungs are also irradiated during tangential chest irradiation possibly leading to development of pulmonary fibrosis and lung function decline. In our analysis, the lung volume was significantly larger in patients with DIBH compared to those without DIBH (2,102±424 cm3 respectively 1,223±323 cm3) due to the anatomical position changes during deep inspiration. The mean lung dose (MLD) was also significantly higher in DIBH in both HF (5.46±1.90 Gy in DIBH and 4.8±1.50 in nDIBH) and CF (8.53±2.24 Gy in DIBH and 7.03±2.94 Gy in nDIBH). In the HF group, however, the MLD was lower overall compared to the CF group.
Chan (11) summarizes in a review article several studies concerning this topic. The literature contains contradicting results regarding the resulting lung doses when using DIBH. Quantitative dose-volume analyses do not take into account different density of the lung between inspiration and expiration. With increasing lung volume in deep inspiration, the lung density may decrease, resulting in irradiation of a reduced fraction of normal lung mass (37). To avoid mistakes in interpretation of dose-volume constraints to the lung, Oechsner (41) suggests the dose-mass histogram (DMH) as a more accurate model to measure relevant dose to the lung. In that study, the mean lung density was decreased by using DIBH technique compared to free breathing. This is in contrast to the results of our analysis, which showed an increased MLD of the lung using DIBH in both HF and CF. Possibly, there might be differences between techniques of breathing maneuvers. In 2018, Zhao (42) presented a prospective analysis showing the abdominal breathing maneuver as the most lung and cardiac sparing technique compared to thoracic breathing. To generate comparable data, there should be consistent requirements of the breathing maneuver. Finally, it is not clearly understood in the current literature whether the lung dose and therefore the risk of radiation-induced pneumonitis is increased using DIBH. Furthermore, as the purpose for DIBH treatment is to avoid heart dose, it is also important to point out that DIBH may result in increased pulmonary exposure, which may lead to corresponding pulmonary toxicity.
Our results regarding dose distribution of the heart are in line with Ferini (43) showing a significant dose reduction of MHD as well as LAD Dmean in DIBH technique compared to nDIBH. The distance between the tangent fields in case of 3D-CRT is the most important influencing factor for dose distribution to the heart. It can be used as an indicator for the actual benefit in terms of heart protection. The authors conclude that with the help of this anatomical predictor, the decision to perform irradiation in DIBH can be facilitated and objectified.
The presented study was performed retrospectively. Known limitations of retrospective studies include the quality of available data, which in our case were collected up to 10 years ago. To eliminate the differences regarding the contouring risk organs heart and lung, all planning data were re-contoured by the same physician. This results in comparable data from the two periods analyzed.
Another disadvantage of retrospective studies is bias due to confounding variables. Patients of this study were clustered in two groups that represent different periods. In the first period (2011-2013), irradiation in CF was state of the art and mainly used. Subsequent evolvement of irradiation technique led to changes in the second period (2017-2019) where more often HF was used. Considering this confounding variable our analyses was done in subgroups comparing DIBH/HF with nDIBH/HF and DIBH/CF with nDIBH/CF.
Besides the retrospective nature, the limitation of this study is the inter-individual comparison of dose-volume parameters irradiated in two different treatment periods. In contrast, other authors did intra-individual dosimetric comparison of treatment plans but equally found a significant decrease of cardiac dose (13, 37-40). Compared to other publications regarding DIBH in our study is included a large number of patients, which we see as an advantage.
In conclusion, DIBH could significantly reduce the MHD in conventional fractionated and hypofractionated scheduled radiotherapy. DIBH is a simple and reproducible technique and is readily applicable in routine clinical practice. However, it does not seem sufficient to focus attention merely on MHD, because hotspots may occur at LAD even though MHD is low. Consistent data with comparable groups of patients and breathing maneuvers should be sampled to generate standardized dose constraints, taking into account the individual patient characteristics such as age, compliance and co-morbidities as well as fractionation schedule and modern irradiation techniques such as IMRT. There is a need to define valid criteria to select patients who benefit most from DIBH in terms of mean heart dose.
Footnotes
Authors’ Contributions
Anne Caroline Knöchelmann collected the data, analysed them statistically, put the results into the current context and wrote the article. Nese Ceylan researched part of the patients who were eligible for the study. Michael Bremer revised it critically for important intellectual content. All Authors read and approved the final version.
Conflicts of Interest
The Authors declare no conflicts of interest in association with the present study.
- Received August 27, 2021.
- Revision received September 10, 2021.
- Accepted October 11, 2021.
- Copyright © 2022 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}
{kind=link}
{kind=link}