


Abstract
Background/Aim: Cervical cancer is the second most common malignancy among women in Vietnam, but the country is yet to introduce a national human papillomavirus (HPV) vaccine programme targeted at adolescents. We determined HPV prevalence and HPV vaccine knowledge among female university students in Vietnam. Patients and Methods: We surveyed and screened 1,491 female university students in Hanoi, Hue, and Ho Chi Minh City for their sexual behaviours, HPV knowledge and low- and high-risk HPV infection. Results: The prevalence of any HPV infection and any high-risk HPV infection were 4.2% (95%CI=3.3%-5.4%) and 3.4% (95%CI=2.5%-4.4%), respectively. Being sexually active [adjusted prevalence ratio (aPR): 6.22; 95%CI=3.4-11.37] and having ever been pregnant (aPR: 4.82; 95%CI=1.93-12.04) were positively associated with high-risk HPV infection. Whilst 60% of participants had heard of HPV vaccine, only 4.6% had received the vaccine. Conclusion: The low HPV prevalence found in university students in Vietnam indicates that they can benefit from HPV vaccination, along with a well-designed HPV health promotion programme.
Human papillomavirus (HPV) is one of the most common sexually transmitted infections around the world (1). It is the cause of several types of anogenital cancers and oropharyngeal cancer, of which the most common is cervical cancer. The majority of HPV infections (80%) are asymptomatic and resolve spontaneously. For those women with persistent infections with high-risk (hr) or oncogenic HPV genotypes, a proportion may later develop cervical abnormalities of high-grade cervical dysplasias which are precursors to cancer (2-5).
To date, three licensed prophylactic HPV vaccines are available, all of which target HPV16 and 18 which are responsible for approximately 70% of cervical cancer cases globally. The nonavalent HPV vaccine also protects against an additional five common cancer-causing HPV types (HPV31, 33, 45, 52 and 58) responsible for another 20% of cervical cancer cases worldwide (6). The World Health Organization (WHO) recommends that all countries vaccinate at least 90% of females aged 9-14 years against HPV. This is a key component of the 2030 goal of 90%, 70% and 90% for vaccination, screening and treatment respectively to establish the basis for the global elimination of cervical cancer as a public health matter (7-11). Although cervical screening with high precision tests at 35 and 45 years of age has been successful in detecting hrHPV types predicting underlying cancer precursors, such secondary prevention has several challenges, including difficulties in implementing these procedures at high coverage levels in many low- and middle-income countries (LMICs) where appropriate infrastructure may be lacking (7, 12).
Cervical cancer is the second most common malignancy among women in Vietnam (13, 14). However, the country has not yet introduced a national HPV vaccination programme, even though HPV vaccination of young adolescent females has been shown to be cost-effective in Vietnam (15). Young women who have recently become sexually active are at high risk of acquiring HPV infection (16). Low HPV vaccination rates among young girls (9-18 years old) predisposes them to HPV infection as they reach sexual maturity (4, 11, 17, 18). In this cross-sectional study, we measured the HPV infection rates and the risk factors for HPV infection, as well as HPV disease and HPV vaccination knowledge among female university students from three universities in Hanoi, Hue and Ho Chi Minh City (HCMC), Vietnam.
Patients and Methods
Participants. Cross-sectional surveys of HPV genoprevalence, risk factors and knowledge among university students were conducted from November 2017 to March 2019 in three major Vietnamese cities: Hanoi in northern Vietnam, Hue in central Vietnam, and HCMC in southern Vietnam. Most undergraduate students in Vietnam take 4-5-year degree courses with the university calendar starting in September and ending in June of the following year. The majority of students start university at 18 years of age. Participants in this study were first- and fourth-year university students from selected universities in Hanoi, Hue and HCMC. Recruitment began in Hanoi (November 2017), continued in Hue (December 2017), and ended in HCMC (December 2018–March 2019). Students from all departments in the universities were recruited; the departments were then categorized into social and natural science. Although universities in Hanoi and Hue have both departments, the university in HCMC only has the department of natural science. Participants were recruited via social media platforms such as Facebook, Zalo and Instagram, as well as through the student union. Participants were recruited on a first-come-first-serve basis while ensuring the number of students from the first year and fourth year were roughly equal. A total of 1,500 female students were determined eligible and provided consent to participate in this study. Based on an estimated HPV prevalence of 4-20% among girls aged 18-24 years in Vietnam, a total of 245 participants/group/site is needed to achieve 80% power. Thus, we aimed to recruit 500 participants from year 1 and year 4 from each university.
Outcome assessments. In a private room at each university, students received instructions by trained medical staff on self-collection of vaginal samples for HPV screening. After sampling, the students were invited to complete a questionnaire lasting approximately 20 min. A trained interviewer asked the participants basic questions about their demographic attributes, sexual behaviours, HPV vaccination status, medical history and knowledge of HPV and its prevention. Participants were given the option to complete questions on their sexual behaviour by themselves. Any participants found to be positive for HPV16/18 were referred to further gynaecological examination and management.
HPV detection and genotyping test. HPV detection and genotyping were performed in two steps. Firstly, nucleic acid extraction was performed using Cador pathogen 96 Qiacube HT kit (Qiagen, Hilden, Germany) on an automated platform, followed by amplification with PGMY9/11 system by polymerase chain reaction (PCR) (19). Next, the positive samples by PCR were subjected to genotyping by Geneflow HPV array test kit (Diagcor, Hong Kong), which allows detection and identification of 33 HPV types [14 high-risk (hr), three probable high-risk and 16 low-risk types]. The kit was in-vitro diagnostic and qualified annually by WHO for hrHPV detection and classification.
The human leukocyte antigen (HLA) and beta-globulin genes were used as internal controls for the PGMY9/11 PCR and Geneflow kit, respectively. The HLA primer pair are directed against the common site of all HLA types. Samples that were negative for the HLA gene were considered invalid, and the participants were asked to return for a new sample collection. Method validation was done on a panel of 40 previously tested samples prior to the screening test. External quality control was also performed by the Western Pacific WHO reference laboratory for HPV at the Royal Women’s Hospital, University of Melbourne, Australia. We found ~90% agreement for hrHPV between laboratories for all samples; some discordant/missed results were found for certain tested hrHPV genotypes: 4/20 for HPV16, 1/12 for HPV18, 1/4 for HPV31, 2/12 for HPV39, 2/7 for HPV45, 3/9 for HPV56, 2/17 for HPV58, 3/16 for HPV 66.
Statistical analysis. Thirty-three HPV genotypes were analysed including (i) high-risk: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66/68; or (ii) low-risk: 6, 11, 26, 40, 42, 43, 44, 53, 54, 55, 57, 61, 70, 71, 72, 73, 81, 82. We calculated the prevalence of any, high-risk, and low-risk HPV infections. To compare the socio-demographic, behavioural, and knowledge variables, we employed a Chi-square test (or Fisher’s exact test) for categorical variables, and Student’s t-test or Mann-Whitney U-test for continuous variables, as appropriate. We explored the bivariate relationship between HPV infection and possible explanatory variables such as college field, year of study, and city. A multivariable modified Cox regression was performed to determine risk factors—participants’ socio-demographics, sexual behaviours, medical history, HPV knowledge—that were correlated with high-risk HPV infection at time of screening. Initially, variables with a significance level of p<0.10 in the bivariate modified Cox regression were included in the multivariable model. A likelihood ratio test was then used to compare the goodness of fit of the nested models. We obtained adjusted prevalence ratios (aPR) for all comparisons and presented them with the 95% confidence intervals (CIs). All data analyses were conducted in R.
Ethics approval and consent to participate. Institutional Review Boards of the National Institute of Hygiene and Epidemiology, Vietnam (reference number: IRB-VN01057-13/2017) and the ethics board of the London School of Hygiene and Tropical Medicine (reference number: 14207) approved this study. To protect the confidentiality and privacy of the study participants, we replaced personal identifiers from any documents with barcodes and collected data and samples from the participants in private places. Eligible participants were informed of the nature of the study including the risks and benefits they may expect, and the way their data would be used. Written informed consent was obtained from all participants.
Test results were communicated with the participants when available. Any participants found to be positive for HPV16/18 were referred to further gynaecological examination and management.
Results
Participant’s characteristics. A total of 1,500 participants were recruited, with no refusal. Nine students (eight in Hanoi and one in Hue) did not provide sufficient samples (negative for HLA gene), thus their data were excluded from all analyses. The demographic characteristics of the 1,491 female student participants across the three cities — Hanoi, Hue and HCMC — are summarised in Table I. The mean age of female university students across the three Vietnamese cities was 19.8 years (range=18-26 years). Of the 1,491 students screened, HPV DNA was detected in 63 students: a prevalence of 4.2% (95%CI=3.3%-5.4%). The prevalence of any hrHPV infection among the study population was 3.4% (95%CI=2.5%-4.4%) (Table I). The HPV prevalence by University departments, year level and cities are shown in Figure 1. There was little difference between the prevalence of any HPV and any hrHPV infection in Hanoi and Hue, where similar proportions of students studying natural and social sciences were recruited (Table I). Low HPV prevalence (1.2%) was found for the university in HCMC, where there were only students from the Natural Science Department (Figure 1).
Participants’ demographic and behavioural characteristics by city in Vietnam.
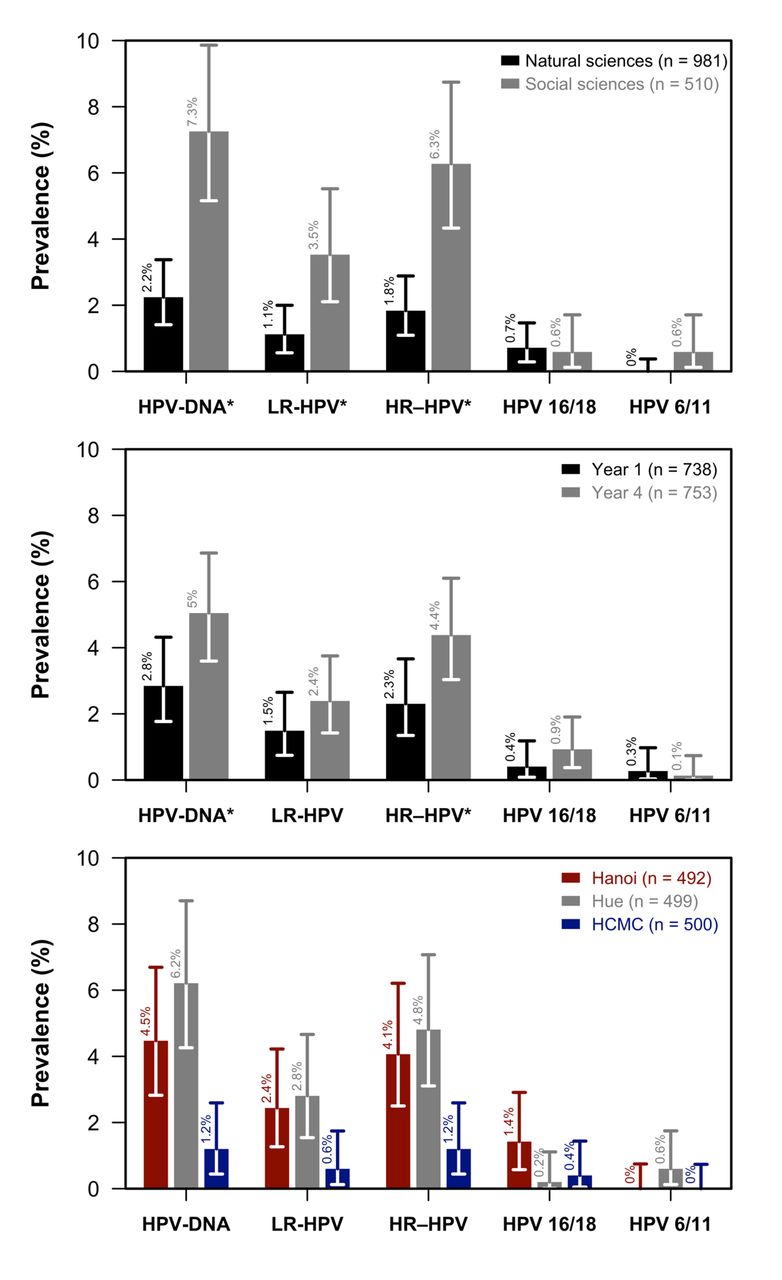
Prevalence of HPV infection among female university students in Hanoi, Hue, and Ho Chi Minh City by college field, year of study, and city. Natural science major/first year (black) and social science major/fourth year (grey) students in the upper and middle panel, respectively; and north Vietnam, Hanoi (red), central Vietnam, Hue (grey) and south Vietnam, Ho Chi Minh (blue) in the lower panel. The high-risk (hr) HPV types include 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66/68 and the low-risk (lr) HPV types include 6, 11, 40, 42, 43, 44, 26, 54, 61, 63, 73, 84, 81, 55. The exact binomial method was used to estimate 95% confidence interval (CI) of HPV infection, depicted by error bars. *In x-axis indicates significant differences (p<0.05) between natural science and social science students, and first- and fourth-year students.
HPV genotype distribution. Twelve high-risk HPV types were found in our cohort (Figure 2); HPV31 and 33 were not detected. HPV52 represents the most common HPV type detected (31.8% of positive samples), followed by HPV39 (17.5%), representing a prevalence of 1.34% (20/1491) and 0.74% (11/1491) for HPV52 and HPV39 respectively. Among the low-risk HPV types, HPV81 was the dominant type, accounting for 20.6% of positive samples (prevalence 0.87%). Multiple HPV types were found in 33 (52%) of the positive samples. Mixed hrHPV and lrHPV infection were found in 25 of them with as many as five types found in some samples. Thirty-seven students (15 in Hanoi, 15 in Hue and seven in HCMC) who reported never having had sex were positive with HPV. Among these, 10 individuals were infected with only low-risk types, and 27 individuals were infected with hrHPV including multiple infections with HPV16, HPV39, HPV52 and HPV56 being the most commonly detected in up to 8 individuals. One individual was co-infected with HPV18, HPV39 and HPV58. No abnormal cytology was found in students who were infected with HPV16 or HPV18. Sixty-eight (4.6%) students who had HPV vaccine were not infected with HPV.
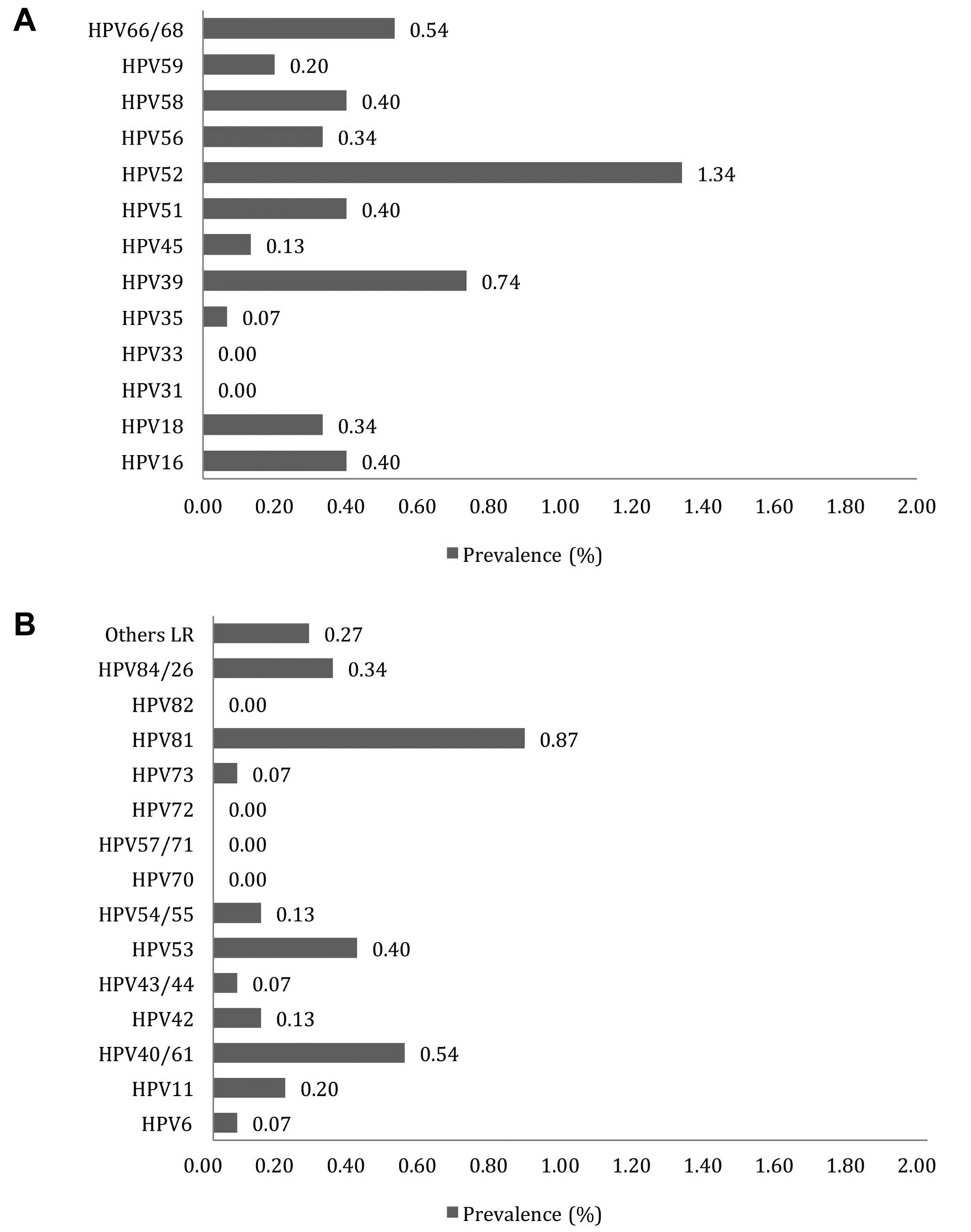
HPV genotype distribution among samples positives with high- (A) and low risk HPV types (B).
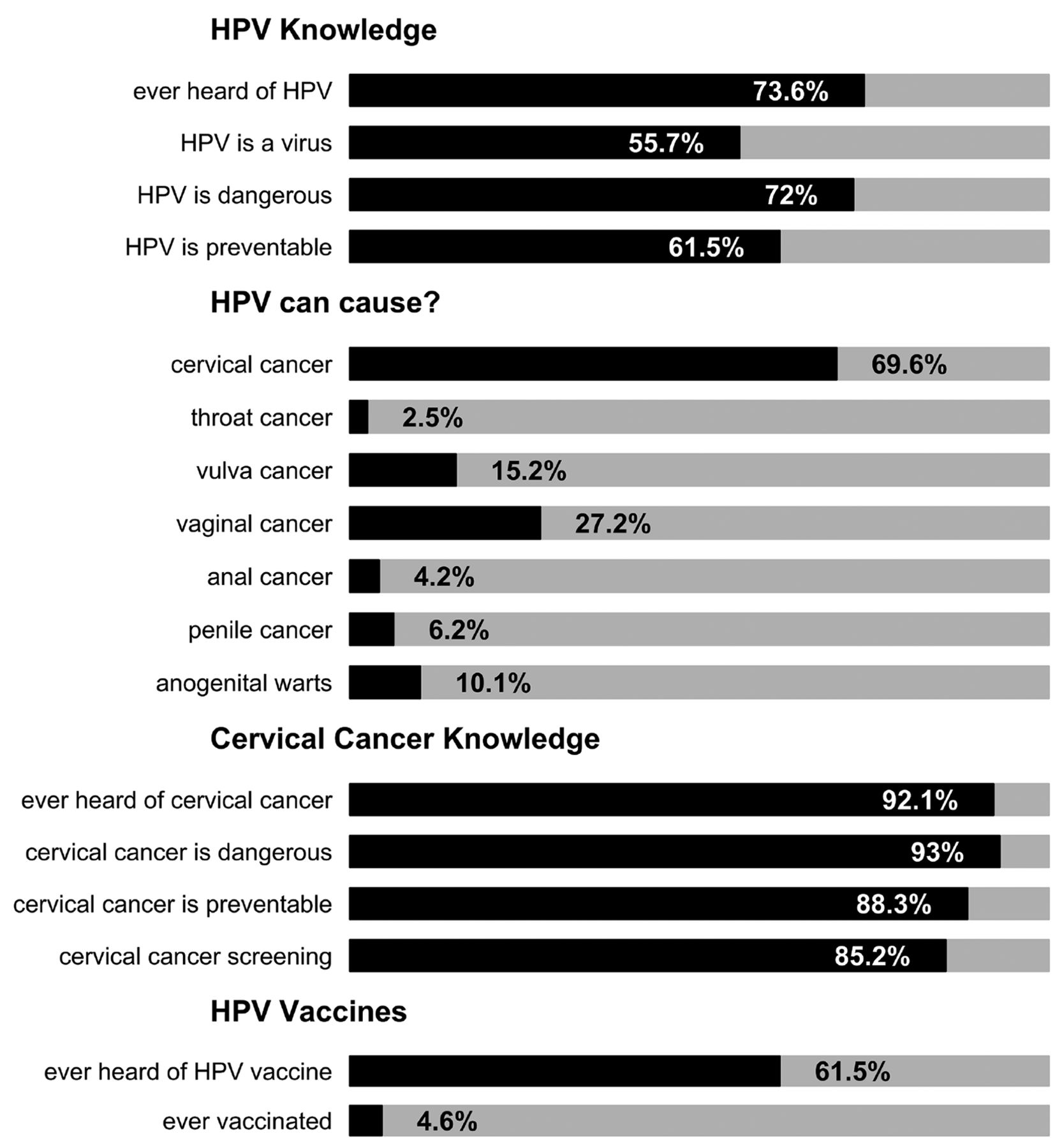
Risk factors for HPV infection. Being older was associated with higher prevalence of HPV infection (p=0.029) (Table II), including hrHPV infections (adjusted prevalence ratio, aPR=1.92, 95%CI=1.07-3.45, p=0.03). Acquiring HPV infection was more likely to be associated with students from the social sciences discipline (aPR, 2.16, 95%CI=1.09-4.27 when compared to age-matched natural science students) and those who have had sex (aPR, 6.22; 95%CI=3.4-11.37) (Table II). Having ever been pregnant was also positively associated with HPV infection (aPR, 4.82; 95%CI=1.93-12.04) (Table II). Knowledge of HPV and cervical cancer. More than half of the study participants had heard about HPV and HPV vaccination (73.6% and 61.5%, respectively), but less than 5% of participants were vaccinated (Figure 3). Final year students had higher HPV knowledge (81.0%) than first-year students (59.2%). However, the majority of students were not aware that HPV causes anogenital cancers and anogenital warts other than cervical cancer.
Correlations of factors associated with high-risk HPV Infection.

HPV and cervical cancer knowledge among female university students in Hanoi, Hue, and Ho Chi Minh City, 2017–2019.
Discussion
In the largest HPV prevalence study among young female university students aged 18-26 years old in Vietnam, we found a low prevalence of any HPV infection, including hrHPV, in Hanoi, Hue, and HCMC. This finding contrasts with studies in other countries. For example, Oh et al. found a higher prevalence of HPV infection (17.5%) among South Korean students aged 17 to 26 years (20). Among the identified HPV types, they reported HPV16, 18 and 35 were the most common and HPV infection was associated with sexual debut, new sexual partners, and smoking (20). Studies in the United States have reported HPV prevalence rates of 19.7% to 44.8% among female university students, depending on their age (11, 21). In the study by Forhan et al., among 838 American women aged 14 to 19 years, the HPV-positive rate was 18.3% (22). In Brazil, Vieira et al. found that 25.3% of students aged 25 years old were infected with HPV (23). In Greece, HPV prevalence of 40-70% were observed among young women aged 18-26 years from outpatient clinics during 2011-2016 with HPV16 and 31 being the most common genotypes (24). According to Institute Catala d’Oncologia, the median age of Vietnamese women at first sexual intercourse ranged from 21.0 to 21.5 years old, corresponding to third or final year in university (25). The low HPV prevalence observed in our study population could be attributed to the low sexual activity/initiation in this age group in comparison to other populations in the studies mentioned above in Korea (21%), Brazil (>75%), USA (61.4%-73.2%). Given the low prevalence of HPV infection among female university students in Vietnam observed in our study, HPV vaccination will protect them from acquiring oncogenic HPV genotypes, particularly HPV16 and 18. We found the prevalence of hrHPV infections was not different in the three Vietnamese cities. However, hrHPV infections were more prevalent among students from the Social Sciences Department in Hanoi and Hue when compared to the Natural Sciences Department in all three cities. One potential factor of the difference in HPV prevalence between the departments may be a reflection of differences in sexual behaviour in social science students in our cohort compared to natural science students.
While most participants know about cervical cancer and more than half had heard about HPV vaccines, only 4.6% of the cohort had been vaccinated. High vaccine costs, accessibility and lack of knowledge regarding HPV and the benefits of the vaccine are likely to be the main barriers to HPV vaccine uptake in Vietnam (26, 27). A 2016 study of 932 college students by Kamimura et al. (495 in Vietnam and 437 in the United States) found that Vietnamese participants had lower levels of knowledge about HPV, more barriers to HPV vaccination (i.e., costs and stigma associated with HPV vaccination) and higher levels of risk denial compared to United States participants. In that study, the percentage of Vietnamese participants who were vaccinated with HPV (7.5%) was much lower than the participants from the United States (42%) (26). There is a need to improve access to HPV vaccine and sexual health education, including benefits of HPV vaccination in this population.
The dominant HPV52 genotype in our study is similar to previous studies in Vietnam and other parts of Asia for example Japan (28, 29). HPV58 and 59, which were the common genotypes in other studies in Vietnam, represented 8% and 4% respectively among the hrHPV genotypes in our study (28). It is important to note that HPV52 and 58 are responsible for a significant proportion of cervical cancer in Asia. We identified HPV 39 and 66/68 the second and third most common hrHPV genotypes in our cohort. HPV39 has been found to be one of the most prevalent HPV genotypes in women in rural areas in Bolivia, Nepal and China (30-32), while HPV 66 was found to be prevalent in Korea, Brazil and Mexico (33-35). Notably, these genotypes except HPV52 and 58 are not present in all licensed HPV vaccines. This finding warrants ongoing surveillance of HPV disease caused by these HPV types, which may be important for future HPV vaccine development.
Effective primary and secondary preventions – HPV vaccination and cytology screening – have shown promise in eliminating cervical cancer (26, 36, 37). Early vaccine impact on anogenital warts is demonstrated in some high-income settings where vaccination was introduced in young adolescents (8, 38, 39). The risk of cervical cancer remains high in many LMICs such as Vietnam because of the absence of routine HPV vaccination and effective cervical screening programmes (28, 29). Most LMICs are challenged with financial and logistic constraints, such as the availability of healthcare infrastructure to implement cervical screening at high coverage (7, 8), high costs of HPV vaccine, the ability to acquire adequate vaccine supplies, and the feasibility of reaching high coverage when vaccinating individuals outside infant vaccination schedules.
Our study demonstrated the feasibility of self-swab in HPV screening in Vietnam. More than 98% of samples from each site were valid for further HPV screening, indicated by the presence of HLA internal control. This collection method would facilitate the HPV screening nationwide allowing for HPV screening with high precision assays, an important component of the HPV related cancer reduction program.
The challenges of a multi-site study include logistical and personnel coordination as well as the standardisation of all study procedures including laboratory testing across different sites. These were mostly overcome by regular meetings between the study groups, rigourous study procedures and well-considered study design. Nevertheless, our study has several limitations. First, our study is based around university students in Hanoi, Hue and HCMC and may not be generalizable to out-of-school females and the whole of Vietnam. Second, no social science students were recruited from HCMC, and this led to potential bias in estimating sexual behaviours and HPV prevalence among female students across the three study cities. Third, culturally, female student participants may under-report socially undesirable behaviours such as their sexual activities, as indicated by the presence of HPV in individuals who reported never having had sexual activity. Last, our recruitment method was calling for volunteers to participate which may have led to participant bias.
Conclusion
In this cross-sectional, multi-site study in Vietnam, we identified a low HPV prevalence rate and low HPV vaccination coverage among female university students. Our study highlighted the potential benefit of a national HPV vaccination program and the need for a health promotion program addressing HPV knowledge in rolling out a vaccine program for young females in Vietnam.
Acknowledgements
The authors would like to thank the study participants and staff of the Vietnam National University in Hanoi, Hue and in Ho Chi Minh City for their involvement with this study. This work was supported by the UK Medical Research Council (MRC), and Vietnamese Ministry of Science and Technology as part of the UK-Vietnam Research Collaboration (Newton Fund), project number HNQT/SPDP/03.16.
Footnotes
↵* These Authors contributed equally to the study.
↵# Equal corresponding Authors.
Authors’ Contributions
KM and NVT conceptualised the study. KM, NVT, SMG, DDA, QDP and HPT contributed to study design. QDP, BTVH, KVN and PTNL were involved in data collection. DTL, LTKL, VC and TDLH screened and genotyped the samples in the laboratory. KP, MJ, MB, KB, QDP, and NVT contributed to statistical analysis and made the figures. KP, ZQT and NVT did the literature review. KP, NVT and MJ wrote the initial draft. All Authors contributed to data interpretation, critically reviewed the manuscript and approved the final version.
Conflicts of Interest
The Authors have declared no competing interest.
- Received August 16, 2021.
- Revision received September 20, 2021.
- Accepted October 1, 2021.
- Copyright © 2022 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.