


Abstract
Background/Aim: Patients after kidney transplants are at risk of cardiovascular morbidity. An elevated resistance index (RI) is associated with renal graft failure, while a decreased RI can be due to a renal artery stenosis. The RI can also be measured in the carotid artery. Whether a correlation between intrarenal RI after kidney transplant in adult patients and the RI of the internal carotid artery exists is still unclear. Patients and Methods: In this prospective cross-sectional study, RI of kidney transplants and of the internal carotid artery were measured with duplex sonography. Carotid intima-media thickness as well as the Framingham risk score and the Augmentation index, all known markers of atherosclerosis, were assessed. Correlations between the RI in Carotid artery and the RI of the kidney transplant were based on Spearmen test with the level of significance set at p<0.05. Results: Ninety-eight consecutive patients [60% male, mean age of 48.7 (±15.6)] were included. The mean interval after transplantation was 27.5 (±8.5) months and mean serum creatinine was 308 (±220.3) mmol/ml The RI of the internal carotid artery and the renal transplant were significantly correlated (p<0.05). A correlation between the RIs and the Augmentation Index was found. Conclusion: The RI of the kidney transplant is correlated with the RI of the carotid artery and to markers of general atherosclerosis. This observation may be helpful to identify patients after kidney transplant with higher risk for cardiovascular events and gain indirect information on transplant renal artery stenosis.
Kidney transplant is the most frequently performed organ transplant (1). Computed tomography (CT) and coronary Angio-CT are used for risk stratification in kidney transplant candidates for risk stratification before transplantation (2). It is the treatment of choice in end-stage renal disease (ESRD) and is ideally performed before initiation of hemodialysis (3). It is also more cost-effective than long-term dialysis (4). Color-coded Doppler sonography (CCDS) is part of the postoperative surveillance (5). The surveillance may start as early as during, but should be initiated immediately after transplant (6). Besides the diagnosis of arterial or venous obstruction, the intrarenal vascular resistance, called Resistance Index (RI) is measured (7). While the RI can be difficult to measure in orthotope kidneys it is often easier to assess in the more superficial transplant in the iliac fossa. Nonetheless, accessibility can be limited due to different factors such as pain, obesity, flatulence amongst others. The RI has been a proven to be sensitive marker of graft dysfunction, but is unspecific (8). The RI of the kidney transplant adapts rapidly to the host (9). An elevated RI of 0.80 (normal range=0.6-0.7) or higher indicates an unfavorable prognosis of renal function as well as increased mortality (10). A decreased RI can be a sign for a renal stenosis (11). RI measurement is observer dependent (12). There is a significant association between an increased RI and markers of generalized atherosclerosis such as the Framingham risk score (FRS), the Carotid Intima-Media-Thickness (CIMT) and the Ankle-Brachial-Index (ABI) but not for renal function measured with the glomerular-filtration-rate (GFR) (13). Krumme et al. showed that recipient age is associated with the RI (14). The RI of the internal carotid artery is a functional parameter for the generalized atherosclerotic process and is correlating well with wall hypertrophy measured as CIMT as a morphologic correlation to atherosclerosis (15). Gerhart et al. showed that indices of systemic atherosclerosis such as the Framingham risk score are superior to ultrasound resistance indices for prediction of allograft survival (16). Augmentation index (AIx) is a parameter measured by pulse wave analysis (PWA) used as a surrogate measure of arterial stiffness and is a useful marker of cardiovascular events (17). A correlation between the RI of renal transplants and the carotid artery as well as the RI of the transplant and IMT, AIx and FRS has never been investigated, but could theoretically be used as a tool to identify patients after kidney transplant with higher risk for cardiovascular events. If the renal RI and the carotid RI were associated, this finding could be useful for the observer if the graft artery and/or the IR was difficult to assess, and a renal artery stenosis suspected: a renal artery stenosis would lead to a discrepant renal-carotid RI.
Patients and Methods
Patients after kidney transplant, that gave their informed consent were consecutively included. All patients that gave informed consent to participate in the study and could withdraw from the study any time. Informed consent was obtained from all subjects. If subjects were under 18, informed consent was obtained from a parent and/or legal guardian.
Patients were consecutively included in this prospective cross-sectional study. They were transferred to our department for CKDS for routine surveillance of grafts or with questions such as renal graft stenosis or AV-fistula after transplantation or decreasing GFR.
Exclusion criterion was the presence of any carotid or renal artery stenosis. Baseline values (including creatinine and creatinine that were used to estimate the GFR using the CKD-EPI Creatinine Equation (2009)) were extracted from the patient chart (18). Patients were included regardless of their GFR to have a broad spectrum of patients as seen in daily practice in a genuine setting. All patients received standard medical treatment for their allograft kidney, including immunosuppressive therapy with steroids and tacrolimus or cyclosporine. Kidneys were transplanted to the iliac fossa with the external artery and vein being the supply vessels.
Colour-coded duplex sonography (CCDS) and spectral analysis. Recognizing pathological findings like stenosis or arterio-venous fistulas becomes considerably easier with CCDS. To demonstrate non-perfused areas, application of a signal enhancer (contrast agent) may be particularly useful (19, 20). Various causes of an elevated RI value are displayed in Table I.
Possible causes of an elevated resistance index [adapted from (30)].
Ultrasound was performed with the ultrasound system iU22 (Philips, Best, Netherlands), a high-resolution ultrasound with integrated software (QLAB). Board certified investigators according to a standardized protocol performed all CCDS. Three representative IMT measurements (QLAB) were bilaterally performed in the wall of the common carotid arteries at defined sites. These six intima-media thickness readings were averaged to give the mean common carotid IMT. The intra-renal resistance index and the index of the carotid artery were measured in the same session.
For the assessment of arterial stiffness using the AIx radial artery pulse wave analysis was performed noninvasively with the SphygmoCor system (AtCor Medical; Sydney, Australia) by a single observer with patients in supine position. Augmented pressure was defined as the difference between the second and the first systolic peak, and AIx was expressed as percentage of the pulse pressure (difference between systolic and diastolic pressure).
A standardized questionnaire was used to compute the Framingham Risk score using the following data: smoking status, record a history of smoking, cholesterol levels, blood pressure, medication for arterial hypertension, diabetes, a family history of premature-onset cardiovascular disease (defined as myocardial infarction or stroke before the age of 65 in first-degree relatives), and current drug intake. The Framingham risk score was calculated for all patients at the webpage of the National Heart, Lung and Blood Institute website (http://www.nhlbi.nih.gov/guidelines/cholesterol/).
Data management and statistical analysis was performed with the STATA software (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC). As the data is not normally distributed but monotonically related; we did not use Pearson correlation – Spearman does not carry assumptions about the distribution of the data. Unless indicated otherwise, continuous data are expressed as means±standard deviation, and compared by Kruskal-Wallis Test. To analyze the association of renal transplant resistance index with various indicators we categorized data firstly in tertiles where possible. Subsequently we compared mean RI of kidney transplant and the internal carotid RI with the tertiles with Kruskal-Wallis test (Figure 1). Correlations between the RI in carotid artery and the RI of the kidney transplant were based on Spearmen test with the level of significance set at p<0.05.
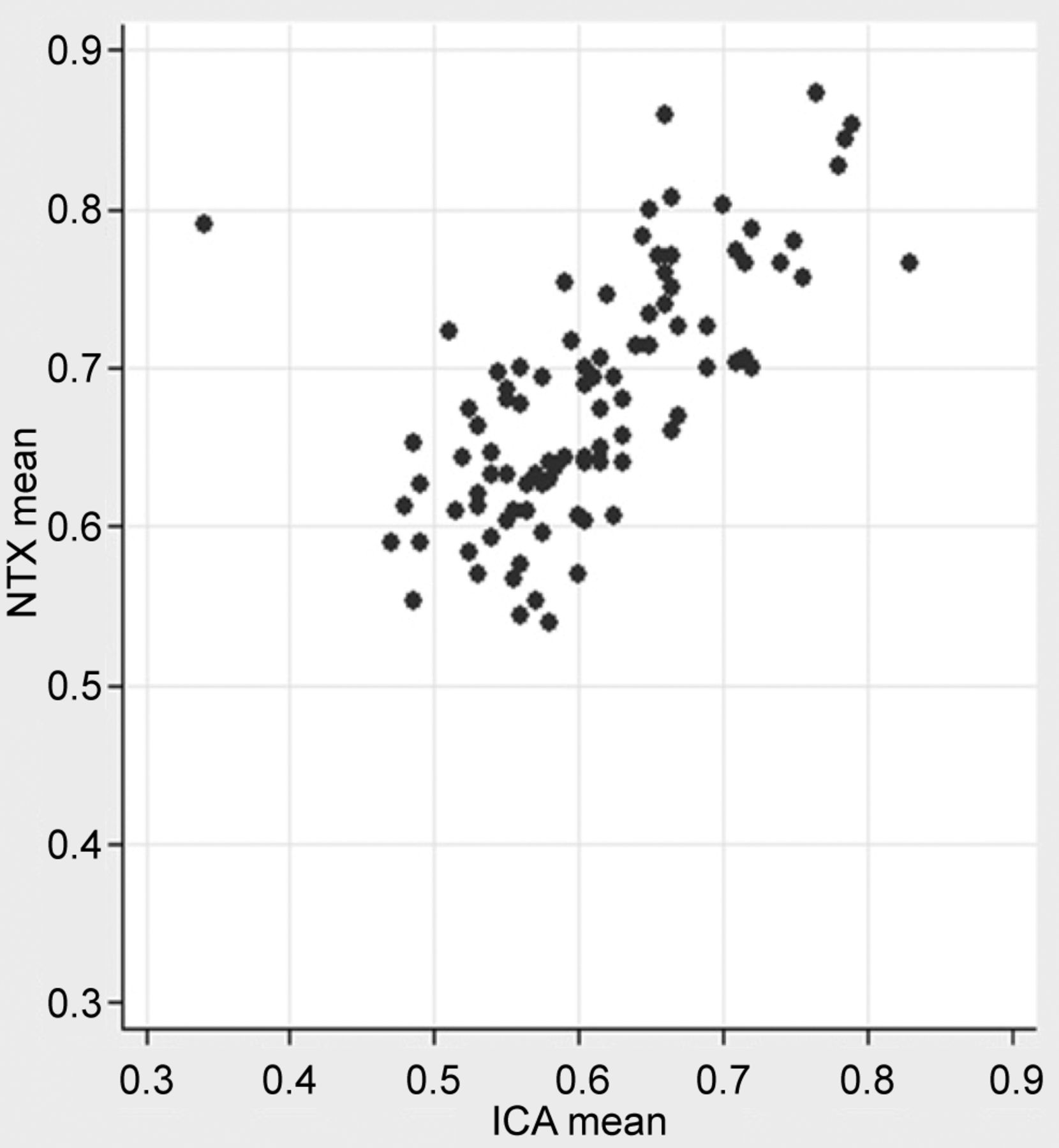
Correlation of kidney transplant-RI and RI of the internal carotid artery. NTX: RI of kidney transplant. ICA: RI of internal carotid artery.
Ethics approval. The Institutional Committee on clinical investigation of the University Hospital Zurich and the cantonal ethic committee Zurich approved this prospective study. All methods were carried out in accordance with relevant guidelines and regulations according to the ethics committee and the Declaration of Helsinki. The study is registered under NCT01001065 at ClinicalTrials.gov.
Results
Ninety-eight patients (60% males, 40% females) were consecutively evaluated between September 2009 and September 2015 and included in this prospective study. The mean interval after transplantation was 27.5 months (±8.5) months and the mean age (48.7±15.6) years. All patients in this prospective cross-sectional cohort received their renal transplant more than 18 months ago.
Patients were consecutively included regardless of their creatinine levels to give a genuine clinical setting without selection bias. The mean serum creatinine was 308 mmol/ml (±220.3). Twenty-eight (28.6%) patients were active smokers, 72 patients (73.5%) were under antihypertensive medication. Baseline characteristics are presented in Table II. A significant correlation of the renal and the carotid RIs with the augmentation Index (AIX) with a coefficient of 0.43 (p<0.05) and the CIMT with a correlation coefficient of 0.58 (p<0.05) as shown in Table III was found. Calculations based on Spearman Test did not show a correlation with renal function and RI. Only patients with a low FRS had a significant correlation with the transplant RI with a coefficient of 0.38 (p<0.05) as shown in Table IV.
Baseline characteristics of included patients.
Spearman’s ranked correlation of NTX RI and various indicators.
Association of RI (NTX mean) with various indicators.
Discussion
Patients after kidney transplant have an elevated risk for cardiovascular events (21). Risk stratification, therefore, depends as well on markers of cardiovascular events. Intrarenal RI is a routinely assessed complex parameter that reflects the arterial compliance and pulsatility rather than renal vascular resistance (22). The function of the allograft is as well routinely assessed with CCDS including the RI (23, 24). RI can also be reliably measured in renal grafts if accessible (25). Päivärinta et al. assessed the kidney function with PET-CT and RI measurements with CCDS to show that the RI was correlated with perfusion and fibrosis of the transplants (26). Boran et al. found an association between recipients with proteinuria <1,000 mg/24 h, and elevated RIs (27). Radermacher et al. showed that an elevated RI was a strong predictor of allograft loss (10), but there is an ongoing discussion if the RI was sensitive and specific enough to discriminate between the different causes for acute graft failure (28). In our population of 98 adult patients with previous kidney transplants we found a significant correlation between the mean kidney transplant RI and mean internal carotid artery RI with a correlation coefficient of 0.69 (p<0.05).
Measurement of flow in the graft vessels and of the measurements of the RI help to exclude early thrombotic complications (8). Further, there is evidence that the RI obtained during the first 6 months after transplant failed to predict kidney allograft failure, whereas the RI obtained 12-18 months after transplantation appeared to be useful to predict long-term allograft outcomes (29). All patients in this prospective cross-sectional cohort received their renal transplant more than 18 months ago. This is important to recognize, as the hemodialysis period and the etiology of the end-stage renal disease as well if the donor was deceased or if it was a living donation and ischemia time have an impact on the transplant-RI. But as discussed above, the RI of the transplant adopts quickly to the recipient and should therefore reflect the recipients RI and not the donors former RI after this period (>18 months) of time. They were consecutively included, regardless of the GFR to give a genuine clinical setting without selection bias.
Heine et al. found that the RI in renal transplants is associated with systemic atherosclerosis as well as subclinical atherosclerotic vessel damage and is, therefore, not only a marker of renal but of vascular damage. They also showed that markers of cardiovascular risk or systemic atherosclerosis are superior outcome predictors for cardiovascular events compared to renal RI (30, 31). Heine et al. included 105 renal transplant recipients in their study and used the FRS, the intrarenal RI, the pulsatility index (PI), the IMT, and ABI to assess risk for cardiovascular events and subclinical systemic atherosclerosis in these recipients(13). They concluded that the renal RI rather than a specific marker of renal dysfunction is a complex integration of different factors, including arterial compliance, arterial pulsatility and peripheral resistance. According to Heine et al., the RI is associated with traditional cardiovascular risk factors and with subclinical atherosclerosis. They also proposed that the RI is not related to the GFR. For this reason, we included patients regardless of renal function as measured by GFR and also found, that the RI seems not to be related to the GFR. However, Heine et. al (or others) did not assess the carotid RI in their work. The carotid RI is technically easier to measure and could also be measured by health care professionals, that are less well trained in more complex renal ultrasound exams. The pathophysiological aspects of the relationship between renal microcirculation and cardiovascular system were further described by di Nicolò and Granata (32). Brennan and Lentine found this result (RI being associated with traditional cardiovascular risk factors and with subclinical atherosclerosis) also in their cohort of patients with kidney transplants. They also used blood samples to measure (amongst others) inflammatory markers. Cardiovascular risk factors and comorbidities were then assessed by a questionnaire. They also studied the risk of coronary heart disease by using the FRS. RI and PI were calculated by CCDS as well as IMT and ABI included in the study data (33). The same parameters were used in our study but also the carotid RI was measured (Heine et al. suggested measurements in native non-renal organs) as well as the AIx. The above shown results are according to the results of Heine et al. and Brennan and Lentine and show that the RI is associated with traditional cardiovascular risk factors. Especially the AIX, that was not measured in the other studies, correlates with subclinical atherosclerosis. AIx is used to measure arterial stiffness as a sign of vascular compliance and was associated with elevated RI. This correlation between RI and changes in vascular compliance/resistance was also shown using an in vitro model (34).
The mechanisms that lead to an increase of the intrarenal RI are still not clarified. While Naesens et al. found, that the transplant kidney is not associated with graft function and graft survival but is associated with recipient survival, Granata et al. proposed, that the transplant kidney RI is increased when tubulointersitial damage is present (35, 36). Discrepant findings in the literature and discouraging clinical experience led some clinicians to abandon the RI as a reliable parameter. Greater understanding of the theoretical basis of the RI might help the RI to live up to its promise as a parameter for measuring changes in renal status. The RI is sometimes difficult to access, even in transplants. A decreased intrarenal RI can be a sign of a renal stenosis. In patient with orthotope kidneys, the RI can be compared. This is not reasonable if the patient has a transplant kidney. If the observer is in doubt, if a renal graft stenosis is present, the renal-carotid RI may be compared and should be within the same range. In case of the kidney transplant, the RI cannot be compared to an orthotope kidney. The brain is also a parenchymal organ. The RI can be measured in the internal carotid artery. The RI of the internal carotid artery reflects atherosclerotic changes in intracerebral arteries. Chung et al. found that an elevated RI is related to a higher risk of cardiovascular events (37). We could also show that there is a positive association between mean kidney transplant RI and mean internal carotid artery RI, so we propose, that the RI of the internal carotid artery and the kidney transplant are comparable. A next step would be to compare intrarenal RI in patients with renal artery stenosis and the internal carotid RI to harden this suggestion.
We could not show a positive correlation between renal function and RI as described in former studies (14, 38). Only patients with a low FRS had a significant correlation with the transplant RI in our cohort, while Heine et al. found that renal transplant recipients with a high cardiovascular risk had increased RIs. There was a significant correlation with CIMT in our study as a sign of elevated cardiovascular risk that was also found in the two above mentioned studies (13, 33). As described by Heine et al. we also found no significant correlation between renal function and CIMT.
Conclusion
Traditional cardiovascular risk factors and markers of subclinical atherosclerosis are related to elevated RIs in renal transplants. As the renal RI is correlated with carotid RI it might be more a general parameter of vascular compliance rather than an exclusive marker of intrarenal resistance. This finding might facilitate the mitigation of the cardiovascular risk in patients with kidney transplants. The measurement of carotid RI is technically easier to perform and could, therefore, be used by a larger number of health associated personnel and as well as used an indirect marker for the suspicion of a renal artery stenosis if there is a gradient in the renal-carotid RI, justifying further imaging with CT or MRI with potentially graft-harming contrast agent.
Acknowledgements
We thank Elisabeth Beckmann, Ph.D., MsC, MA, BA for the statistical analysis, figures and tables and her support.
Footnotes
This article is freely accessible online.
Authors’ Contributions
P.K. collected data, contributed to the data, wrote the paper and reviewed the paper. S.E. analyzed the data, wrote the paper and reviewed the paper. CT designed the study, collected data, contributed to the data, and reviewed the paper. R.W. took part in the study design, reviewed the results, contributed to the style and reviewed the paper. MLV collected data, contributed to the data, wrote the paper and reviewed the paper. NK reviewed the results, contributed to the style and reviewed the paper. RC designed the study, collected data, contributed to the data, wrote the paper and reviewed the paper.
Conflicts of Interest
There are no conflicts of interest.
- Received July 4, 2021.
- Revision received August 23, 2021.
- Accepted August 31, 2021.
- Copyright © 2021 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}