


Abstract
Lipomatous meningioma (LM) is a form of metaplasia, originating from intracellular lipid bodies accumulation due to metabolic alterations. A comprehensive literature review was performed introducing further elements of evaluation. The parameters utilized were age, sex, location, clinical presentation, imaging features, treatment, and recurrences. Seizure and headache are the primary onsets of symptoms. Further LM clinical features, such as visual disturbances and visual epileptic seizures were examined. Symptoms may occur ten years prior to LM finding and it can resolve completely with the indicated surgery. LM computed tomography imaging analysis reveals hypodense regions due to the presence of fat content. On magnetic resonance imaging, the lesion displays hyperintense signal in T1-T2 with signal loss in the fat-suppression sequences. Immunohistochemically, lipidized meningioma cells are positive for Epithelial-Membrane Antigen, Vimentin, CD99, S-100 protein, and progesterone receptor. The recurrence risk rate of LM is estimated to be around 17%. Precise immune-histological findings have been correlated with imaging features to help with early diagnosis. A defined diagnosis of LM is a crucial factor in the choice of treatment.
Meningiomas are the most common benign intracranial tumours, accounting for 36% of all central nervous system (CNS) neoplasms. Their incidence, increasing with age, remarkably rises after the age of 65. Meningiomas are approximately twice as common in females than males and are estimated to be three times more common in females of the 35 to 54 years old age group. Meningiomas are tumours of mesodermal origin, thought to grow from the arachnoid cap cells of the arachnoid villi and granulations. According to the 2016 World Health Organization (WHO) classification scheme, they are classified into three groups: grade I (benign), grade II (atypical), and grade III (anaplastic). Approximately 80% of meningiomas are WHO grade I. Surgery, aiming at gross total resection (GTR), is the treatment of choice for symptomatic WHO grade I meningiomas. WHO classification of CNS tumors stratifies grade I meningiomas into: (a) meningothelial, (b) fibrous (fibroblastic), (c) transitional (mixed), (d) psammomatous, (e) angiomatous, (f) microcystic, (g) secretory, (h) lymphoplasmacytic-rich, and (i) metaplastic (1). According to Kasantikul et al. (2), this diversity may be related to the capability of arachnoidal cap cells to undergo de-differentiation, thus transforming into different mesenchymal cell types (2). Lipomatous metaplasia is an infrequent and rare histological finding. The first case described was the one described by Bailey and Bucy in 1931 (3). Since then, a total of 64 cases have been reported in the literature. Other elements from our case, here reported, aimed at contributing to the current knowledge of this rare pathology in terms of differential diagnosis and prognosis.
Literature Review
In the literature, we have reviewed and collated all the cases reported to date of lipomatous meningioma in the last 35 years. The terms used for the PubMed database search were “Lipomatous” and “Lipoblastic meningioma”. Xanthomatous meningiomas, cutaneous neurofibromas, and liponeurocytoma were excluded from the search. Initially, 52 manuscripts were found and evaluated. Records identified from reviewed references were examined and resulted in further 154 manuscripts. The inclusion parameters were age, sex, onset and duration of symptoms, imaging characteristics [computed tomography (CT) and magnetic resonance imaging (MRI)], treatment, histology, immunohistochemistry, and follow-up. In total, we have selected 64 cases of lipomatous meningioma. The selection process is illustrated in Figure 1, using the Prisma Flow Diagram.
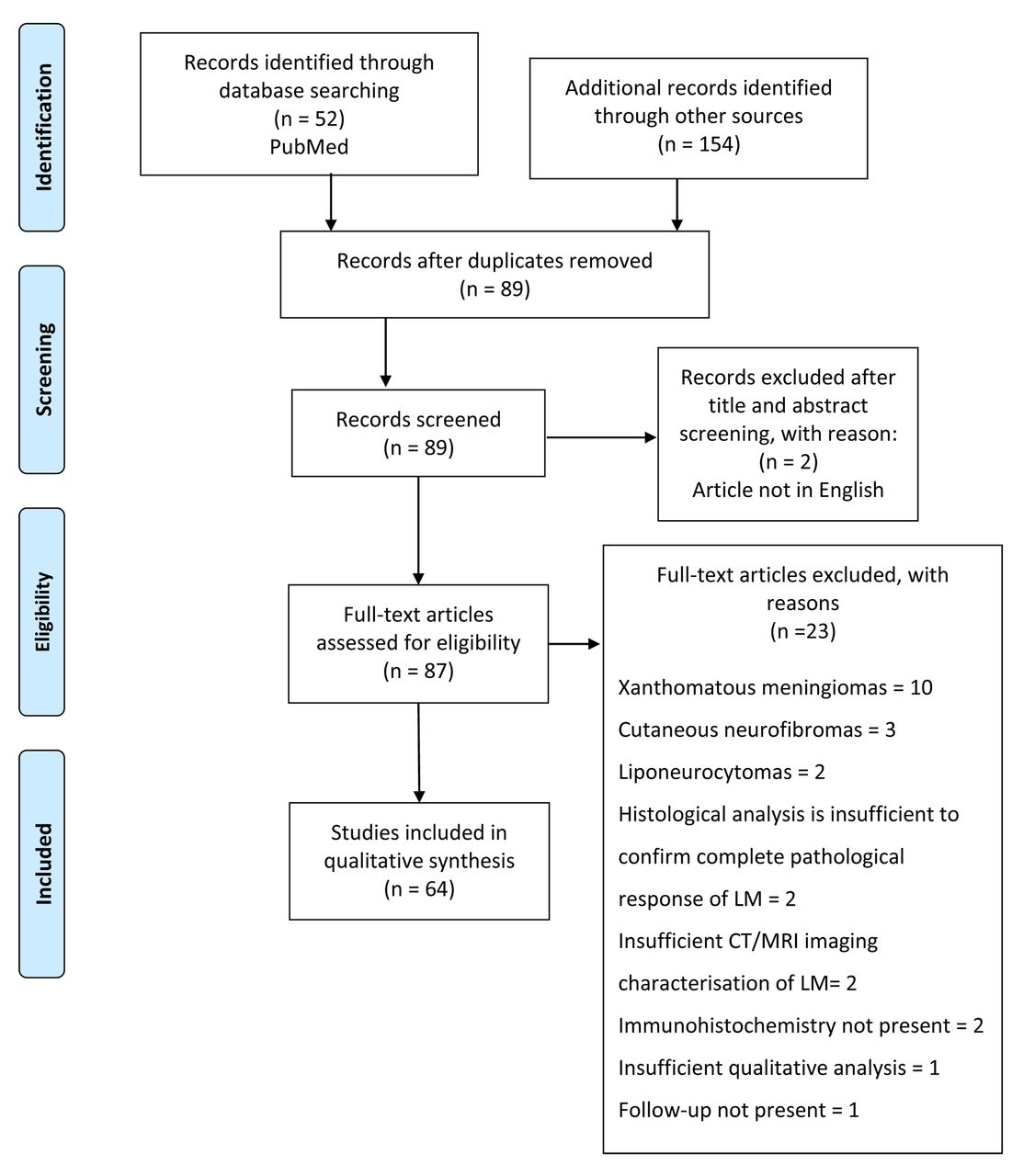
Flow chart of the work selection process.
Ethical approval. Institutional review board/ethics committee approval was not required for this study. All procedures performed in the studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Discussion/Observations
Pathophysiology. Lipomatous meningiomas are benign lesions, World Health Organization (WHO) grade1, with a good prognosis. According to the WHO 2007 classification of meningiomas, it is considered a subtype of metaplastic meningioma, and includes tumors that contain different types of mesenchymal cells able to differentiate into different subtypes (metaplastic changes), including fat cells (4). Metaplastic differentiation commonly occurs in some subtypes of meningiomas such as meningothelial, transitional, and fibrous (5). Specifically, these types of meningioma contain meningothelial cells that resemble adipocytes or lipoblasts (6). The terms lipoblastic or lipomatous meningioma were used to refer to this type of meningioma. In 2003, Bolat et al. coined the term “lipidised” to indicate all meningiomas with those characteristics typical of lipomatous meningiomas. We have analysed 64 cases to perform a literature review and to understand the characteristics of lipomatous meningiomas better. Our study revealed that fat accumulation occurs mainly in meningiomas of the meningothelial and transitional types (7). These neoplasms contain a mixture of meningothelial-type cells and cells with a predominant adipocyte tissue type. In the literature, we have found four cases of the secretory meningioma type with a lipomatous component. Yamada et al. reported the first case in 1999 (8), the second one by Matyia et al. in 2005 (9), the third one by Patil et al. in 2017 (10), and the last one by Khubrani et al. in 2019 (11). Secretory type meningioma can be the result of the transformation into the secretory form by meningothelial cells; the underlying mechanism involves the altered glycosylation of the tumour cells (12). In the past, it was assumed that fat accumulation in meningioma was due to metaplastic alteration of meningothelial cells (13). However, recent studies demonstrate that lipids’ accumulation is due to a metabolic abnormality of the tumour cells rather than true metaplasia (14, 15). The proportion of adipocyte component varies from 10% to 90% (7, 16, 17). The cytoplasm of the lipidated tumour cells contains large fat droplets; nuclei are shifted to the periphery and composed mainly of triglycerides (18). These characteristics differentiate the lipomatous meningioma from the xanthomatous meningiomas in which they present central nuclei mostly composed of cholesterol (19). Also, lipid cells contain common cytoplasmic elements, interdigitated cellular processes, and desmosomes (16). Other differential diagnoses include liposarcoma, chondroma, metastatic mucinous carcinomas, giant cell glioblastomas, and epidermoid cysts.
Clinical Presentation
Like most subtypes of meningiomas, lipomatous meningioma most frequently affects women rather than men. Symptoms are related to the meningioma’s size and location; similarly, to other meningiomas subtypes, seizures and headache are the main onset symptoms. Seizures are most likely associated with tumours located in the frontal and temporal areas, whereas headaches with parietal tumours (6, 15). Almost all intracranial lipomatous meningiomas occur in the supratentorial location with frontal and parietal areas as the most common sites. In our presented case and the one of Okamoto et al., the lesion’s implantation was on the tentorium (20). Roncaroli et al. and De Eulate-Beramend et al. reported three cases in the spinal location. Kasantikul et al. reported a case of LM correlated with an arteriovenous (AVM) malformation (2); according to the author, the presence of the coexistence of the AVM and meningioma, was explained by the chronic irritation of the arachnoid cells, which can then stimulate the growth of meninges lesions (21).
In the case reported by Kasantikul et al. (2), symptoms manifestation such as headache and seizures were related to the angioma rupture as suggested by the findings of erythrocytes and hemosiderin in the tissue surrounding the meningioma. Kashimura et al. described a temporal lipomatous meningioma, which was initially treated conservatively. This meningioma was bleeding in the subdural space, leading to the formation of subdural hematoma. The hypothesis of the bleeding was attributed to the rupture of abnormal vessels. They developed in the tumour mass comprising capillaries and venules with walls of different thickness, which constituted the tumor’s vascular network (22). Kimwada et al. analysed a woman of 74 years affected by a renal cell carcinoma that metastasised and developed in a lipomatous meningioma; the lesion was composed of a central portion of metastasised tissue originating from the renal carcinoma and a peripheral portion consisting of microcystic meningioma tissue with focal lipomatous metaplasia (23).
Assessment and Diagnosis
Patients analysed in this review are in the range of 14 and 90 years old, with an average of 57 years. Forty patients were female; the patients’ total ratio was M: F = 1: 2. Duration from symptoms onset to treatment-outcome spanned from 10 years to 10 days. Onset of symptoms were mainly headache in 34% (n=22) of the cases (total cases n=64) and epileptic seizure in 36% (n=23), followed by visual disorders 11% (n=7), hemiparesis 9% (n=6), and gait instability 6% (n=4). Less frequent symptoms such as behavioural disorders suggestive of a frontal lesion, memory loss, and confusion, each accounted for 5% (n=3), and other minor symptoms included muscle such as weakness, spinal cord compression, attention deficit, and dysphasia, each found in 3% (n=2). Six percent of the cases (n=4) was accidentally detected on imaging investigations (Table I).
Lipomatous meningioma associated clinical characteristic at the onset of symptoms.
At CT imaging, traditional meningiomas appear as solid extra-axial lesions with dura attachment; they present density similar to the cerebral parenchyma with homogeneous contrast enhancement. Lipomatous meningiomas show a hypodensity appearance because the fat tissue component has attenuation values between -50 and -100 Hounsfield Unit (H.U.) (24). When the adipose component is abundant, the lesions present a hyperintense signal in the T1 weighted images and T2 weighted with signal loss in the sequences with fat suppression. If the adipose component is less predominant, the signal is isointense in T1 and T2 (25). The contrast enhancement is homogeneous. Oedema is not ordinarily present. The presence of oedema is a sign of parenchymal tumour invasion. However, oedema can be related to the vascular endothelial growth factor (VEGF) production by meningothelial cells in the case of specific subtypes of meningiomas (e.g., secretory) with the absence of parenchymal tumour invasion (15). Perfusion-weighted Magnetic Resonance imaging (PWI-MR) performed on a case of lipomatous meningioma shows an unusual hypovascularisation of the lesion demonstrated by the extremely low levels of relative cerebral blood volume (rCBV) (26). Colnat-Coulbois et al. reported a case of temporal lipomatous meningioma with hyperostosis of the large sphenoid wing (27). Kim et al., instead, reported the case of a 49-year-old man with a parietal lipomatous meningioma with an erosion of the internal boarding of the bone (6). Intraoperatively, the tumour has well-defined margins and a brown-yellowish appearance, with a visible adipocyte component. Histologically, it is composed of adipocyte-like cells within a conventional type meningioma (11). These adipocyte-like cells are elongated with tapered ends and round nuclei with eosinophilic cytoplasm. Mitotic index is very low, the Ki67 marker for proliferation rate shows values less than 1% (6). Immunohistochemically, lipidated meningioma cells are reactive for epithelial membrane antigen (EMA), Vimentin (VMT), CD99 and S-100 protein and negative for Glial fibrillary acidic protein (GFAP) (28). They are also positive for progesterone receptors but not for estrogens; in fact, the presence of progesterone receptors has been reported to be correlated with a more severe form and recurrences (29). Also, these cells are negative for Calretinin; a highly sensitive but not specific marker for adipocytic tumours. These histopathological features are essential diagnostic elements to differentiate this tumour’s typical lipomatosis process from other diagnoses.5 In the presence of evident areas of the tumour lipidisation, the differential diagnosis between lipomatous meningioma and lipoma relies on the immunohistochemical analysis; positivity for EMA, and negativity Type-4 Collagen confirms the diagnosis of lipomatous meningioma (16). EMA and VMT are distinctive markers for meningiomas that reflect epithelial and mesenchymal cells (30); markers of immunoreactivity such as EMA, VMT, S-100, and progesterone receptors confirm the meningothelial differentiation (27). Cases in which both secretory and lipidated cells are present, the hyaline inclusion bodies of the secretory type meningioma result positive for periodic acid Schiff (PAS) stain as well as carcinoembryonic antigen (CEA), with surrounding CK-positive tumour cells (11). The presence of fat tissue is definitively diagnosed with the histological and immunohistochemical examination. Besides, a precise evaluation of the lipomatous meningioma’s radiological features is of fundamental importance to characterise the benign nature of such tumour (31). Hypodensity, displayed in CT images, is often associated with cystic degeneration, tumour necrosis or previous haemorrhage (13), while hyperintensity in T1-weighted MRI is frequently associated with lipomas, teratomas or met-haemoglobin (13). Macroscopically, the lesions were yellowish, soft, and difficult to differentiate from adipose tissue. The different histological findings of lipomatous meningiomas are described as meningothelial meningiomas with a lipomatous component in 38% of cases, transitional meningiomas with a lipomatous component in 12% (7, 25, 27, 32, 33), secretory meningioma with a lipomatous component in 8% (8-11, 34), microcystic meningioma with a lipomatous component in 3% (7, 27), and in only one case the histological diagnosis was Chordoid Meningioma with a lipomatous component (7). The meningothelial cell with lipomatous metaplasia exhibited immunoreactivity to Epithelial Membrane Antigen (EMA) in 37 cases (5, 7-10, 15,16, 23-28, 33, 35, 36), and Vimentin in 15 cases (5, 9, 10, 15, 16, 23-26, 28, 35-37). Ten meningiomas presented progesterone receptor (5, 6, 15, 27, 33, 34, 37), nine meningiomas showed S100-Protein (11, 24, 26, 27, 35, 36), three meningiomas presented CD99 (27, 37), three meningioma showed Cytokeratin (8, 11, 34), and two cases resulted positive for CEA (8, 11).
Treatment
Almost all found lesions were located in the supratentorial region (frontal, temporal or parietal lobe), except for 3 cases (7, 32), in which the spine was involved. Lattes et al. described a single case of extra-axial meningioma on the orbit (35). The tumours showed a hypodensity signal on CT images, except in two cases (15, 24), in which the lesion presented a hyperdense appearance with hypodense foci inside. Depending on the degree of fat component, meningiomas can be seen at CT images as hyperintense or hypointense with hyperintense foci in weighted T1, and hypo-isointense or hyperintense sequences in T2-weighted sequences. The contrast enhancement, if present, is homogeneous. In this review, all lesions were surgically removed; the partial resection procedures were six, and the total resections were thirty-nine. When the resection was completed, the reported follow-up showed no recurrences.
Prognosis and Results
Roncaroli et al. estimated the recurrence rate of lipomatous meningioma to be around 17%, reporting 3 cases of recurrence out of 18 total cases. These 3 cases presented recurrence at 7, 8 and 24 months. Also, these recurrences were related to cases that had undergone incomplete resection (7). Lipomatous meningiomas are classified as WHO grade I tumours, however, cases in which the tumour characteristics differed from the canonical features have been found. Aage et al. has described a case of lipomatous meningioma with hypercellularity, small cell changes, and a sheathing pattern suggestive of atypical meningioma of WHO grade 2 tumours (38). Sadiya et al. described the case of a recurrent meningioma, which presented characteristics of an atypical type (mitosis >4/10 hpf), lipomatous type meningioma, and focal papillary features (37). Therefore, it is crucial to correctly identify these features which are related to the aggressive form of the tumour and a higher rate of recurrence (37).
Conclusion
Upon reviewing the literature, examining the available LM cases descripted, we have collated and presented the typical features that can be useful in correctly identifying this rare type of meningioma. The main clinical characteristics of LM at onset of symptoms are epileptic seizures followed by headache and migraine with or without visual aura. The imaging analysis of the LM cases revealed helpful characteristics to correctly classify and distinguish the lipomatous type meningioma from lesions of different origin, which can present similar density or intensity at MRI sequences, but malignant behaviour. The specific histologic and immune-histological findings have been correlated with the radiological features, which can alone allow earlier identification of the tumour. Regarding the surgical intervention, a partial or not complete resection with residual tumour is associated with a high rate of relapse. In the cases analysed, a complete safe resection “en bloc” of this type of rare tumour is the suggested surgical treatment that has shown a favourable outcome and is associated with a low recurrence rate. Therefore, the accurate identification of LM by the combination of imaging and immune-histological features is essential for the correct choice of surgical treatment.
Acknowledgements
This research was funded by the Ministry of Foreign Affairs and International Cooperation of Italy (MAECI) project number CN18GR10.
Footnotes
This article is freely accessible online.
Authors’ Contributions
Conceptualisation, P.L. G.Z.; methodology, P.L. and G.Z; investigation, P.L., P.F., P.B, G.Z.; resources, A.S.; data curation, P.F and P.B.; writing – original draft preparation, P.L.; writing – review and editing, P.L.; visualisation, R.C., X.L.; supervision, G.F.; funding acquisition, G.F.
Conflicts of Interest
The Authors declare that they have no conflicts of interest in relation to this study.
- Received August 10, 2021.
- Revision received September 18, 2021.
- Accepted September 20, 2021.
- Copyright © 2021 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.