


Abstract
Background/Aim: Concomitant proton pump inhibitor (PPI) and immune checkpoint inhibitor (ICPI) were determined as risk factors of acute kidney injury. To identify the type of PPI associated with ICPI-induced nephritis, we used the Japanese Adverse Drug Event Report database. Patients and Methods: ICPIs (nivolumab, pembrolizumab, ipilimumab, atezolizumab, durvalumab, and avelumab) and PPIs (esomeprazole, omeprazole, vonoprazan, rabeprazole, and lansoprazole) were selected as suspected nephritis-inducing drugs. Results: The cases of concomitant use of atezolizumab and rabeprazole, ipilimumab and omeprazole, ipilimumab and lansoprazole, nivolumab and esomeprazole, nivolumab and omeprazole, nivolumab and rabeprazole, nivolumab and lansoprazole, pembrolizumab and esomeprazole, as well as pembrolizumab and lansoprazole had a significantly higher reported odds ratio than monotherapy cases. Conclusion: Male patients or patients using ICPIs and PPIs (excluded vonoprazan) concomitantly should be monitored for renal function after chemotherapy.
Immune checkpoint inhibitors (ICPIs) are used as essential anti-cancer chemotherapy in various types of cancers (1-5). Blockade of programmed cell death-1 (PD-1)/PD-ligand-1 signaling (6, 7) and cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) signaling (8) activates T-cell mediated antitumor immunity; therefore, ICPIs exert dramatic effects in patients with cancer expressing these proteins. As ICPIs induce antitumor effects by reactivating antitumor immunity, they also cause immune-related adverse events (irAEs), such as interstitial pneumonia and nephritis (9-11), thyroid dysfunction (5, 9), type 1 diabetes mellitus (5), and lupus erythematosus (12). The clinical features and outcomes of ICPI-induced acute kidney injury (AKI) have been reported (13-15). As a pathological feature, acute tubulointerstitial nephritis was the primary pathologic lesion with lymphocyte infiltration. In addition, lower baseline estimated glomerular filtration rate (eGFR), use of proton pump inhibitor (PPI), and ICPI combination were determined as risk factors of ICPI-associated AKI (13). Furthermore, the mortality of patients with renal recovery after ICPI-induced nephritis was better than that of patients without renal recovery (16). To improve prognosis for patients treated with ICPIs, the prevention of ICPI-induced nephritis is essential.
PPIs are traditionally widely used for the treatment of several acid-related disorders, including peptic ulcer disease, gastroesophageal reflux disease, and Helicobacter pylori eradication. Although the use of PPIs was perceived as safe, it is associated with the incidence of AKI (17-22). In particular, omeprazole is associated with acute interstitial nephritis (AIN) (17). Because AKI and AIN increase the risk of chronic kidney disease (CKD), the prevention of PPI-induced AIN could decrease the initiation of dialysis (23-25).
Since the frequency of overall incidence of ICPI-induced AKI is 2.2% (26), the information regarding ICPI-induced AKI is limited. In addition, it remains unclear as to which PPIs increase the risk of AKI. The Japanese Adverse Drug Event Report (JADER) database is an open-access database of adverse drug events (ADEs). The JADER database is useful for calculating ADE signals in rare cases. The frequencies of irAEs associated with ICPIs were approximately 50% (skin disorders), 40% (gastrointestinal disorders), 8% (endocrine disorders), 4% (hepatitis), and 1% (pneumonitis) in advanced melanoma (14). Because of their low frequency, the signals of irAEs for nephritis/renal dysfunction, pneumonitis, rash, and type 1 diabetes mellitus associated with ICPIs were calculated using JADER (27). However, information on drug-drug interactions is limited. In this study, we aimed to elucidate the type of PPI associated with ICPI-induced nephritis and used the JADER database.
Patients and Methods
Data source. Data from April 2004 to September 2020 were extracted from the JADER database. The JADER database consists of four data tables: patient demographic information (demo), drug information (drug), ADEs (reac), and primary disease (hist). The duplicated data in the “drug” and “reac” tables were removed, and the “demo” table was linked to the “drug” and “reac” tables using each case identified in the data tables. In these cases, the contribution of the medications to the ADEs was classified into three categories: “suspected medicine”, “concomitant medicine”, and “interaction”. The “suspected medicine” category was extracted into ADEs in the present study.
The “demo” table contained data for patient sex and age, as well as other patient characteristics. Data without sex or age information were excluded from the dataset. For the association analysis performed with patients classified in 10-year age intervals, we defined “older adults” as those in their “70s”, “80s”, “90s”, and “100s”, according to a previous report (28). Nivolumab, pembrolizumab, ipilimumab, atezolizumab, durvalumab, and avelumab were selected as suspected drugs for analysis of irAEs. These ICPIs have been approved by the Japanese Ministry of Health, Labor, and Welfare.
Definition of cancer patients. The primary disease in the “hist” tables was defined on the basis of the preferred terms (PTs) in the Medical Dictionary for Regulatory Activities (MedDRA) version 23.1. MedDRA term grouping at the PT level defines the patient’s medical condition. Cancer as a primary disease as defined by PTs is shown in Table I after removing duplicated data. Other cancers not included in Table I that appeared as primary diseases were classified as others/uncertain.
Preferred terms to define different cancer types (appearing in the Medical Dictionary for Regulatory Activities version 23.1).
Definition of ICPIs and nephritis as irAEs. ICPIs (nivolumab, pembrolizumab, ipilimumab, atezolizumab, durvalumab, and avelumab) and PPIs (esomeprazole, omeprazole, vonoprazan, rabeprazole, and lansoprazole) were selected as suspected nephritis-inducing drugs. The ADEs in the “reac” table were coded according to the PTs in the MedDRA. Nephritis as an irAE was selected by three nephrologists from the MedDRA, and the PTs for nephritis are listed in Table II.
Preferred terms to define nephritis as an immune-related adverse event (appearing in the Medical Dictionary for Regulatory Activities version 23.1).
Statistical analysis. The reporting odds ratio (ROR), which serves as an index for adverse event signals, was calculated using the following equations (28), with a, b, c, and d cross-tabulation as follows: a, number of cases with an ADE related to the use of the suspected drug; b, number of cases with an ADE related to the use of all other drugs; c, number of cases with all other ADEs related to the use of the suspected drug; and d, number of cases with all other ADEs related to the use of all other drugs.
ROR=(a/b)/(c/d)=ad/bc
Adverse event signals were recognized as significant when the ROR estimates and the lower limits of the corresponding 95% confidence interval (CI) exceeded 1. RORs were calculated using Excel for Microsoft 365 (Microsoft Corporation, Redmond, WA, USA). The signals of drug-drug interactions were evaluated as significant when the lower limits of the corresponding 95% CI in drug-drug interactions exceeded the higher limits of the corresponding 95% CI in monotherapy (29).
Chi-square test as univariate analysis and multiple logistic regression analysis were used to assess the risk of nephritis in ICPI monotherapy. Two-sided p-values less than 0.05 were considered significant. We conducted the multiple logistic regression analysis in ICPI dataset showing significant ADE signals of nephritis. Multiple logistic regression analysis in each ICPI dataset was performed using SPSS version 22.0 (SPSS Inc., Chicago, IL, USA).
Results
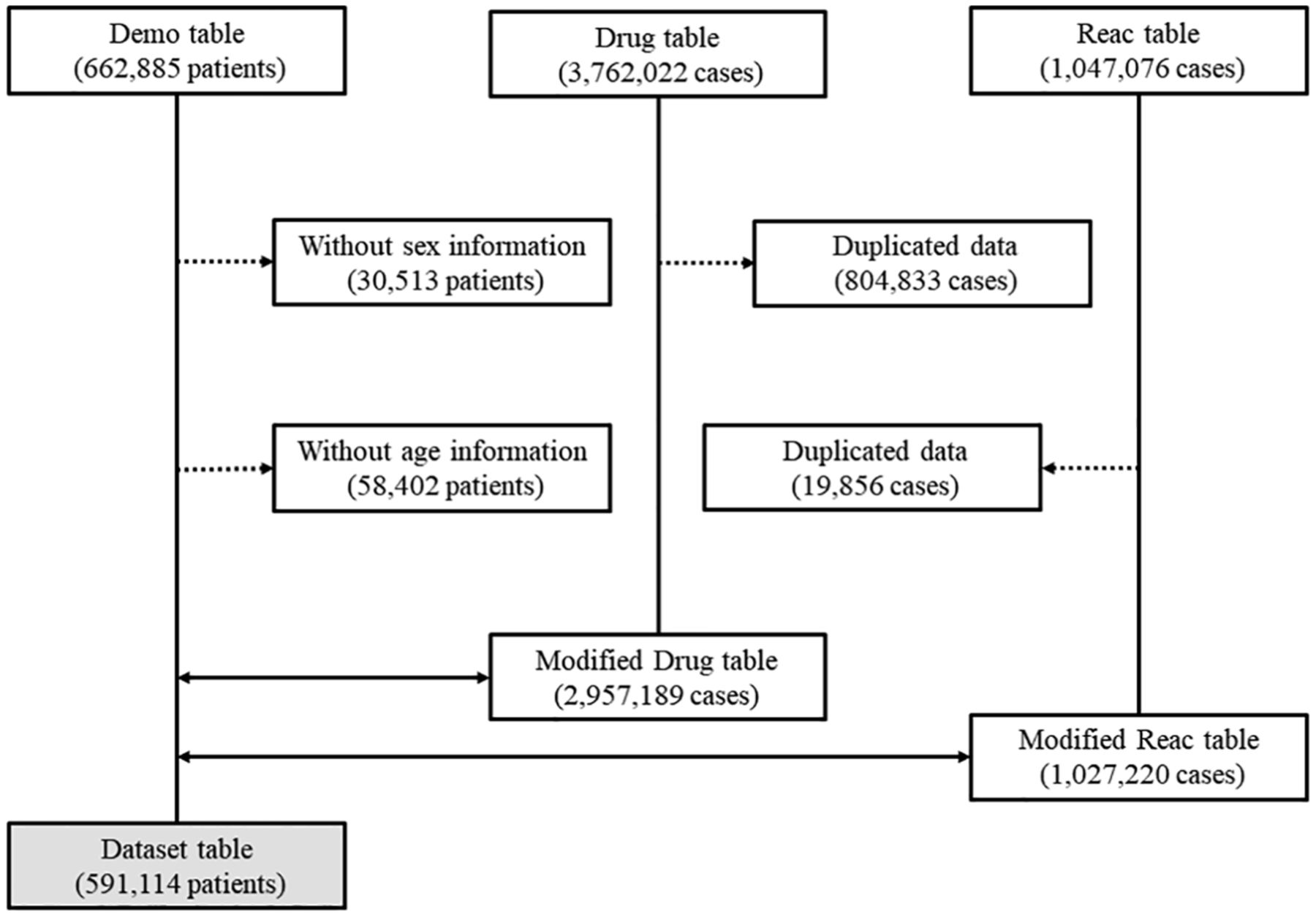
Patient characteristics and ROR of monotherapy. A total of 591,114 cases were included in the dataset (Figure 1). The numbers of side-effects associated with nivolumab, pembrolizumab, ipilimumab, atezolizumab, durvalumab, and avelumab were 9,116, 5,838, 2,831, 1,288, 1,054, and 48, respectively (Table III). In patients taking ICPI monotherapy, ADE signals of nephritis were detected in the atezolizumab, ipilimumab, durvalumab, nivolumab, and pembrolizumab groups. The use of atezolizumab [ROR (95% CI)=1.780 (1.102 to 2.874)], ipilimumab [ROR (95% CI)=2.454 (1.857 to 3.242)], nivolumab [ROR (95% CI)=2.091 (1.764 to 2.479)], and pembrolizumab [ROR (95% CI)=2.443 (2.008 to 2.973)] showed a statistically significant signal for nephritis (Table IV). Although the durvalumab group also showed ADE signals for nephritis, the signals were not statistically significant [ROR (95% CI)=0.252 (0.063 to 1.010)] (Table IV). Moreover, the avelumab group did not show any ADE signal for nephritis because of the small sample size.
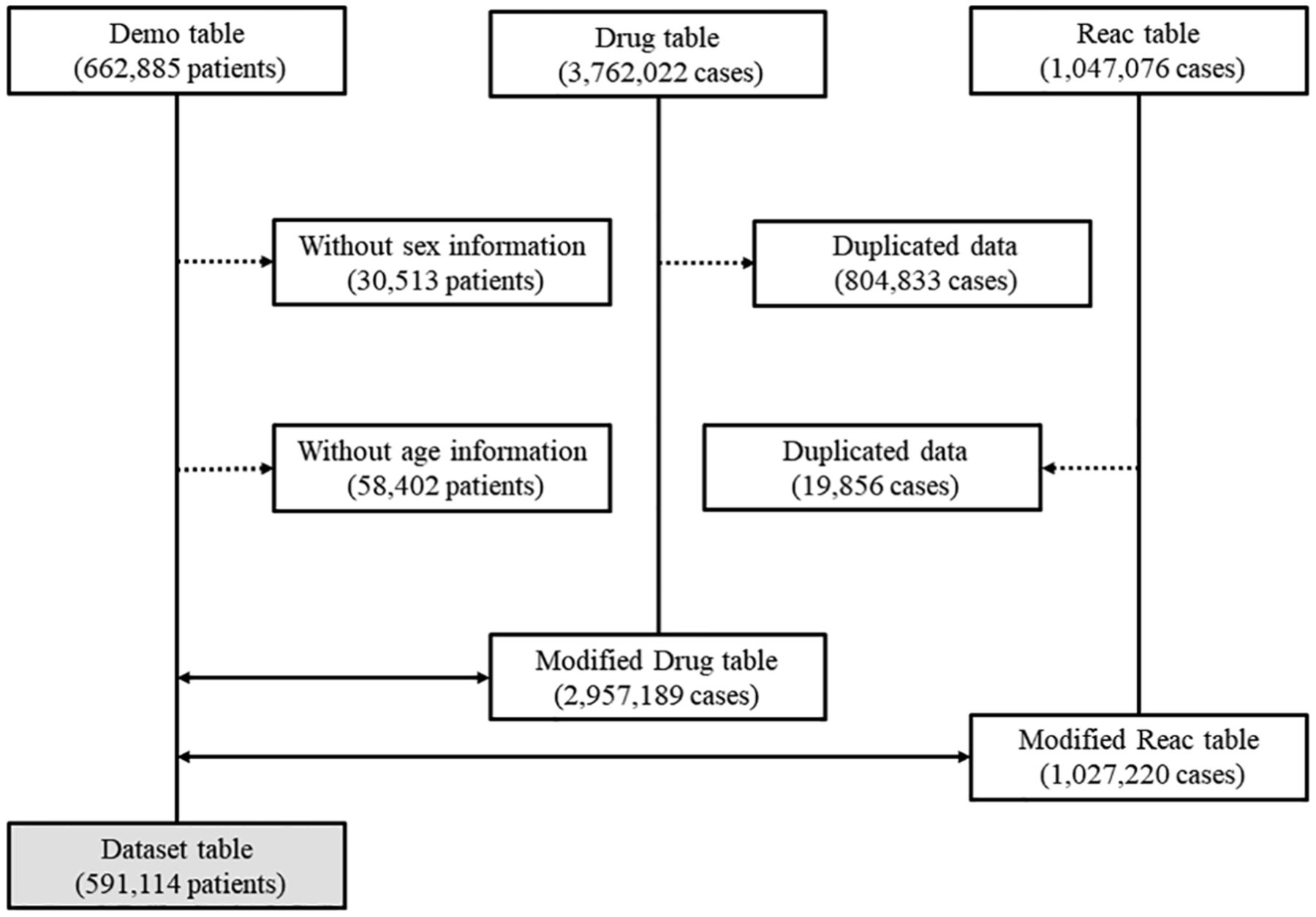
Flow diagram of the study. Dotted arrow and double arrow show data exclusion and combination, respectively.
Patient characteristics.
Crude reporting odds ratios for nephritis.
ADE signals of nephritis were detected in patients treated with PPIs. The use of esomeprazole [ROR (95% CI)=2.064 (1.326 to 3.214)], omeprazole [ROR (95% CI)=4.248 (3.209 to 5.622)], vonoprazan [ROR (95% CI)=1.829 (1.132 to 2.954)], rabeprazole [ROR (95% CI)=3.169 (2.263 to 4.437)], and lansoprazole [ROR (95% CI)=2.178 (1.705 to 2.783)] showed a statistically significant signal for nephritis (Table IV).
Drug-drug interaction signals. The signals of drug-drug interactions are shown in Table IV. Cases with concomitant use of atezolizumab and rabeprazole [ROR (95% CI)=66.43 (6.022 to 732.8)], ipilimumab and omeprazole [ROR (95% CI)=265.8 (24.09 to 2931)], ipilimumab and lansoprazole [ROR (95% CI)=29.53 (6.378 to 136.7)], nivolumab and esomeprazole [ROR (95% CI)=40.91 (13.33 to 125.5)], nivolumab and omeprazole [ROR (95% CI)=199.5 (56.28 to 707.3)], nivolumab and rabeprazole [ROR (95% CI)=114.0 (38.30 to 339.4)], nivolumab and lansoprazole [ROR (95% CI)=31.04 (13.67 to 70.71)], pembrolizumab and esomeprazole [ROR (95% CI)=33.23 (9.374 to 117.8)], and pembrolizumab and lansoprazole [ROR (95% CI)=15.63 (3.611 to 67.69)] had a significantly higher ROR than monotherapy cases.
Multiple logistic regression analysis. In univariate analysis, the frequency of nephritis was significantly high in male patients treated with ipilimumab (OR=3.844; 95%CI=1.634-9.042; p=0.001). There were no significant differences in male patients treated with atezolizumab (OR=3.139; 95% CI=0.714-13.794; p=0.110), nivolumab (OR=1.371; 95% CI=0.913-2.060; p=0.126), and pembrolizumab (OR=1.648; 95% CI=0.977-2.782; p=0.059). We also conducted multiple logistic regression analysis to assess the risk of ipilimumab-induced nephritis. The frequency of nephritis was significantly higher in male patients treated with ipilimumab (OR=3.798; 95% CI=1.614-8.938; p=0.002). Age over 70 years did not influence the frequency of nephritis (Table V).
Univariate and multivariate analysis for predictors of ICPI-induced nephritis.
Discussion
The estimated incidence of ICPI-induced nephritis is much lower than that of other irAEs (26). Therefore, understanding ICPI-induced nephritis was limited to small case series. To clearly identify the risk factors for ICPI-induced nephritis, Cortazar et al. (13) conducted a multicenter study involving 138 patients with ICPI-induced nephritis. This report identified low baseline eGFR and PPI use as independent risk factors of ICPI-induced nephritis. However, the PPIs that increase the risk of ICPI-induced nephritis were not identified in this study. In the present study, omeprazole increased the frequency of nephritis in patients treated with ipilimumab or nivolumab. Esomeprazole and lansomeprazole increased the frequency of nivolumab and pembrolizumab-induced nephritis. Furthermore, the frequency of ipilimumab-induced nephritis increased in male patients.
Hypomagnesemia, AKI, AIN, and CKD were reported as adverse events associated with PPI use (30, 31). The risk of hospital admission was elevated within 120 days of PPI exposure (32). In addition, PPI use was associated with increasing mortality due to cardiovascular disease, CKD, and upper gastrointestinal cancer (33). These previous reports suggested that medical practitioners should consider the potential benefits and risks of PPIs. Based on kidney biopsy results, the frequency of AIN with severe inflammatory cell infiltration was higher in ICPI-induced nephritis than in other types of renal injury (14). Hence, these reports suggest that cell-mediated immunity is associated with nephritis. Although the underlying mechanism of PPI-induced nephritis is unclear, PPI-induced nephritis showed cellular infiltrates with lymphocytes and occasional eosinophils in the renal interstitium (20, 22). Therefore, concomitant use of ICPI and PPI might develop cell-mediated immunity associated with AIN. In the present study, omeprazole and lansoprazole showed high risk of nephritis induction in the cases with or without ICPI. Although the most of omeprazole-induced nephritis are recognized as interstitial damage (17, 30), the underlying mechanism is unclear. Organic cation transporters (OCTs) uptake PPIs to renal tubular cells (34). Since the affinity for OCTs and accumulation in renal tubular cells are higher for omeprazole or lansoprazole than that for rabeprazole (34), omeprazole, and lansoprazole have more potential in inducing AIN compared to other PPIs.
Male gender showed an increasing tendency towards risk of ICPI-induced nephritis (13). Although the mechanism of nephritis in male patients treated with ICPIs was unclear, our results supported this previous report. Since the frequency of irAEs is higher in female patients than that in male patients (35-37), ICPI-induced nephritis might have different mechanism to that of other irAEs. Since ipilimumab has an immunoglobulin G1 (IgG1) structure, it might lead to higher activation of complement and other immune system factors than the rest of the IgG subtypes (38-40). Therefore, our results suggested that male patients or patients with concomitant use of ICPIs and PPIs (excluded vonoprazan) should be monitored for renal function after chemotherapy.
The present study has certain limitations. First, the ADE signal of avelumab-induced nephritis was either weak or not detected because of the small sample size. Nivolumab was approved in Japan in 2014, whereas ipilimumab, pembrolizumab, avelumab, atezolizumab, and durvalumab were approved in 2016, 2015, 2017, 2018, and 2018, respectively. Therefore, the number of ADE reports for nivolumab is greater than those for the other ICPIs. Second, as a large spontaneous reporting system, the JADER database has various biases including under- or over-reporting and confounders caused by comorbidities (28, 41-45). Third, the number of nephritis event was small in concomitant use of ICPI and PPI. Although multiple logistic regression analysis could be conducted in monotherapy data set, this analysis was not applied for concomitant use data set because of lack statistical power.
The most common trigger of AIN is the drug used (46), therefore the identification of the types of drug is important in determining a preventive strategy. Although our results provide new insights of ICPI- and PPI-induced nephritis, further basic and clinical studies are required to elucidate the mechanisms of action.
Acknowledgements
The Authors would like to thank Editage (https://www.editage.com/) for editing and reviewing this manuscript for English language.
Footnotes
↵* These Authors contributed equally to this study.
Authors’ Contributions
KK, TM, YI, and NT designed this study. KK and TK carried out the survey of the JADER database. KK, TM, TK, and MH performed the statistical analyses. KK, TM, YI, KT, SY, and NT drafted the manuscript. All Authors approved the final manuscript.
This article is freely accessible online.
Conflicts of Interest
The Authors report no conflicts of interest regarding this work.
- Received May 13, 2021.
- Revision received June 7, 2021.
- Accepted June 14, 2021.
- Copyright © 2021 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}