


Abstract
Background/Aim: Kidney cancers account for about 2% of human malignancies. In recent decades, the incidence of this cancer type has gradually increased, mainly due to advances in imaging. The metastatic potential of these cancers is significant: a quarter of patients will immediately present with metastases and more than one third of patients treated with nephrectomy for a localized disease will develop metastases during their course. In total, more than half of patients will suffer from the consequences of metastasis. The median survival at this stage is only thirteen months, so the therapeutic challenge is immense. Case Report: The present case report describes a case of left renal clear cell carcinoma with brain, lung, right adrenal, bone and lymph node metastases in a 55-year-old male. The patient received only one line of anticancer treatment with sunitinib, which could not be continued due to haemorrhagic manifestations in brain metastases. The treatment was changed with immunotherapy which showed its effect even if it was stopped due to the patient wishes in the context of the COVID-19 epidemic. Conclusion: Immunotherapy opens the doors to a new era in treatment of metastatic renal cancer and shows efficiency even after it has been stopped.
Kidney cancers account for about 2% of human malignancies. In recent decades, the incidence of this cancer type has gradually increased, mainly due to advances in imaging and its vast application of investigations (1). However, the annual mortality rate remains relatively stable, mainly because tumors detected during these radiological examinations are successfully treated with nephrectomy. Kidney cancer affects more men than women (1.5/1 ratio), it is diagnosed mainly between 60 and 70 years but can occur at any age. The main risk factors are smoking and obesity. The metastatic potential of these cancers is significant: one quarter of patients will present immediately with metastases, more than a third of patients treated with nephrectomy for a localized disease will develop metastases during their course. In total, more than half of patients will suffer from the consequences of the metastatic process. The median survival at this stage is only thirteen months, so the therapeutic challenge is immense.
Histologically, there are three main types of renal cell carcinoma: clear cell, papillary, and chromophobic. Over the past ten years, it has been clearly established that these different histological aspects correspond to specific genetic abnormalities in both sporadic and hereditary forms of kidney cancer. In this paper, we focus on clear cell cancer, by far the most common (approximately 80%), and on which therapeutic development has focused.
The major cellular components of a kidney cancer are the tumor cells, blood vessel cells, and lymphocytes infiltrating the tumor. Strategies for destroying the tumor cells (conventional chemotherapy), or endothelial cells and blood vessel pericytes (antiangiogenic treatment) can be considered in order to limit nutritional and oxygen supply, or to stimulate lymphocytes so that they can exert their cytolytic effects. Due to the intrinsic chemo-resistance of kidney cancer tumor cells, focus of immunotherapy has been examined since several decades (2).
Immunotherapy in renal cancer. There are several observations suggesting that the immune system may, under certain conditions, control the growth of kidney cancers. For example, the rare cases of regression of metastases, observed spontaneously or after nephrectomy, or the sharp increased risk of developing kidney cancer with immunosuppression, for example after kidney transplantation (3). It was, therefore, logical to attempt to stimulate this natural property for therapeutic purposes. Two cytokines, interferon-α and interleukin-2, were particularly tested for this purpose. The rate of objective responses obtained with these cytokines is modest, between 5 and 20%. The potential benefit on survival is highly questionable. For interferon-a, although a randomized study (4) showed a slight benefit over placebo, 30 years of use of this cytokine demonstrate that this benefit is marginal and probably limited to patients with a good prognosis (2). However, one should note that interferon-a was the only drug reimbursed in Switzerland until 2006 for the treatment of metastatic kidney cancer. The potential of interleukin-2, a true “doping” of the immune system, is quite paradoxical. Indeed, randomized studies have not shown a survival advantage over interferon or placebo, but this treatment is currently the only one with which long-term complete remissions can be expected (1% of cases).
The use of these cytokines is limited by their toxicity. In addition, it is now established that the growth of a cancer is accompanied by development of mechanisms that allow the tumor cell to escape control of the immune system. Rather than trying to stimulate a “sleeping or defective” immune system with cytokines, the idea emerged to try to replace it. Thanks to the expertise gained in the treatment of malignant hematological diseases, it was attractive to try and perform bone marrow allografts for the treatment of kidney cancer. Indeed, induction chemotherapy is used only for immunosuppressive purposes, allowing the transplantation and establishment of a new immune system. The antitumor potential of T cells included in the spinal graft has been demonstrated by hematologists who routinely use this property in the treatment of certain forms of leukemias. Extrapolation of this procedure is in full swing in the treatment of metastatic kidney cancer. Several research teams reported impressive response rates, close to or greater than 50%. However, it is important to emphasize the limitations and constraints of this therapeutic modality (5).
Treatments using immunotherapy like nivolumab, a humanized antibody targeting programmed cell death protein 1 (PD1), achieve durable effects in approximately 15% of patients with metastatic renal cell carcinoma (mRCC) (6-9). Choueiri et al. (10) reported immunomodulatory activity of nivolumab in biopsied mRCC tissues, which were acquired before and in the course of treatment with nivolumab. The combination of nivolumab and ipilimumab, anti CTLA-4 in the first-line treatment demonstrated clinical efficacy in metastatic renal cancer patients, leading to regulatory approval of the combination for patients with intermediate- or poor-risk disease in April 2018.
Case Report
The present case was a 55-year-old male with left renal clear cell carcinoma operated in June 2015. Left radical nephrectomy was performed and the pathological staging was pT3pN0. In October 2019 the follow-up CT scan showed disease progression with right adrenal metastasis which was operated in October 2018. Unfortunately, follow-up CT scan 3 months later in January 2019 showed multiple lung nodules and bone metastasis. We stared first-line treatment with sunitinib and after one week of treatment the patients presented with seizures.
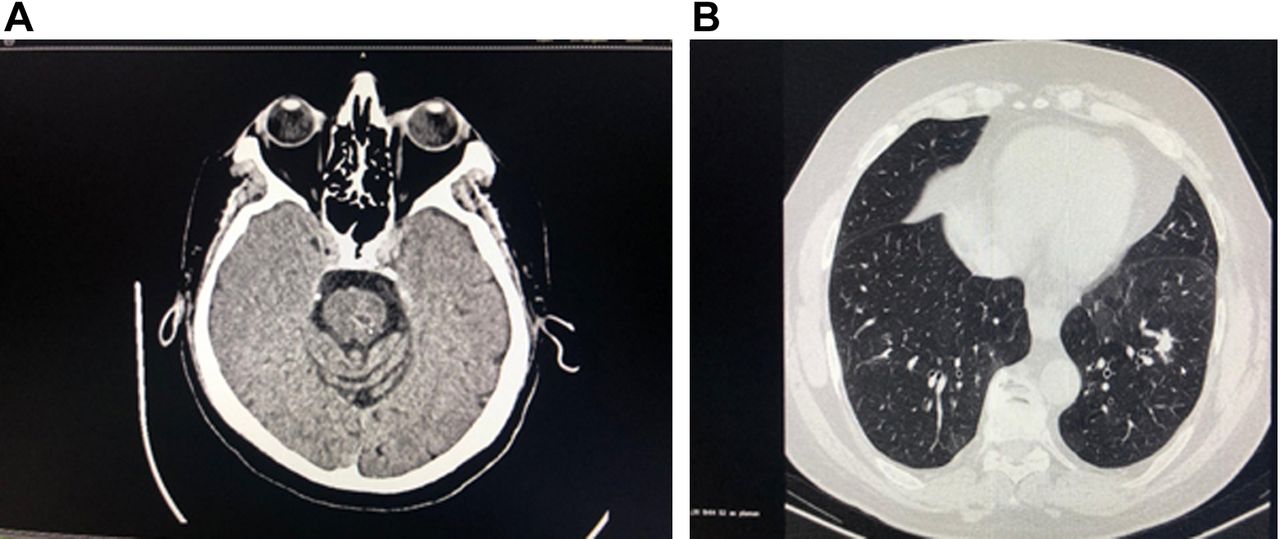
The brain CT scan showed secondary cerebral expansive infra and supratentorial hemorrhagic lesions (Figure 1). We stared the whole-brain radiotherapy and after the stabilization of the lesion in march 2019 we changed the treatment with nivolumab 240 mg, one administration at 14 days. He tolerated the treatment extremely well.

Basal CT brain scan shows multiple brain metastases.
According to the evaluation protocol, 8-14 weeks after the start of administration it was shown that regression was achieved on both brain and lung lesions, bone and mediastinal lymphadenopathy (Figure 2).

Basal CT thoracic scan shows multiple lung metastases.
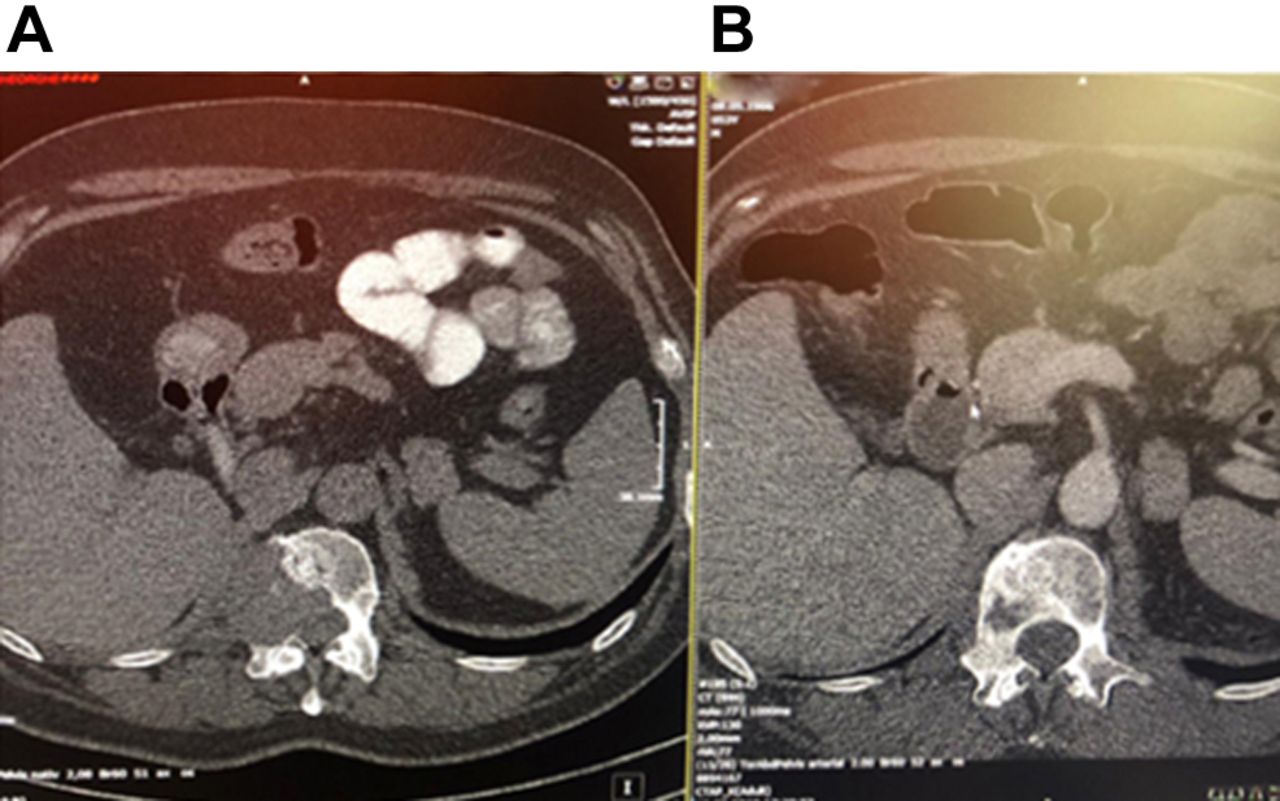
Very interesting was the fact that combination of nivolumab and the osteoclast inhibitor induced restoration of bone structure, and the patient presenting a secondary osteolytic lesion in the right L1 vertebral body measuring 43/42 mm with right T12-L1 intraforaminal extension and in the canal spinal cord with mass effect on the medullary cord. The results are shown in Figure 3A and B.

Basal CT scan shows bone metastases (A), and radiological response after twelve cycles of immunotherapy (B).
He clinically responded well to the treatment with minimal side-effects. After 12 cycles of nivolumab therapy, a repeat CT scan was obtained. The results showed a decrease of the lesion at the anterior aspect. About 5 months later, he presented to the hospital complaining of fatigue, forgetfulness and symptomatic bradycardia.
At this time, further laboratory investigations revealed a TSH was 58.4 mU/l (normal=0.27-4.2) with free T4 of 0.54 (normal=5.10-14.10). The patient was started on specific treatment which resulted to clinical improvement. Nivolumab had to be stopped due to immune-mediated side-effects.
The patient wanted to delay treatment both due to the side-effects manifested in the thyroid gland and due to the Covid-19 pandemic.
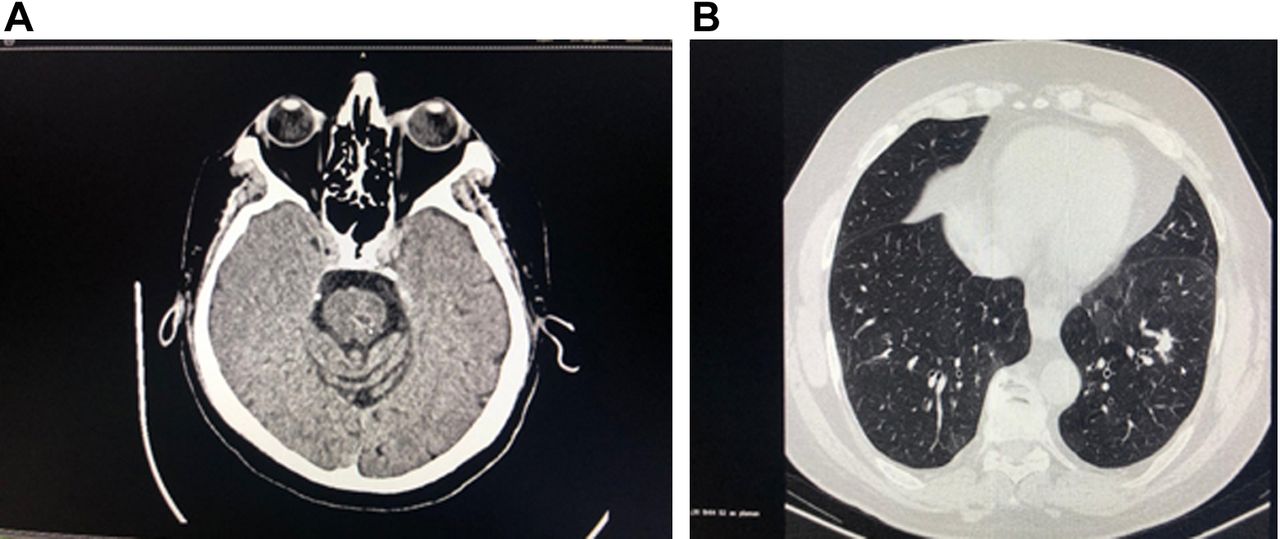
As shown in Figure 4A and B, at 6-month intervals, the patient performed a CT evaluation that showed that the target lesions remained stationary, without the appearance of new lesions one year after stopping treatment. At one year after he stopped immunotherapy the patient is asymptomatic, and with good biological test results. Follow-up CT scans at one year showed a stable disease according to (RECIST) criteria version 1.1.
CT brain (A) and thoracic (B) shows stable disease after one year immunotherapy has been stopped.
Discussion
Renal cell carcinoma is known to be a chemo-resistant malignancy, thus conventional chemotherapy is currently not recommended for the management of metastatic cases. The most-used VEGF inhibitors, sunitinib is the standard of care in the first line metastatic renal cancer, and are currently recommended by National Comprehensive Cancer Network (NCCN) guidelines (11).
Until 2005, immunotherapies such as high-dose interleukin (IL-2) and interferon alpha (INF-a) were the only treatments available. Fyfe et al. published the results of a study that included 225 patients with renal cancer treated with high-dose IL-2 and found an overall objective response rate of 14%, with 5% showing a complete response and 9% showing partial responses.
Nivolumab is a checkpoint inhibitor, a humanized anti-PD1 antibody. PD-1 is a receptor found on the surface of T lymphocytes and binding to PD-L1/2 ligands results in anergy. This regulation, which makes it possible (under physiological conditions) to avoid autoimmune reactions, constitutes an avoidance mechanism for tumor cells that express PD-L1/2 on their surfaces (12). Nivolumab recently demonstrated a survival benefit in second-line treatment, in a phase III study published in 2015 (13, 14). Overall survival was 25 months in the nivolumab arm versus 19.6 months in the control arm treated with everolimus, this in a cohort comprising only clear cell histologies. It is important to note the lack of benefit in terms of PFS between for the two groups. Prolonged survival was observed in patients treated with nivolumab, compared to everolimus. The study population consisted mainly of patients at favorable/intermediate risk according to the Memorial Sloan-Kettering Cancer Center (MSKCC) score. A subgroup analysis showed that this benefit is also present in high-risk patients. Adverse effects of nivolumab reported in this study were fatigue (33%), pruritus (14%), as well as digestive disturbances in the form of nausea (14%) and diarrhea (12%) (15, 16). Cases of drug-induced pneumonia have been reported. Its overall tolerance was better than that of patients treated with everolimus. Grade 3-4 adverse reactions were almost half the frequency and the quality of life significantly better in the nivolumab arm (17). There is a risk of hypothyroidism, hypophysitis, adrenal insufficiency and skin reactions with this type of immunotherapy. Autoimmune hepatitis, sometimes severe, has also been reported. These side-effects usually occur eight to 12 weeks after starting treatment, but sometimes later. Close clinical and laboratory monitoring of patients on immunotherapy is necessary.
CTLA4 inhibitors, the main representative of which is ipilimumab, are currently a standard in the treatment of metastatic melanoma. Data from a phase II study demonstrated partial response in patients suffering from metastatic renal cancer. In addition to the above-mentioned side-effects, which are more frequent, there is a greater risk of autologous colitis. The identification of these toxicities and their effective management by administration of systemic immunosuppressive therapies provide a favorable outcome in the vast majority of cases. The Checkmate 214 study, which is currently undergoing recruitment, will evaluate the efficacy of nivolumab/ipilimumab combination as a first-line treatment for metastatic renal cancer compared to sunitinib. The final results of this study will be available in 2019 (18). Data concerning its safety nonetheless reveal a grade 3-4 toxicity rate of around 30%, a rate comparable to that observed in the study of this same combination in patients with metastatic melanoma. The combination of anti-PDL1/PD1 with bevacizumab or axitinib, compared to sunitinib, is currently in phase III studies. Their results are also more than expected.
In a multicentre, open-label, phase 3, randomised controlled trial, patients with a component of clear cell or sarcomatoid histology and who were previously untreated and were randomly assigned 1:1 to either atezolizumab 1,200 mg plus bevacizumab 15 mg/kg intravenously once every 3 weeks or sunitinib 50 mg orally once daily for 4 weeks on, 2 weeks off, atezolizumab plus bevacizumab prolonged progression-free survival versus sunitinib in patients with metastatic renal cell carcinoma and showed a favourable safety profile (19).
The combination of nivolumab plus ipilimumab has demonstrated efficacy in first-line treatment of metastatic renal cancer patients with IMDC intermediate- or poor-risk disease and will become the new treatment standard in this group of patients.
Radiation therapy is a very effective way of treatment used for the curative and palliative management of almost all types of cancer. It is often combined with other treatment modalities, including surgery, recent immunotherapy chemotherapy, to maximize the chance of controlling the disease. Combination of CRT with immunotherapy in renal cancer must be evaluated. Radiotherapy has pro-immunogenic effects on the tumour microenvironment, initiating innate and adaptive immunity. The abscopal effect in patients treated with immunotherapy and radiotherapy showed response to radiotherapy in other distant sites after local radiotherapy administration (20).
Conclusion
At a time when the therapeutic arsenal continues to be enriched with new targeted agents, hope once again lies in immunotherapy. This approach, thanks to the recently approved nivolumab, opens the doors to a new era in the treatment of metastatic renal cancer. It brings the need to change our way of evaluating its effectiveness, given that PFS is a poor representative of the overall survival of treated patients. During this difficult period, due to the Covid-19 pandemic, it is important to know that the effect of delaying the administration or stopping immunotherapy does not lead to progression of the disease.
Footnotes
Authors’ Contributions
BH was responsible writing of the manuscript. AZ, BH, CM and NB were responsible for reviewing and editing of the manuscript. AZ, BH and NB, CM, CD made substantial contributions to the conception or design of the work. RA were responsible for the critically reviewed the manuscript. All Authors read and approved the final manuscript.
This article is freely accessible online.
Conflicts of Interest
The Authors declare that they have no competing interests in relation to this study.
- Received February 5, 2021.
- Revision received February 20, 2021.
- Accepted March 1, 2021.
- Copyright© 2021, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.