


Abstract
Sunitinib is listed as first-line therapy for non clear-cell renal cell carcinoma (RCC) in several guidelines. However, in the era of immunotherapy, there is an urgent need for updated evidence for the treatment of metastatic non clear-cell RCC. Herein, we present three cases of patients with type 2 papillary RCC who were effectively treated with cabozantinib. The first case was a 48-year-old woman who underwent radical nephrectomy (pT3aN0M0). The tumor relapsed in the retroperitoneum 3 months postoperatively and was unresponsive to first-line nivolumab plus ipilimumab (NI). After the use of cabozantinib, the tumors drastically shrunk in 2 weeks, and complete response was achieved 3 months later. The second case was a 55-year-old man who underwent radical nephrectomy (pT3aN2M1). Metastatic lesions continued to grow with first-line NI, and cabozantinib was used as the second-line therapy. All metastatic lesions had shrunk by 50% after 4 months. The third case was a 36-year-old man with multiple tumors in the left solitary kidney and iliopsoas muscle metastasis. First-line therapy with NI was ineffective; subsequently, second-line axitinib was used for 5 months, and the disease was identified as progressive. Cabozantinib was started as third-line therapy. Multiple tumors shrunk in 2 weeks. There is little evidence concerning the treatment of papillary RCC. We experienced low efficacy of NI for first-line treatment of papillary RCC for three patients who were subsequently effectively treated with cabozantinib. Cabozantinib inhibits multiple tyrosine kinase receptors, which may suppress aggressive tumor progression of type 2 papillary RCC. Cabozantinib or combination with immuno-oncological drugs may be a promising treatment option for papillary RCC.
Cabozantinib was shown to confer longer progression-free (PFS) and overall (OS) survival over everolimus as second-line treatment and longer PFS over sunitinib as initial treatment in patients with metastatic clear-cell renal cell carcinoma (ccRCC) (1, 2). However, the efficacy of cabozantinib in patients with papillary RCC (pRCC) remains unknown. Herein, we present three cases of patients with pRCC who were highly responsive to cabozantinib following ineffective initial therapy with nivolumab and ipilimumab.
Case Reports
Retrospective study’s protocol of this report was approved by the appropriate Institutional Review Boards (2020-0009). Pathological diagnoses were made according to the 2016 World Health Organization classification (3). The best response during NI treatment was recorded with reference to the Response Evaluation Criteria in Solid Tumors (RECIST, version 1.1) (4).
The first case was a 48-year-old female patient with no medical history who presented with left lumbar pain, and a tumor was found in the left kidney. A contrast-enhanced computed tomographic scan showed a 13-cm left kidney mass with renal venous thrombus extension, with no regional lymph node involvement or metastatic disease. Open radical nephrectomy revealed pathological findings of type 2 pRCC, Fuhrman nuclear grade 2, and pT3aN0M0. Three months postoperatively, the tumor relapsed in the left retroperitoneum (5 mm) and inguinal lymph node (17 mm). Nivolumab plus ipilimumab therapy was started as the initial therapy for International Metastatic Renal Cell Carcinoma Database Consortium (IMDC) intermediate risk disease (5). However, unresponsive to four cycles of nivolumab plus ipilimumab, the relapsed tumors enlarged in the retroperitoneum (38 mm) and inguinal lymph node (25 mm). As immune-related adverse events, grade 1 myalgia in the extremities was observed, which was relieved spontaneously. Cabozantinib (60 mg per day) was then started as second-line therapy. Two weeks later, the patient presented with a fever of 40°C without any other symptom, and computed tomography revealed drastic shrinkage of the relapsed tumors (retroperitoneum: 10 mm; inguinal lymph node: 7 mm) (Figure 1). Complete response was achieved 3.5 months later. Temporarily, drug interruption was necessary, and the dose was reduced to 20 mg due to adverse events, including grade 4 neutropenia, grade 2 hypothyroidism, alopecia, and palmar–plantar erythrodysesthesia.
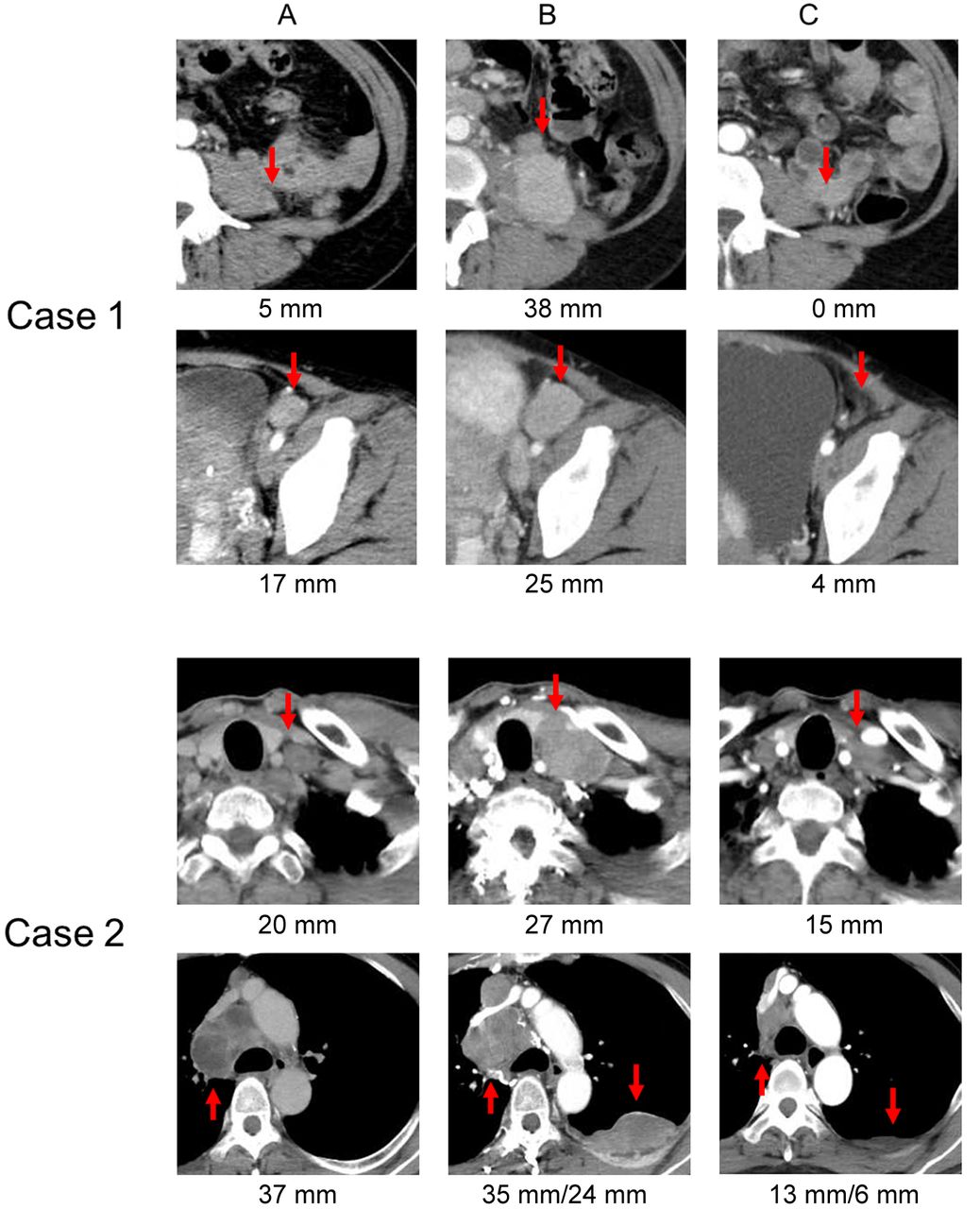
Tumor responses from the commencement of the first- to second-line treatment in two cases (contrast-enhanced computed tomography). Case 1, upper panel: metastasis in iliopsoas muscle; Iower panel: metastasis in inguinal lymph node. Case 2, upper panel: metastasis in the cervical lymph node; lower panel: metastasis in the mediastinal lymph node and in the pleura. A: Metastatic status at the start of nivolumab and ipilimumab therapy. B: Metastatic status at the evaluation of progressive disease with nivolumab and ipilimumab. C: Metastatic status showing the efficacy of cabozantinib after 3 months of therapy.
The second case was a 55-year-old male patient without past medical history who presented with left back pain and gross hematuria. Contrast-enhanced computed tomography showed a 14-cm left renal tumor with metastases of the mediastinal lymph nodes and vertebral bone that compressed his spinal cord. He underwent emergency decompressive surgery and radical nephrectomy. Pathological findings were type 2 pRCC, Fuhrman nuclear grade 2, and pT3aN2M1. Immediately after surgery, nivolumab and ipilimumab therapy was initiated for IMDC intermediate risk disease. The best tumor response was stable disease at 5 months. Radiation was added for new lesions, including vertebral and pelvic metastases. However, metastatic lesions continued to grow for another 7.2 months. Cabozantinib (60 mg per day) was then started as second-line therapy. All target lesions in the mediastinal lymph node, lung, and pleural metastases had shrunk by 50% after 4 months (Figure 1). He presented with grade 2 palmar-plantar erythrodysesthesia, hypothyroidism, and hypertension, which did not require drug interruption or dose reduction.
The third case was a 36-year-old male patient who had a past history of testicular cancer (seminoma). He underwent right radical nephrectomy due to right RCC at the age of 28 years (pRCC, pT2aN0M0, Fuhrman nuclear grade 4). Additionally, a 2.7-cm left renal tumor appeared at the age of 35 years, and he underwent open partial nephrectomy. However, multiple recurrent tumors in the left kidney (5.5-6.2 cm) and iliopsoas muscle (2.3 cm) were found 9 months later. The tumors were unresponsive to initial therapy with nivolumab and ipilimumab. Subsequently, axitinib was used for 5 months, and the best tumor response was stable disease. Cabozantinib (60 mg per day) was then used as third-line therapy, and the tumor drastically shrank in 2 weeks, with the patient having a fever of 39°C (Table I). Grade 2 diarrhea was identified as an adverse event in these 2 weeks. However, drug interruption or dose reduction was not necessary.
Individual clinical profiles in patients with papillary renal cell carcinoma treated with nivolumab plus ipilimumab as first-line therapy.
Discussion
Currently, sunitinib is listed as first-line therapy for non-ccRCC in the National Comprehensive Cancer Network guidelines (6). However, due to their aggressive nature and poor response to targeted agents, type 2 pRCC subtypes have been reported to have a worse prognosis compared with ccRCC (7). Nivolumab and ipilimumab therapy was reported to lead to longer PFS and OS compared with sunitinib in patients with IMDC intermediate- and poor-risk ccRCC in CheckMate 214 (8). All our patients were young and did not have serious comorbidities. Therefore, we chose nivolumab plus ipilimumab and expected a high rate of complete response for type 2 pRCC. Unfortunately, all patients had progressive disease on this first-line nivolumab and ipilimumab therapy. Our recent report also showed modest efficacy of nivolumab and ipilimumab therapy in cases of pRCC; one out of seven patients achieved partial response, and five patients had progressive disease (9). Therefore, another treatment option for pRCC is needed. Here, we reported three cases that were effectively treated with second- or third-line therapy using cabozantinib after failure of first-line immunotherapy.
Cabozantinib inhibits multiple tyrosine kinase receptors associated with tumor progression, including vascular endothelial growth factor, mesenchymal–epithelial transition (MET), rearranged during transfection, and anexelekto (RET) (10). Martinez et al. reported the efficacy of cabozantinib in non-ccRCC in a multicenter retrospective analysis and concluded that cabozantinib was effective in controlling non-ccRCC (11). To the best of our knowledge, this is the first report of the efficacy of cabozantinib after nivolumab and ipilimumab in cases of pRCC. Choueiri et al. reported the efficacy of savolitinib (a selective MET inhibitor) against MET-driven pRCC in a phase III trial. The PFS, objective response rate, and OS were greater with savolitinib compared with those with sunitinib, and they concluded that a combination therapy with immuno-oncological drugs was promising (12). The efficacy of cabozantinib in our three cases may be due to its ability to inhibit many receptors. Furthermore, there is a possibility of a synergistic effect of cabozantinib with first-line immuno-oncological drugs; the ongoing clinical trial on nivolumab and cabozantinib (NCT03141177) may show this to be a promising regimen for pRCC. There are few reports about pRCC; however, cabozantinib or a combination of cabozantinib and immunooncological drugs may be a hopeful treatment option for pRCC. Further analysis with a larger number of cases is required to make any conclusion.
In summary, we reported, for the first time, three cases pRCC which were effectively treated with cabozantinib as second- or third-line therapy. The favorable result poses this as a hopeful treatment option for pRCC.
Footnotes
Authors’ Contributions
Hidekazu Tachibana: Acquision of data, analysis and interpretation of data, drafting of the manuscript. Yudai Ishiyama: Acquisition of data. Maki Yoshino: Acquision of data.
Kaori Yamashita: Acquision of data. Daisuke Toki: Supervision. Tsunenori Kondo: Concept and design, analysis and interpretation of data, critical revision of the article for important intellectual content, and supervision.
This article is freely accessible online.
Conflicts of Interest
Tsunenori Kondo received honoraria from Pfizer, Novartis, and Ono Pharmaceutical. All other Authors have no conflict of interest to declare.
- Received January 20, 2021.
- Revision received February 10, 2021.
- Accepted February 14, 2021.
- Copyright© 2021, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}