


Abstract
Background/Aim: Different manual therapy techniques and conservative therapy have been used separately for alleviation of pain and improvement of physical function in patients with knee osteoarthritis (KOA). However, no study has reported the effect of combination of these treatment modalities in the management of KOA. Our aim was to test the feasibility of the study design and to compare the effect of end-range Maitland mobilization to conservative therapy in KOA. Patients and Methods: Fifteen patients (conservative therapy group: CG) received conservative therapy alone, fifteen patients (Maitland plus conservative therapy group: M+CG) received additionally end-range Maitland mobilization during the 3-week study period. Outcomes were pain intensity, measured with visual analogue scale (VAS) in general and during functional activities, passive range of motion (PROM) and peak muscle force during knee flexion and extension, Timed Up and Go test and 6-Minute Walk Test (6MWT). Results: All outcomes improved significantly in both groups. Magnitude of changes was significantly greater in M+CG compared to CG regarding all VAS pain scores, flexion PROM of both knees, right hamstring peak muscle force and 6MWT. Conclusion: With few modifications, this study design seems feasible for the comparison of end-range Maitland mobilization with conservative therapy in KOA. Moreover, end-range Maitland mobilization in addition to conservative therapy appeared more effective in relief of pain and improvement of functional status than conservative therapy alone in KOA.
Knee osteoarthritis (KOA) is a musculoskeletal condition affecting mostly older people. Main symptoms in KOA are pain, stiffness, crepitation, instability, loss of range of motion and limited physical activity (1). The prevalence of KOA has been reported appearing in 13% and 10% of women and men, respectively, aged 60 years or above (2).
Different international guidelines highly recommend conservative therapy including land- and water-based exercises, electrotherapy (3, 4) and medical bath (4) for the management of KOA. The effectiveness of these interventions has been widely demonstrated in KOA (5-13); however, applying medical bath depends mainly on geographical accessibility. Nevertheless, in a possibility of using medical bath, just as in Hungary, the effectiveness on alleviation of pain and improvement of physical function has been reported in KOA (13, 14). Additionally, as 3-week inpatient rehabilitation care has been reported to be more efficient in the treatment of symptoms and functional deficits in KOA compared to outpatient rehabilitation (15), applying land- and water-based exercises, electrotherapy and medical bath combined in 3-week inpatient rehabilitation care could produce positive effects in the management of KOA.
Maitland manual therapy out of different manual therapies could be a useful adjunct intervention (3) in the management of symptoms in KOA. Maitland manual therapy applies both accessory and physiological technique and varies the performed Grades from I to IV. Grade I, applied with accessory technique, and Grade II, applied with accessory or physiological technique, are used in pain-free position for alleviating severe pain only. Grades III and IV are applied with both accessory or physiological technique and are performed in end-range in order to restore full range of motion (16). Positive effects of Maitland manual therapy have been proven in KOA (17, 18); however, knee joints were neither mobilized in end-range positions, nor managed in addition with conservative therapy in those studies. Previous studies showed that land-based exercises combined with different manual therapies are more effective than land-based exercises alone in KOA (19, 20). Therefore, the combination of end-range Maitland mobilization with these interventions might also improve the functional status of the arthritic knee. Although all end-range mobilizations of the different manual therapies provide the same similar stretching effect, only end-range Maitland mobilization applies two Grades in resistance without active movement of the patient. Thus, the mobilization-induced hypoalgesic and functional effects observed in the management of other joints’ condition (21-23) could provide superior effects in addition to conservative therapy in KOA as well.
Therefore, the aim of this pilot study was to test the feasibility of the study design and to investigate the effect of end-range Maitland mobilization in combination with conservative therapy in a 3-week inpatient rehabilitation care on alleviation of pain, compared to conservative therapy alone, in KOA patients. Furthermore, different function-related measures were also evaluated regarding potential effects.
Patients and Methods
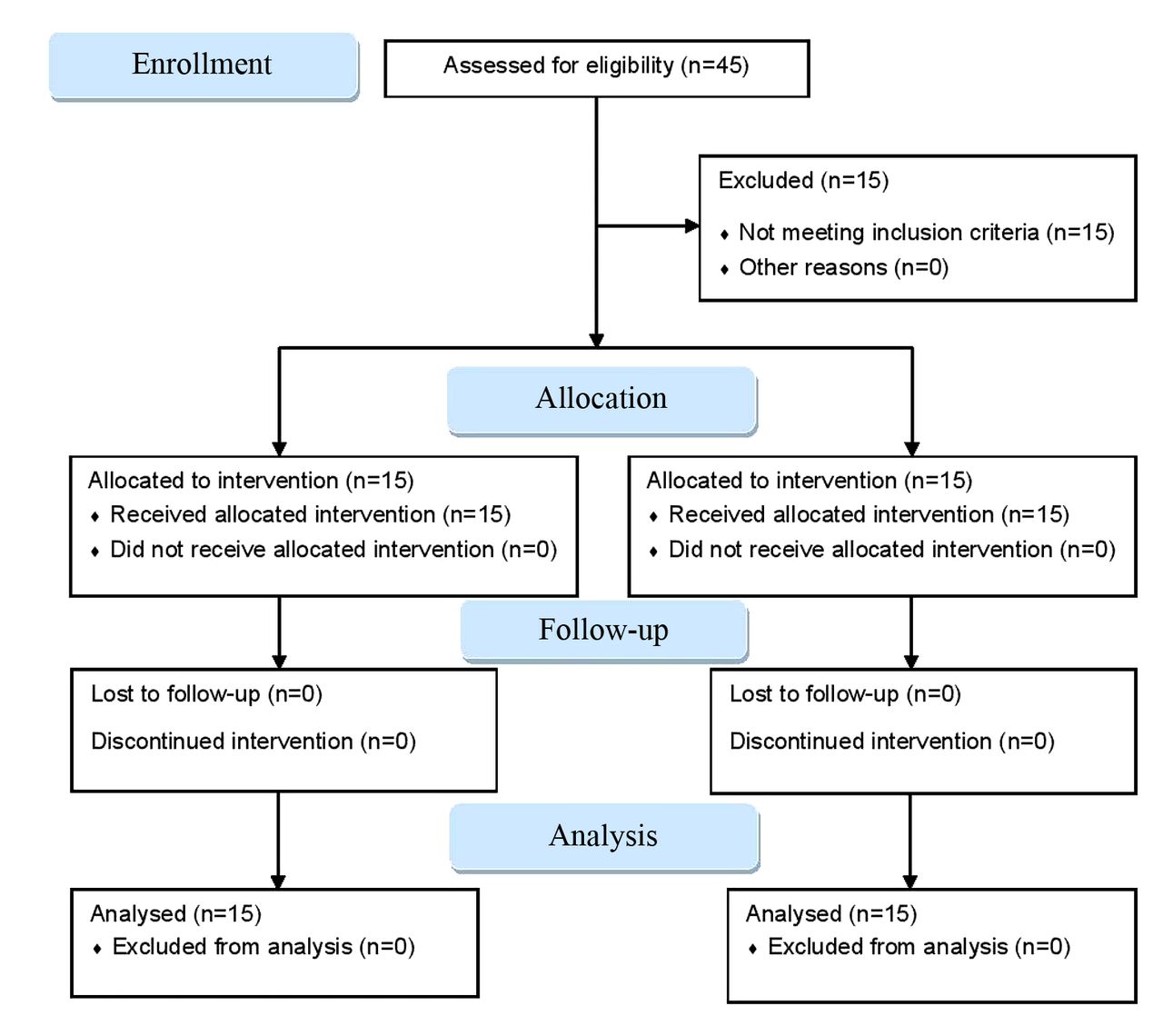
Study design. Assessor-blinded, non-randomized interventional trial was conducted between March and September 2018. All patients participated in the trial were admitted for 3-week inpatient rehabilitation care to Harkány Thermal Rehabilitation Centre between June 2017 and July 2018. Patients screened self-selected eligible for participation in the trial were enrolled and allocated to Maitland plus conservative therapy group (M+CG) and Conservative therapy group (CG). Two different investigators carried out all tests (MP) in a physical therapy room at the Balneology Department and assessed all variables (NN) at baseline (day 0) and after 3-week treatment period at follow-up (day 21), respectively. The trial was approved by the Regional Research Ethics Committee of the Medical Center in Pécs (7144 – PTE 2018). Due the first clinical trial conducted in the hospital and therefore questionability of implementation of the study, the trial was registered retrospectively on ClinicalTrials.gov (identifier number: NCT04270253). The flow diagram of the trial is displayed in Figure 1.
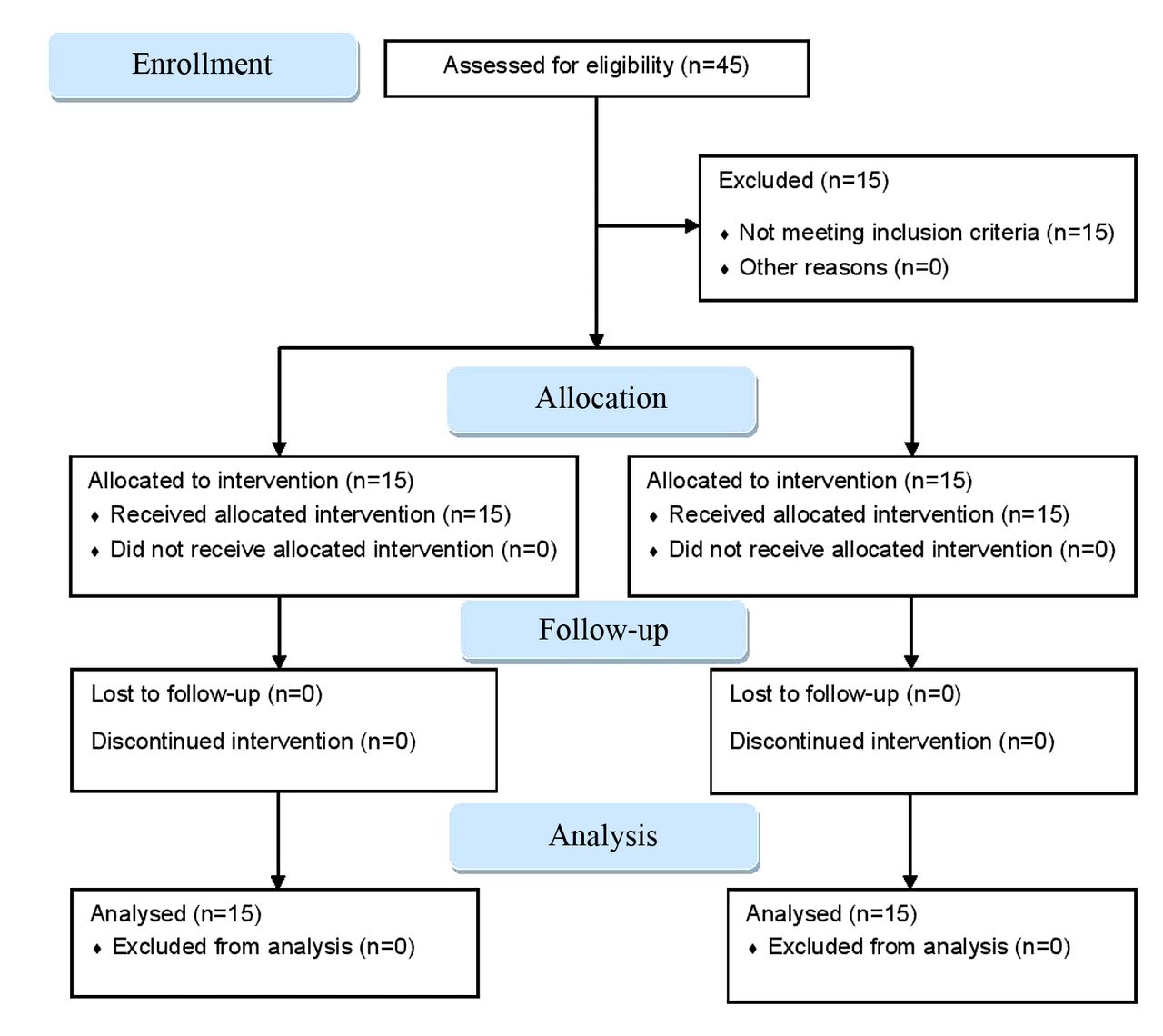
Flow diagram of the trial.
Patients. Inclusion criteria of patients were the clinical classification criteria of KOA according to the American College of Rheumatology (24, 25), categorization of End of Range Problem based on Maitland’s classification, age above 65 years, at least half year existing and at least 3 pain scores measured with Visual Analogue Scale (VAS) during weight-bearing activities, bilateral, moderate-to-severe symptomatic tibiofemoral KOA with radiographic evidence, at least 90° passive knee flexion range and sufficient mental status. Exclusion criteria were acute inflammation of the knee, intraarticular injections within the last 3 months, total knee replacement in the opposite side, class II obesity (body mass index, BMI>35kg/m2), severe degenerative lumbar spine disease (e.g. spondylolisthesis), systemic inflammatory arthritic or neurological condition, conservative intervention attendance within 6 months, contraindication to conservative therapy and manual therapy, unstable heart condition or complex regional pain syndrome. Written informed consent was obtained from all patients.
Conservative therapy. Conservative therapy for patients in both groups including medical bath, water- and land-based exercises and TENS therapy was delivered in the Department of Balneology. Medical bath and water-based exercises were carried out for 20 min in a total of 15 sessions over the 3-week treatment period, respectively. Medical bath was delivered in carbonyl sulfide containing medical water heated at 34°C. Water-based exercises were applied in the same water heated at 32°C. Land-based exercises and TENS therapy (Tensel Double Smart, Minel Elektronikai Kft, Budapest, Hungary, applied strength between 15-25 mA) were applied 3-times per week for 20 min during the 3-week treatment period. Water-based exercises included dynamic movements of upper and lower limb, isotonic strengthening exercises of muscles around the spine and peripheral joints, exercises for improving balance and coordination. Land-based exercises consisted of exercises improving knee joint range of motion, isotonic strengthening and static stretching exercises for the quadriceps, hamstring and gastrocnemiussoleus muscles. All types of conservative therapy except TENS therapy were delivered as group therapy under supervision of a trained and experienced physiotherapist.
Maitland manual therapy. Patients in M+CG received in addition oscillatory Grade III or IV end-range Maitland mobilization. The different Grades were applied depending on the level of tolerance and pain of each patient (26). Patients laid down on a plinth supine with the knee joint positioned in its actual end-range. Flexion end-range of tibiofemoral joint was mobilized with accessory technique, which either reproduced the knee pain or was the most limited in flexion end-range. Extension end-range of tibiofemoral joint was mobilized with physiological extension technique due performing accessory technique in extension end-range is difficult and strength-demanding. Flexion and extension end-range of patellofemoral joint was mobilized with accessory, longitudinal caudal and cranial technique of the patella following the physiological movement of the patella, respectively. The applied manual contact precisely reproduced the hand positioning of the mobilization by movement of the therapist’s body without applying any other movement in all cases. All mobilizations were performed as described by Maitland (16). Both knees were mobilized in every session. All mobilizations were repeated twice at the rate of one oscillation per second for 2 min in each session, twice a week, 6 times in total during the 3-week treatment period. Mobilizations were performed individually in a physical therapy room of the Department of Balneology after the daily conservative intervention with a 20-sec break between each mobilization by a classified Maitland manual therapist (MP). Neither during the 3-week treatment period, nor after the applied mobilizations were confounding factors or adverse events observed resulting in exacerbation of symptoms and consequently in patient drop out.
Outcome measures. Pain: Perceived pain intensity was evaluated using VAS on a 0-10 mm line, with 0 being no pain and 10 being as worst imaginable pain (27). Patients were instructed to rate their average level of pain in general (VAS 1), during getting up from a chair (VAS 2), during getting in car (VAS 3), during turning while walking (VAS 4) and during stair descending (VAS 5).
Passive range of motion (PROM): Flexion and extension passive range of motion (PROM) of knee joints were measured bilaterally with the full-circle 1°-increment plastic standard long-arm extendable goniometer (Elite Medical Instruments, USA) with a moveable arm (28). Flexion PROM and extension PROM was measured in prone and supine position, respectively, with the patient lying comfortably on the plinth (29). Onset of pain determined end-range in both measurements. Every test was performed 3-times.
Peak muscle force: Peak voluntary isometric muscle force of quadriceps and hamstring muscles were evaluated in both legs using CITEC hand-held dynamometer (CIT Technics, Haren, The Netherlands) (30). Patients were in sitting position with 90° hip and knee flexion. The dynamometer was placed on the tibia at 30 cm distally from the knee joint line over the anterior and posterior surface. Patients were instructed to exert maximal force by pushing the shin against the dynamometer. Verbal encouragement was given to patients during each contraction. With 30 s rest interval for avoiding muscle fatigue, three consecutive contractions of 3-5 sec were recorded in Newton (N) for each muscle group.
Functional performance: Timed Up and Go Test (TUG) and 6-Minute Walk Test (6MWT) were used to evaluate patients’ functional performance. TUG is a standardized test, according to which patients were instructed to rise from a standard armchair, walk to a point on the floor 3 meters away, return to the chair, and sit down while being timed in sec with a stopwatch. Patients performed this test in their own pace (31). During the 6MWT, patients were instructed to walk as far as possible for 6 min on a 50 m long corridor back and forth. The total distance covered in meters was measured (32).
Statistical analysis. Shapiro-Wilk test was conducted to examine distribution of the measured variables. Considering results of the normality tests, independent samples t-test was used to assess difference in the demographical data and baseline values between the groups, such as age, height, weight, BMI, duration of symptoms, all PROM and peak muscle force variables; Mann-Whitney U-test was used to calculate baseline differences between groups in all other variables. The differences between post- and pre- treatment values were examined with paired sample t-test or Wilcoxon-test and the magnitudes of changes were expressed in percentage. These percentages were then compared between groups using independent sample t-test or Mann-Whitney U-test, depending on the distribution of the variable. All calculations were carried out and analyzed with IBM SPSS Statistics 25.0 (IBM Corp., USA). Results are presented in median with 25 and 75 percentiles and the percentage change in mean with standard deviation (SD). All p-values equal or below 0.05 were considered statistically significant.
Results
Thirty patients (17 women, 13 men, mean age=68.63±8.34 years) were found eligible and participated in the trial. All involved patients completed follow-up and were analysed. No significant differences were found in baseline characteristics between both groups (Table I). No significant differences were found in any outcome parameters between both groups at baseline, except the greater right hamstring peak muscle force in M+CG (p<0.001) (Table II).
Demographic characteristics of patients.
Pre- and post- treatment results of PROM, peak muscle force, TUG and 6MWT.
Pain. All post-treatment VAS pain scores reduced significantly in both groups compared to the pre-treatment scores. Moreover, the magnitude of these reductions was significantly greater in the M+CG compared to the CG group (VAS 1: 42.78%, p=0.002; VAS 2: 40.67%, p<0.001; VAS 3: 35.84%, p=0.004; VAS 4: 35.43%, p=0.008; VAS 5: 31.02%, p=0.004) (Table III).
Pre-, and post- treatment results of the different visual analogue scale (VAS) pain scores.
PROM. Flexion and extension PROM improved significantly in both groups compared to the pre-treatment scores. Furthermore, the magnitude of improvement of flexion PROM of both knees was significantly greater in the M+CG compared to the CG group (right side: 14.66%, p=0.01; left side: 15.35%, p<0.001) (Table III).
Peak muscle force. All peak muscle force values increased significantly in both groups after treatment, compared to pretreatment scores. Moreover, the magnitude of improvement of right hamstring peak muscle force was significantly greater in the M+CG compared to the CG group (32.26%, p=0.045) (Table III).
Physical performance. TUG decreased and 6MWT improved significantly in both groups compared to the pre-treatment scores. Furthermore, the magnitude of improvement of 6MWT was significantly greater in M+CG compared to CG (31.45%, p<0.001) (Table III).
Discussion
The greater reduction of general VAS pain score in M+CG suggests the additional hypoalgesic effect of end-range Maitland mobilization attributed to multiple neurophysiological mechanisms (33, 34) and stretching of the tightened periarticular tissues (35-37). Azlin et al. showed the positive effect of Maitland mobilization in addition to different land-based exercises followed by thermal therapy against different land-based exercises and thermal therapy alone on reduction of general pain. However, this trial studied a 4-week-long treatment period (17). In contrast, Rao et al. reported alleviation of pain immediately following the Maitland mobilization in KOA patients (18). However, the more non-noxious input and consequently the hypoalgesic effect of all of the performed Grades with different techniques could have contributed to the rapid alleviation of pain in that trial. The functional activities are often reported as painful everyday movements and pain is indirectly related to the functional status in KOA. Our results, compared to previous research, indicate greater hypoalgesic effect of end-range Maitland mobilization due to effects discussed previously regarding general pain. Direct comparison cannot be made regarding pain intensity during certain functional activities, because they were not investigated in earlier trials. However, these findings might serve as an important measurement that could be used in future trials.
The greater change of flexion PROM in M+CG can be attributed to the improved extensibility of the tightened periarticular tissues as a result of end-range Maitland mobilization (16). This finding corroborates previous studies regarding improvement of PROM of different joints’ (21-23). However, neither conservative therapy, nor 3-week treatment period was applied in addition in any of these trials. Some explanations for the improvement of flexion PROM in M+CG: firstly, end-range accessory movement increases the arthrokinematic movement of the joint in contrast to end-range physiological movement, which is required for achieving full passive and subsequently active range of motion. Direction and type of end-range accessory mobilization is determined in Mulligan manual therapy (38), while only the direction of end-range accessory mobilization is determined in Maitland manual therapy. Therefore, the applied end-range accessory Maitland mobilization might be able to improve the arthrokinematic movement of the mobilized joint as well, independently from its type, and should be applied primarily as suggested by Maitland et al. (16). Secondly, the improvement of extension against flexion PROM, in general, demands more time in clinical practice. One explanation for this may be attributed to the increasing tissue resistance whilst approaching end-range of extension PROM due to the screw-home mechanism. Therefore, improvement of extension PROM in both groups may be attributed to the improvement of elasticity of connective tissues by conservative therapy (3, 4). Although mobilization of patellofemoral joint with end-range accessory technique in addition to land-based exercises increase extension PROM in patients with patellofemoral pain syndrome (39), mobilization of tibiofemoral joint with accessory technique may produce greater effect on improvement of extension PROM instead of physiological technique in KOA.
The greater improvement of right hamstring peak muscle force in M+CG can be attributed to the arthrokinetic reflex. Page et al. suggested that a dysfunctional joint causes a secondary inhibition of muscle activation via anterior horn motor cells leading to decreased muscle force (40). Arthrokinetic reflex activated by mobilization through stimulation of joint mechanoreceptors can inhibit this mechanism and therefore increases motor unit activity (41, 42); however, only in the less painful side of bilateral KOA, based on our present result. As previous data on the effect of end-range mobilization on peak muscle force are inconsistent (43, 44), the observed improvement of peak force of both quadriceps and left hamstring muscles in both groups is considered primarily due to the effect of land-, and water-based exercises (3, 4). The inappropriate stimulation of mechanoreceptors might be attributed to either the high age of patients or the severity of KOA. Reinke et al. showed that stimulation of the peripheral cutaneous mechanoreceptors is not age-related in rats (45). Although no data are available for humans, there may be differences in the stimulations of mechanoreceptors according to age or degree of joint damage. Furthermore, the correspondence between severity of KOA and stimulation of mechanoreceptors is unclear. Thus, further trials might be needed to clarify this relationship.
The greater improvement regarding 6MWT in the M+CG group indicates an additional effect of end-range Maitland mobilization on functional performance. Some possible explanations are proposed for this finding: firstly, patients in M+CG experiencing greater alleviation of pain could have led to putting greater load on their knees and walk consequently longer distance during 6-minute walk. Secondly, knee flexion PROM depends on the elasticity of both the vasti and the rectus femoris muscle. The elasticity of rectus femoris muscle, however, also influences hip extension, which is an important contributor to stride length during gait (46, 47). Therefore, the greater increase of flexion PROM and right hamstring peak muscle force together might have contributed to the improved walking distance in M +CG. Our result corroborates previous finding of Kappetijn et al. concerning 6MWT (44); however, in that study, end-range Maitland mobilization was performed in the first 12 sessions of an 8-week treatment program, along with land-based knee exercises. Regarding the TUG test in the present trial, the decrease of time in both groups might be attributed to the cumulative effect of conservative therapy on all measured physical parameters (3, 4); however, not likely attributed to alleviation of pain. Contrary to our suggestion, Rao et al. reported an immediate decrease of TUG time after performing different Grades of both Maitland mobilization techniques without addition of conservative therapy, in contrast to the present result (18); however, patients with mild-to-moderate severity of KOA were mobilized in that trial, in contrast to patients presenting moderate-to-severe severity of KOA in the present trial. Therefore, the impact of end-range Maitland mobilization on dynamic balance may depend on the severity of KOA independently from alleviation of pain. Future studies should focus on clarification of this supposition.
Some limitations should be highlighted. Patients in M+CG were not blinded and patients in CG were not receiving sham intervention. Therefore, the improved performance in M+CG, mainly in determination of pain, may be attributed to awareness of patients receiving Maitland manual therapy. Therefore, performance bias could be present. Furthermore, the small sample size may limit the generalizability of the present results. Additionally, the present trial focused especially on the effect of mobilization of the tibiofemoral and patellofemoral joints, despite examination and mobilization of the adjacent joints near the knee joint is recommended based on Maitland manual therapy.
Conclusion
This study design is capable of investigating the effect of end-range Maitland mobilization in addition to conservative therapy, in a 3-week inpatient rehabilitation care, on KOA. In this pilot study, both interventions (CG and M+CG) were effective in alleviation of pain and improvement of physical function in KOA. However, oscillatory Grade III or IV end-range Maitland mobilization in addition to conservative therapy provided superior effect on alleviation of pain in general and during certain functional activities, on flexion PROM of both knees, on right hamstring peak muscle force and on 6MWT, compared to conservative therapy alone, in patients with moderate-to-severe KOA. Therefore, these outcome measures are good indicators for evaluating the effect of end-range Maitland mobilization. However, several modifications may be required in future studies to avoid performance bias mentioned earlier. Firstly, a multicenter interventional trial with bigger sample size should be performed. Secondly, patients should be blinded. For this reason, sham therapy should be performed in control group. Thirdly, the 3-week treatment period could be complemented by 3-month follow-up. These changes together could lead to further information regarding both the short- and long-term effect and the superiority of end-range Maitland mobilization in KOA. As a consequence, the effectiveness and importance of end-range Maitland mobilization in addition to conservative therapy can be highlighted in KOA as well.
Acknowledgements
The support of Harkány Thermal Rehabilitation Centre, University of Pécs as well as patients for their contributions is appreciated.
Footnotes
Authors’ Contributions
Miklós Pozsgai acquisited and analysed data and drafted the article; Erzsébet Kövesdi recruited patients and drafted the article; Balázs Németh and István Kiss recruited patients; Nelli Farkas conducted the statistical analysis; Tamás Atlasz analysed data and drafted the article; Márk Váczi conducted the study design, drafted the article and approved the final version; Nóra Nusser recruited patients, conducted the study design, drafted the article and approved the final version.
This article is freely accessible online.
Conflicts of Interest
Authors declare that they have no conflicts of interest.
- Received January 5, 2021.
- Revision received March 18, 2021.
- Accepted March 14, 2021.
- Copyright© 2021, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.