


Abstract
Background: Time-to-treatment is defined as a quality indicator for cancer care but is not well documented. We investigated whether meeting Norwegian timeframes of 35/42 days from referral until start of chemotherapy or surgery/radiotherapy for lung cancer was associated with survival. Patients and Methods: The medical records of 439 lung cancer patients at a regional cancer center were reviewed and categorized according to treatment: (i) surgery; ii) radical radiotherapy; iii) stereotactic radiotherapy; iv) palliative treatment, no cancer symptoms; v) palliative treatment with severe cancer symptoms). Results: Proportions receiving timely treatment varied significantly at 39%, 48%, 10%, 44% and 89%, respectively (p<0.001). Overall, those starting treatment on time had the shortest median overall survival (10.6 vs. 22.6 months; p<0.001). This was also the case for palliative (5.3 vs. 11.4 months) (p<0.001) but not for curative treatment (not reached vs. 38.3 months) (p=0.038). Conclusion: Timely treatment is not necessarily associated with improved survival.
The incidence of cancer is growing, and it is now a leading cause of death worldwide (1-5). The burden of malignant diseases is a public and political concern and has led to increasing attention being paid to the quality and organization of cancer care. One common perception is that a long interval until treatment starts worsens the prognosis due to tumor growth while waiting (6), and many guidelines for cancer care organization include recommendations for timeframes until treatment start.
Lung cancer is among the most common malignant diseases, the prognosis is poor, and it is the most common cause of cancer-related death (3, 7-9). Due to the rapid disease evolvement in many patients with lung cancer, we deem it to be one of the most relevant types of cancer to study when investigating whether time until treatment start affects survival.
Despite this being the subject of many studies, the importance of diagnostic delay is uncertain. Some studies show associations between increased mortality and long waiting time for diagnostic procedures to be completed (10, 11), or treatment to start (12-15), but only when timeframes are as long as 3 to 4 months (16, 17). Paradoxically, other studies have shown that long intervals are associated with improved survival (18-23), probably due to differences in number and types of investigations included in diagnostic workup for different stages of disease (24-26). Others found no such associations (27-29), and thus the evidence of time for diagnostic workup being a prognostic factor in lung cancer is limited.
The recommended time to starting lung cancer treatment ranges from 35 days to 3 months in different countries (30-32). In Norway, recommended timeframes from receiving a referral letter for suspected lung cancer until the start of treatment are 35 calendar days for systemic cancer therapy and 42 days for surgery and radiotherapy. We found that the proportions at our hospital of patients who started lung cancer treatment within recommended timeframes were 35% for curative and 65% for palliative treatment (33). In the present study, the aim was to investigate whether patients who started treatment within these timeframes had longer survival than those who started treatment later.
Patients and Methods
Study setting. St. Olav’s Hospital, Trondheim University Hospital, in Trondheim, Norway, is the regional cancer center for the Central Norway Health Region which has 700,000 inhabitants, and it is the primary hospital for 317,000 people. All facilities for diagnosis and treatment of lung cancer are available, including a Tumor Board, of pulmonologists, thoracic surgeons, oncologists, thoracic radiologists, specialists in nuclear medicine, pathologists and a patient coordinator, which meets twice every week.
Study design, patients and definitions. We performed a retrospective review of the individual electronic medical records of all patients who were diagnosed with lung cancer at the Department of Thoracic Medicine at St. Olav’s hospital between January 1, 2011 until December 31, 2013. Further details of the conduct of the study were presented in a previous article (33). Stage of disease was assessed according to the seventh edition of the TNM classification of lung cancer (34).
Start of the diagnostic workup was defined as a) the date when a referral letter for suspected lung cancer was received at the Department of Thoracic Medicine, or b) the date when diagnostic workup for suspected lung cancer was initiated for a patient with a single pulmonary nodule who had been previously observed (‘watchful waiting’). Survival was defined as the time from the start of diagnostic workup until death from any cause. ’Time to treatment’ was defined as the interval from the start of diagnostic work-up until the day of surgery or the first day of radiotherapy or systemic therapy.
We defined ’timely’ as a time to treatment of ≤42 days for surgery or radiotherapy or ≤35 days for systemic therapy. If intervals were longer, time to treatment was categorized as ’untimely’. For the subgroup analyses, we defined five treatment groups: i) Surgery: Patients who underwent surgery for stage I-III disease; ii) Other standard curative: Radical radiotherapy for stage III non-small-cell lung cancer (NSCLC), or radio-chemotherapy for stage I-III (limited stage) SCLC; iii) Secondary curative: Stereotactic radiotherapy or radical radiotherapy for stage I-II NSCLC for patients who were ineligible for surgery; iv) Palliative, no severe symptoms: Palliative treatment for patients with no severe cancer symptoms; v) Palliative, severe symptoms: Palliative treatment for patients who presented with neurological symptoms, symptoms due to infiltration of mediastinal structures (e.g. airway obstruction, hoarseness, dysphagia, superior vena cava syndrome), bone pain, other pain due metastases, or weight-loss ≥5% in the 3 months prior to diagnosis.
We used the forced expiratory volume in 1 second (percentage of expected value, FEV1%) as a measure of pulmonary function, and the Charlson comorbidity index score without age-adjustment as a measure of comorbidity.
Analyses were performed using the Stata/IC 14.2 package for Windows (StataCorp LLC, College Station, TX, USA). We used chi-square statistics for bivariate analyses and log-rank test for survival analyses. A two-sided p-value of less than 0.05 was defined as the level of statistical significance.
Ethics. The study, including the use of a passive consent procedure, was approved by the Regional Committee for Medical and Health Research Ethics in Western Norway (REK Vest (2014/60). Patients still alive received written information about the study and were given the opportunity to decline participation by completing a form and return it in an enclosed, prepaid envelope.
Results
Patient characteristics. A total of 453 patients were diagnosed with lung cancer at the Department of Thoracic Medicine between January 1, 2011 and December 31, 2013, of whom five declined participation. Another nine patients were excluded from the analyses due to uncommon thoracic malignancies: Carcinoid (n=6), clear-cell carcinoma (n=2), and epithelial/myoepithelial carcinoma (n=1).
Of the 439 patients analyzed, 203 (46%) were women; 155 (35%) >75 years; 311 (71%) had NSCLC and 63 (14%) had no histologically or cytologically confirmed diagnosis. One hundred and forty-seven (33%) had stage I-II disease; 113 (26%) stage III; and 179 (41%) stage IV (Table I).
Patient characteristics.
Eleven patients with preliminary stage I-IIIA on the initial computed tomography (CT) scan and fit for curative treatment were upstaged and received palliative treatment due to metastasis revealed on positron-emission tomography CT (n=9), brain magnetic resonance imaging (n=1), or bone scan (n=1). Fourteen patients were upstaged from clinical stage I to pathological stage II (n=9) or III (n=5) after surgery, and six patients with clinical stage II had pathological stage III disease. We were not able to assess performance status due to missing data in a large proportion of the medical records.
One hundred and nine patients (25%) underwent surgery; 42 (10%) other standard curative treatment; and 31 (7%) secondary curative treatment. Among those who received palliative treatment, 88 (20%) had severe symptoms, and 85 (19%) did not. Eighty-four patients (19%) did not receive any cancer therapy. Among these, seven patients died before treatment started, one due to complications of a diagnostic procedure.
There were no statistically significant differences in sex distribution, or the proportion aged >75 years between the treatment groups. There were significantly more patients with an FEV1% <80% of the expected value (p=0.004), a Charlson comorbidity index score of >2 (p=0.033), and no histologically or cytologically confirmed diagnosis (p≥0.001) among the patients in the secondary curative treatment group than among those who underwent surgery or other standard curative treatment. In addition, there was a trend towards more patients with stage I disease in the secondary curative treatment group than in the surgery group (p=0.052). In the palliative treatment group without severe symptoms, the proportion with stage I-III disease was significantly higher than among those in the group of palliative treatment with severe symptoms (p=0.007) (Figure 1).
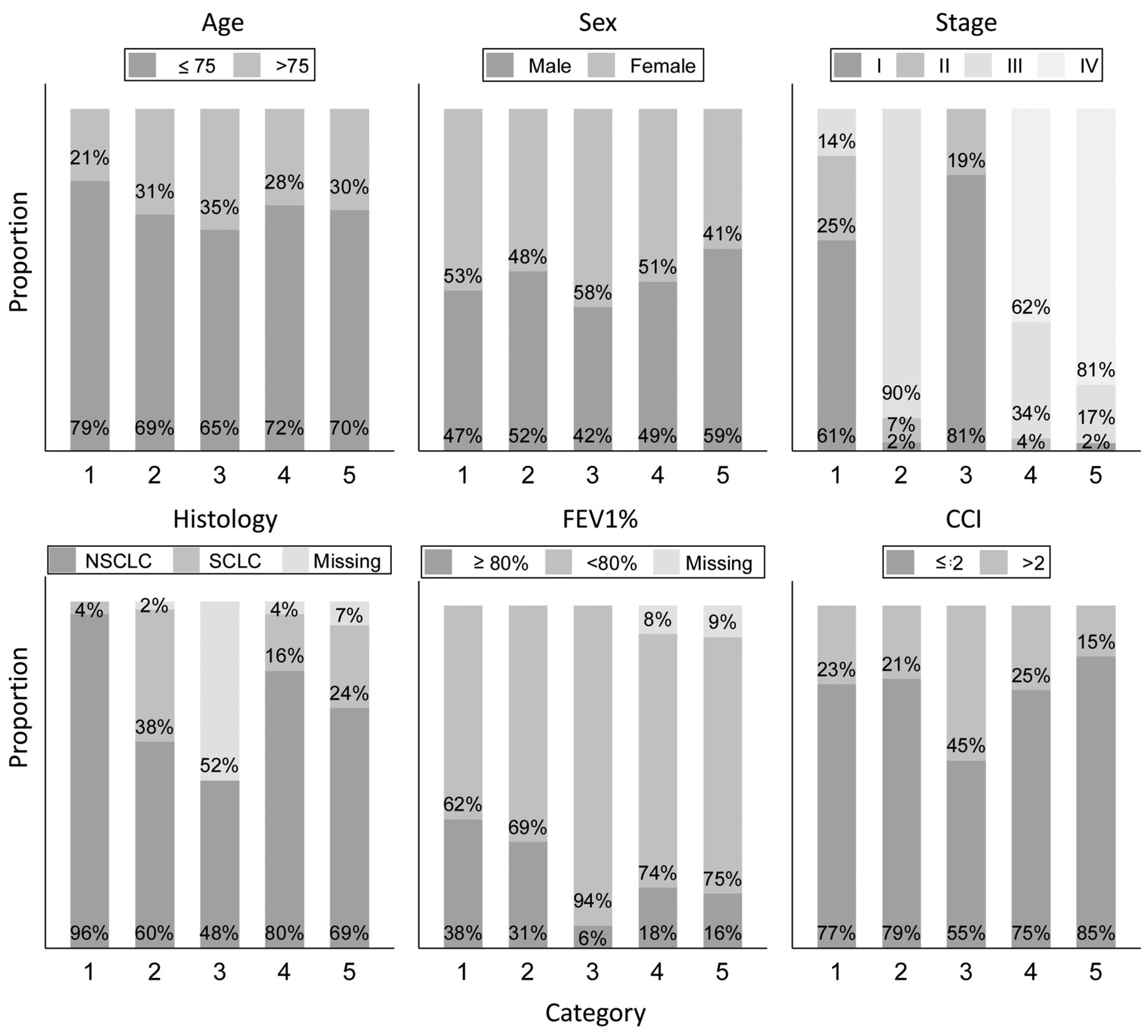
Distribution of patients according to important characteristics by treatment category: 1) Surgery for stage I-III disease; 2) radical radiotherapy for stage III non-small-cell lung cancer, or chemo-radiotherapy for stage I-III small-cell lung cancer; 3) stereotactic radiotherapy or radical radiotherapy for stage I-II non-small-cell lung cancer; 4) palliative treatment, no severe cancer symptoms; 5) palliative treatment for patients presenting with severe cancer symptoms. CCI: Charlson comorbidity index score; FEV1%: forced expiratory volume in 1 second (percentage of expected value).
Timeliness. Overall, 180 (51%) received timely treatment, and the proportion varied significantly (p<0.001) between the groups: 39% among those who underwent surgery [with a median number of days until treatment : 49 (range=5-296) days]; 48% in the other standard curative treatment group [median=42 (range=2-90) days]; 10% in the secondary curative treatment group [median=63 (range=29-168) days]; 44% in the palliative, no severe symptoms group [median 42 (range=6-201) days]; and 89% in the palliative with severe symptoms group [median=23 (range: 3-90) days] (Figure 2).
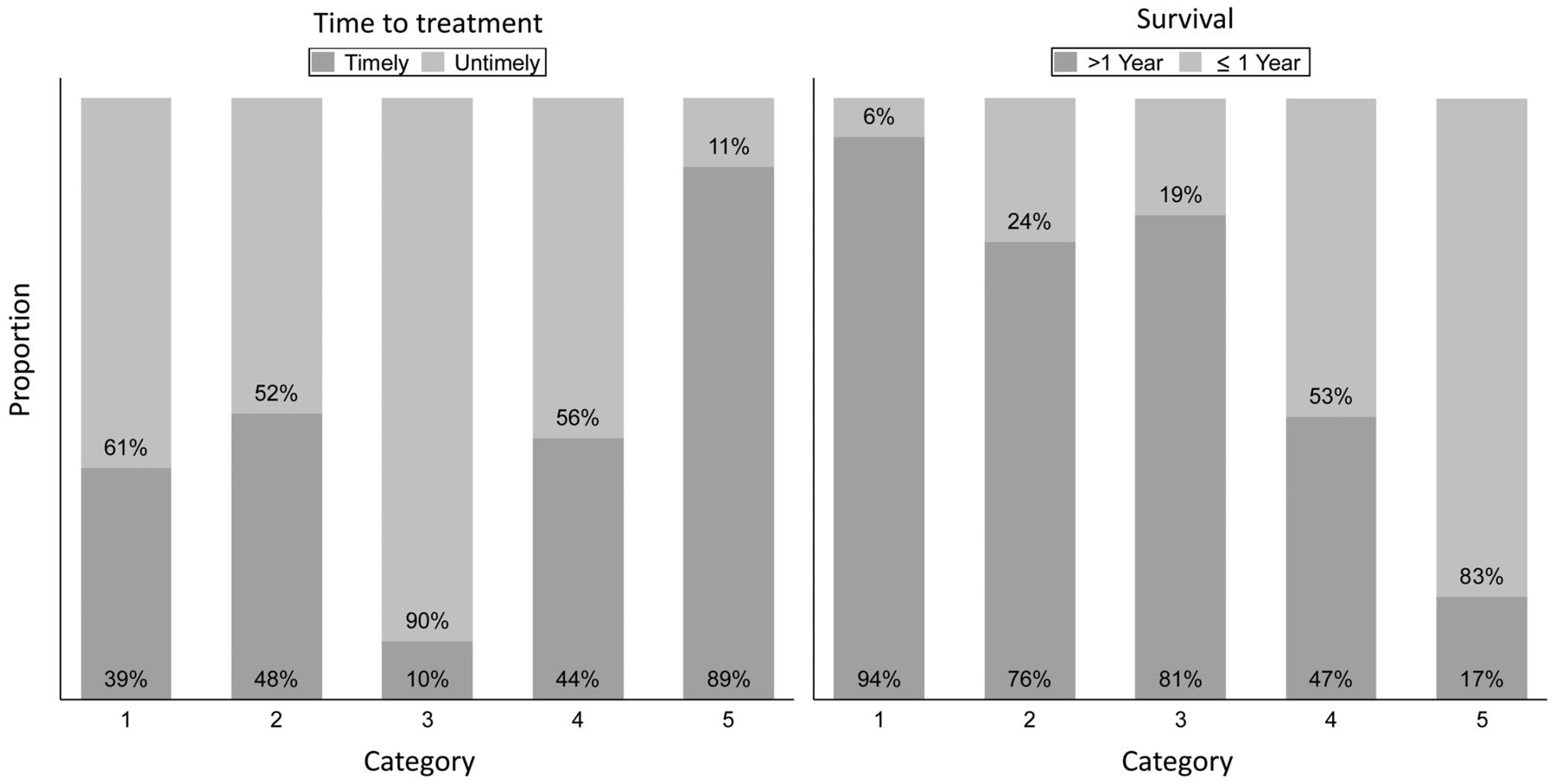
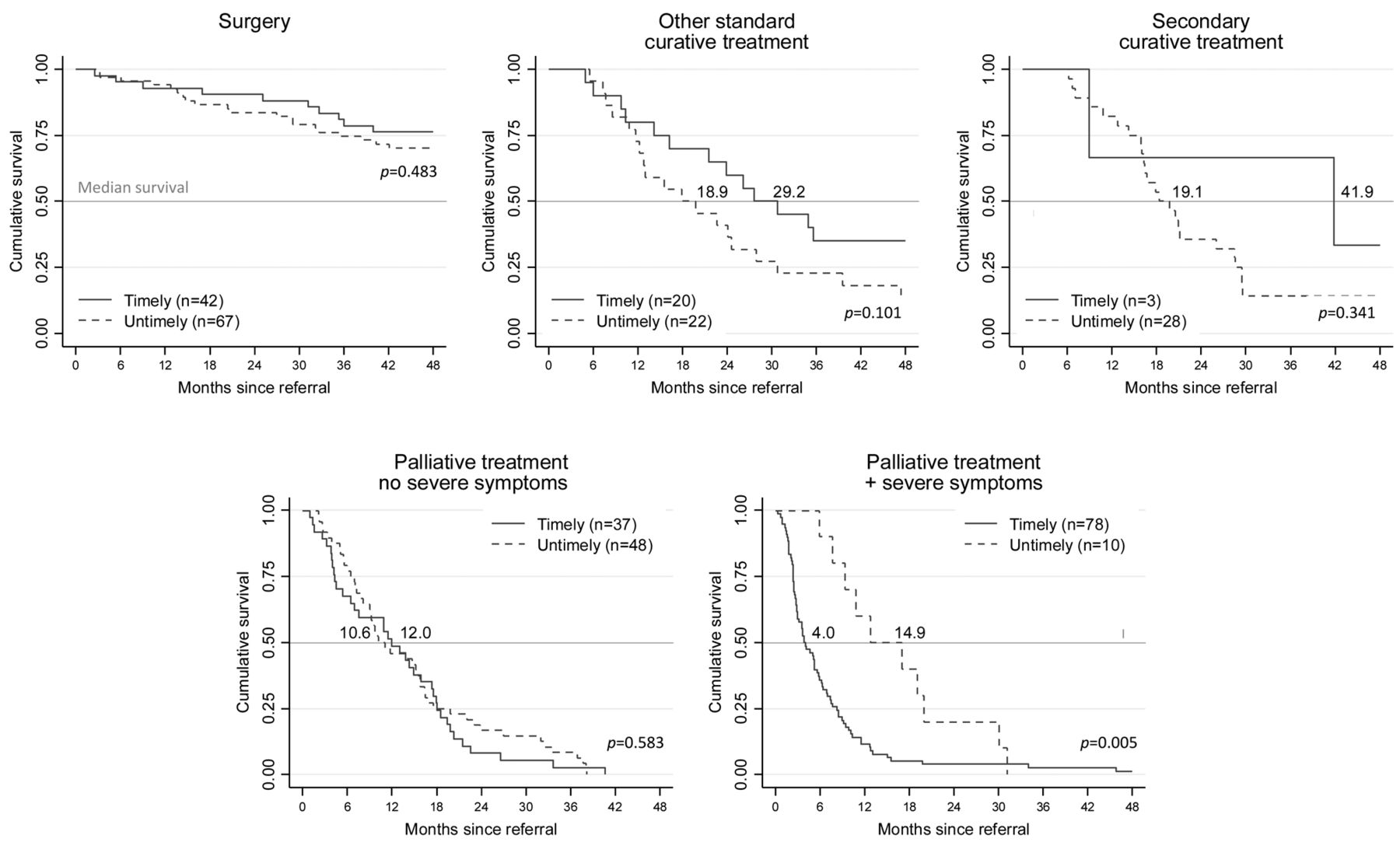
Timeliness of lung cancer treatment and survival by treatment category: 1) Surgery for stage I-III disease; 2) radical radiotherapy for stage III non-small-cell lung cancer, or radio-chemotherapy for stage I-III small-cell lung cancer; 3) stereotactic radiotherapy or radical radiotherapy for stage I-II non-small-cell lung cancer for patients ineligible for surgery; 4) palliative treatment, no severe cancer symptoms; 5) palliative treatment for patients with severe cancer symptoms.
In the other standard curative treatment group, the proportion of patients aged >75 years was significantly higher in those who received untimely treatment (45% vs. 15%; p=0.033). In the group with palliative treatment with severe symptoms, there was a higher proportion of stage I-III disease in those who received untimely treatment (50% vs. 15%; p=0.009). Otherwise, baseline characteristics were well balanced between those who received timely treatment and those who did not within each treatment group (data not shown).
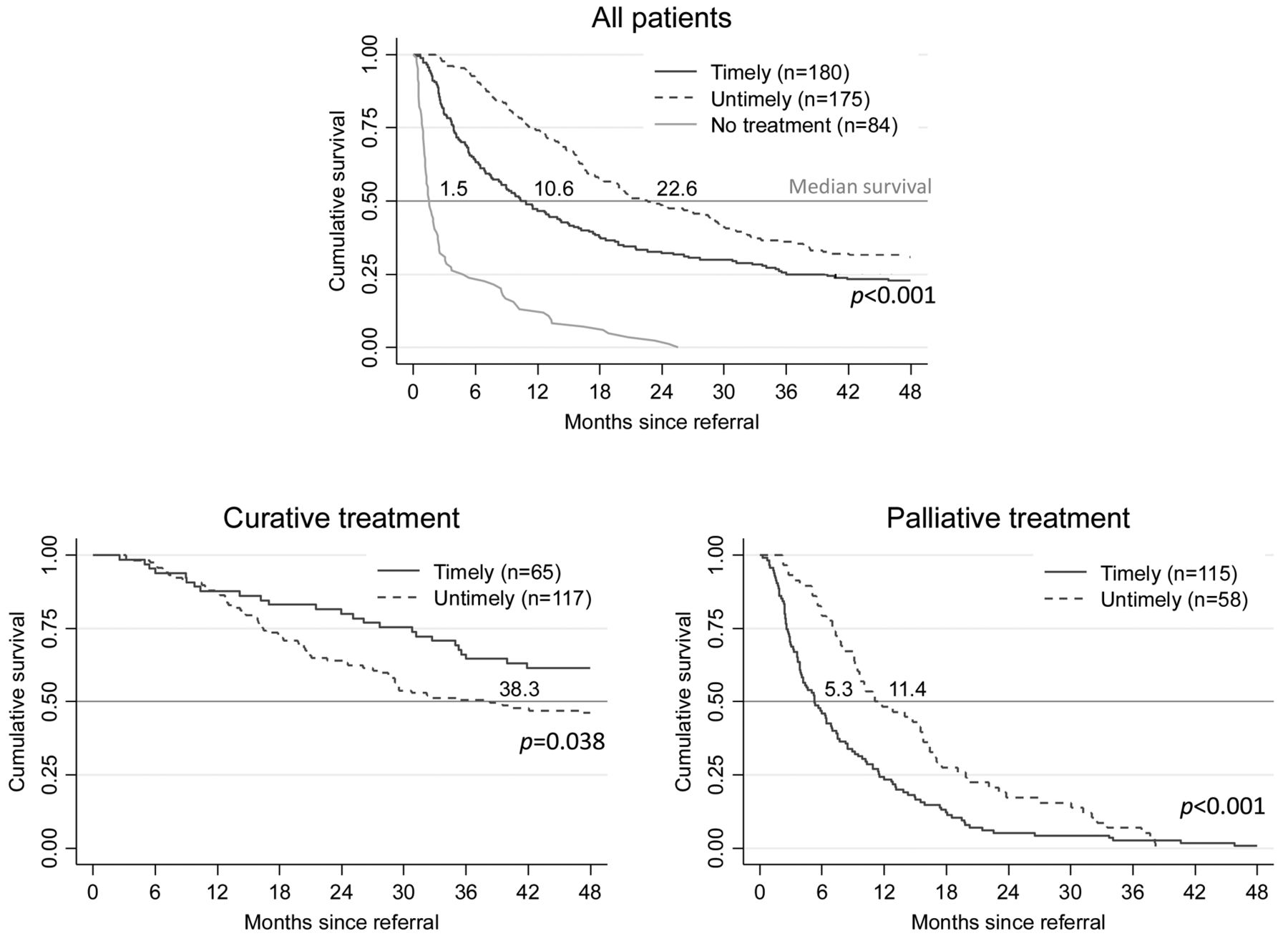
Survival. Considering the total population, the median overall survival was 10.6 months among those who received timely treatment, and 22.6 months among those who received untimely treatment (p<0.001). Those who did not receive any cancer treatment had a median overall survival of 1.5 months. Among curative patients, those who received timely treatment had a better median survival (timely=not reached, untimely=38.3 months; p<0.038), whereas the opposite was the case among those who received palliative therapy (timely=5.3 months, untimely=11.4 months; p<0.001) (Figure 3).
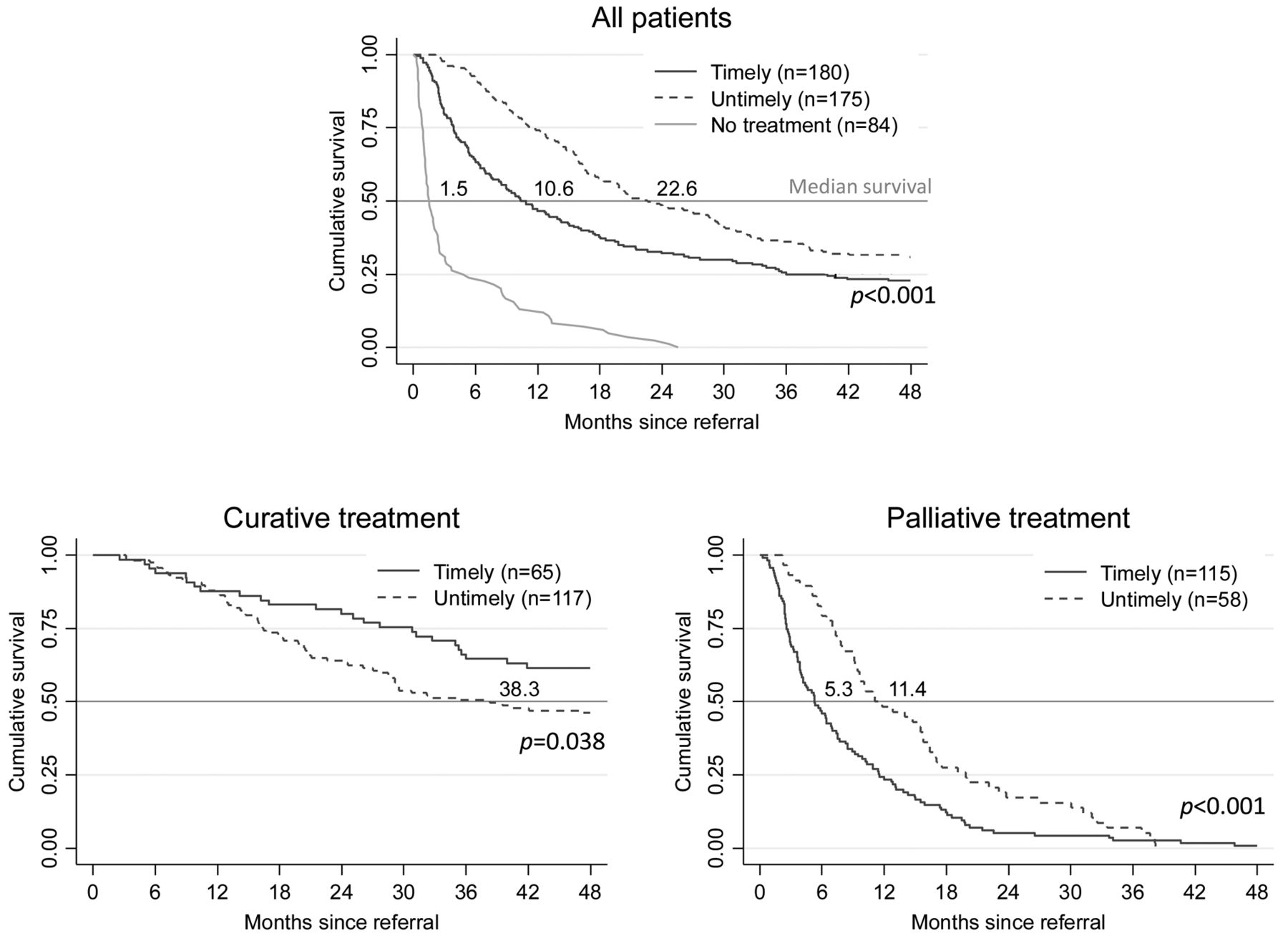
Overall survival according to timeliness of treatment for all patients, for those receiving curative, and those receiving palliative treatment.
The subgroup analyses revealed that there were no survival differences between those who received timely and untimely treatment among those who underwent surgery, other standard curative therapy, or those who received palliative treatment and had no severe symptoms. For the group which received secondary curative treatment, there was a large numerical difference in median overall survival (timely=41.9 months, untimely=19.1 months; p=0.341), although only three patients started timely treatment in this group. Those who received untimely palliative treatment and had severe symptoms lived significantly longer than those who received timely treatment (14.9 vs. 3.9 months; p=0.005) (Figure 4).

Overall survival according to timeliness by treatment group.
Discussion
In this study of patients diagnosed with lung cancer at a regional cancer center in Norway, we found that patients who received timely treatment had a much shorter overall survival than those who started treatment later than recommended by the Norwegian guidelines. Subgroup analyses revealed that among those who received curative treatment, there was a survival benefit of timely treatment, while the opposite was the case among those who were offered palliative treatment. When analyzing patients who underwent surgery or other curative treatment separately, there was no survival benefit among those who received timely treatment. Among patients who received palliative treatment, there was no survival benefit of timely treatment among those with no severe symptoms. Among the group with severe cancer symptoms, those who received timely treatment had a significantly shorter survival than those who received untimely treatment.
The results of other studies of timeliness in cancer care are not consistent. It has been demonstrated that tumors grow and that the grade of invasion and the number of metastases can increase while waiting to start treatment (12-16, 35) but it is unclear whether this actually influences the prognosis of the patients when the time to treatment is shorter than 3 to 4 months. The recommended timeframes vary between countries, and many are longer than in Norway (24, 26, 30, 31).
Review articles published in 2009 (36) and 2015 (37) showed that most studies reported negative or no association of timely care and survival for patients with lung cancer survival, while positive associations were related to long intervals (>4 months) from mass screening until diagnosis (10, 11), or late referral to a specialist for symptomatic disease (38). Among more recent publications, five report positive associations of timely treatment and survival in those with localized disease (15-17, 24, 35), five studies found a negative association (18, 20, 23, 39, 40), while two found no associations at all (27, 29).
The retrospective, descriptive study design does, of course, not allow for assessing whether shortening the time from the start of diagnostic workup until the start of treatment influences a patient’s prognosis. It does, however, provide valuable information about the potential impact of reducing the diagnostic workup time. As we have previously reported (33), there is a large heterogeneity with respect to what kind and number of procedures are required before the diagnostic workup is completed in patients with lung cancer. Furthermore, some patients need treatment for concomitant diseases, indicating that the timeframes cannot and should not always be met.
The most important clinical factor that influenced the time for diagnostic workup in potentially curative disease in our cohort was poor lung function. Patients with lung cancer have a high comorbidity burden, higher than most other patients with cancer due to a relatively old age at diagnosis and a history of tobacco smoking (41-44). Not all patients are eligible for standard therapy due to comorbidity, and the treatment alternatives may be less effective (45, 46). In our cohort, many patients with poor lung function or other severe comorbidity received radiotherapy instead of surgery for stage I-II disease, and those who received secondary curative treatment had significantly shorter overall survival than those who underwent surgery. However, the patients in the secondary curative treatment group also had significantly shorter progression-free survival (data not shown), possibly suggesting that the survival difference was not only due to deaths caused by comorbidity, but also to inferior disease control from radiotherapy than achieved after surgery.
There is also a large heterogeneity between patients with the same stage of disease. Each patient’s cancer may behave biologically differently, and symptoms may provide prognostic information (47, 48). This was most evident among patients with advanced disease who received palliative treatment. As demonstrated in other studies, patients with severe cancer-related symptoms had a shorter prognosis than those without, even though their waiting time until treatment time was shorter (49-51).
Our study was a single-center study and the results may not be generalizable. Diagnostic work-up at our hospital during the study period was suboptimal due to limited positron-emission tomography CT capacity, and it was not possible to retrieve data on performance status due to missing data. On the other hand, our study cohort consisted of an unselected patient population, and data were complete and collected by a comprehensive review of each patient’s hospital medical records by an experienced physician (TS), and the sample size was fairly large. There were imbalances in baseline characteristics but some are covariates, e.g. stereotactic radiosurgery is only offered to patients without lymph node metastases, which explains the imbalance with respect to disease stage between the standard and secondary curative treatment groups. One might argue that the impact of time to treatment differs between important subgroups and should be analyzed separately. For example, small-cell lung cancer is the most rapidly-progressing subgroup of lung cancer and it is generally accepted that treatment should start as soon as possible, whereas patients with sensitizing epidermal growth factor receptor mutations receiving targeted therapy respond better to treatment than most other patients with advanced NSCLC, and survival may be less affected by time to treatment. The number of patients was too low to allow for such subgroup analyses but results were similar when excluding these patients (data not shown), and all recommended timeframes we are aware of apply for all patients with lung cancer.
The most surprising observation was that overall, patients who received untimely treatment had a longer survival than those who received timely treatment. Looking at the survival curves in Figure 4, it is evident that this finding is mainly due to a large difference between the groups among patients with severe symptoms who received palliative treatment. In this group, those with severe symptoms who received untimely treatment had weight loss as their main symptom, and it appears that the other symptoms we defined as severe in this setting are more strongly associated with a short prognosis. We still believe that our results illustrate that the complexity of the extent of disease, required diagnostic workup and treatment effect need to be taken into consideration when assessing quality of cancer care, and that time until treatment alone has limited value as a quality indicator.
A prospective randomized trial is needed in order to assess whether shortening the time until treatment improves survival. There are, however, several practical and ethical challenges associated with such a trial design, and our study does not indicate that time until treatment start alone is an important prognostic factor. Based on our previous analyses, however, we do believe that the number of diagnostic procedures, and hence the time for diagnostic workup, can be reduced by training healthcare personnel to choose wisely and adhere to guidelines (52). Thus, we believe that a system for continuous quality assurance of diagnostic workup is more feasible than a randomized trial and may be a better approach for improving outcomes for patients with lung cancer than solely focusing on reducing the time until treatment.
In conclusion, time until the start of treatment was a significant independent prognostic factor in our cohort of patients with lung cancer but the associations varied significantly between important subgroups of patients, indicating that reducing the time until treatment alone is unlikely to improve survival for all patients, and that a broader approach is needed to monitor and improve the quality of cancer care.
Acknowledgements
This work was supported by a grant from St. Olav’s hospital, Trondheim University Hospital in Trondheim, Norway. The funder had no role in the data collection and analysis and was not involved in the interpretation of results, writing, revision, or approval of the article.
Footnotes
Authors’ Contributions
TS and BHG conceived and designed the study. TS collected data and performed data analyses. All Authors participated in the interpretation of the data and article writing.
This article is freely accessible online.
Conflicts of Interest
The Authors have declared no conflicts of interest.
- Received February 15, 2021.
- Revision received March 11, 2021.
- Accepted March 18, 2021.
- Copyright© 2021, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}
{kind=link}
{kind=link}
{kind=link}