


Abstract
Background/Aim: Programmed death ligand-1 (PD-L1) and programmed death protein 1 (PD-1) expression levels in many tumors and their correlation with prognosis have been actively studied. However, studies on PD-1 expression and its prognostic value in clear cell renal cell carcinoma (ccRCC) are limited and controversial. In this study, we describe the expression of PD-1 and its prognostic significance and association with clinical features in patients with ccRCC. Materials and Methods: We obtained clinicopathological data from 166 patients with ccRCC who were treated at Gyeongsang National University Hospital, Jinju, Korea between January 2000 and December 2009. Tissue microarray blocks were made using representative paraffin blocks of ccRCC specimens. Two pathologists analyzed PD-L1 and PD-1 expression in both tumor and inflammatory cells. Results: PD-1 expression in tumor-infiltrating inflammatory cells was significantly correlated with unfavorable disease-free survival (DFS) (p<0.001) and disease-specific survival (DSS) (p=0.002) in univariate analysis. A statistically significant correlation between PD-1 expression and unfavorable DFS (p=0.025) was observed in the multivariate analysis. Conclusion: PD-1 expression in tumor-infiltrating inflammatory cells serves as an independent prognostic factor for unfavorable DSS in patients with ccRCC.
Clear cell renal cell carcinoma (ccRCC) accounts for ~80% of all kidney cancers and is a major lethal genitourinary malignancy (1-3). The prognosis of ccRCC depends on clinicopathologic factors, such as stage, size, grade and necrosis (4). Some studies have been performed to identify gene signatures of ccRCC, molecular prognostication strategies and biomarkers (5-7).
Recently, programmed death ligand-1 (PD-L1) and programmed death protein (PD-1) have been under the spotlight. PD-L1 and PD-1 expression in many tumors and their correlation with prognosis have been largely studied (8-13). Recent studies have also demonstrated the expression of PD-L1 and its correlation with prognosis in ccRCC and have reported that elevated levels of PD-L1 expression have a negative prognostic role in ccRCC (14-17). However, studies regarding PD-1 expression and its prognostic role in ccRCC are scarce and controversial (16, 18, 19).
In this study, we describe the expression of PD-1 and its prognostic significance and association with clinical features in patients with ccRCC.
Materials and Methods
Patients and clinicopathological data. By reviewing electronic clinical charts, we obtained clinicopathologic data of ccRCC patients at Gyeongsang National University Hospital, Jinju, Korea between January 2000 and December 2009. One hundred sixty-six patients with ccRCC were enrolled in this study. The tumors were staged according to the guidelines of the eight edition of the American Joint Committee on Cancer tumor-node-metastasis (TNM) staging system. Recurrence was diagnosed by surgical biopsy or radiologically. Disease-free survival (DFS) was defined as the period from the date of the surgery to the date of cancer recurrence. Disease-specific survival was defined as the period from the date of the surgery to the date of death due to ccRCC.
Two pathologists reviewed hematoxylin and eosin-stained glass slides. This study was approved by the Institutional Review Board of Gyeongsang National University Hospital with a waiver of informed consent (GNUH 2020-04-006).
Tissue microarray. Specimens were obtained surgically and fixed overnight in neutral buffered formalin (20%). The samples were embedded in paraffin blocks. Two cores of 2-mm representative tissue were collected from each paraffin block and transplanted onto new recipient tissue microarray (TMA) blocks. Two cores were collected from the center and periphery of the tumor.
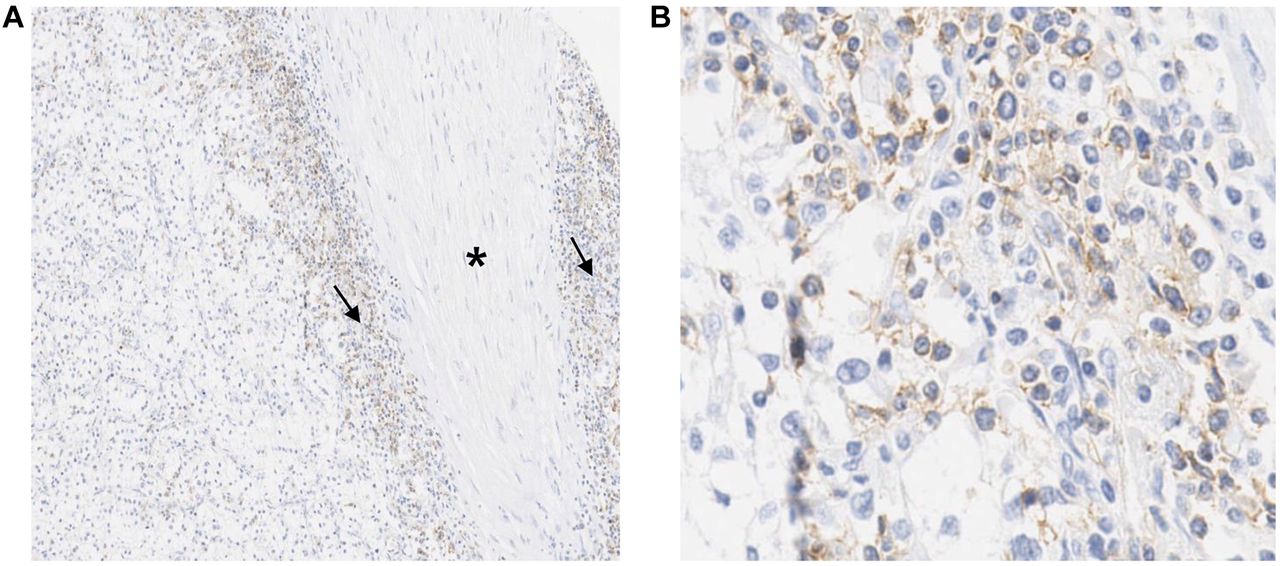
Immunohistochemical analysis. Primary antibodies against PD-L1 (1:200, ElL3N, Cell Signaling Technology, Danvers, MA, USA) and PD-1 (1:100, ab52587, Abcam, Cambridge, UK) were used to evaluate protein expression. The immunohistochemical (IHC) method is described in our previous report (20). PD-L1 scoring (SP142) was based on the percentage of PD-L1-expressing tumor cells or inflammatory cells with any intensity (21). To increase the reproducibility, we evaluated the intensity of PD-1 expression of membranous staining on tumor cells and inflammatory cells simply as negative or positive for any percentage (Figure 1).

PD-1 expression in ccRCC. (A) PD-1 positive inflammatory cells are infiltrating the tumors (arrow) around the fibrotic band (star) (Original magnification ×100). (B) PD-1 staining of inflammatory cells shows membranous pattern. (Original magnification ×400). PD-1: Programmed death protein 1; ccRCC: clear cell renal cell carcinoma.
Statistical analysis. The correlation between PD-1 expression and clinicopathological parameters was analyzed by using chi-square tests. The prognostic significance of the clinicopathological data for DFS and DSS was evaluated by Cox proportional hazards regression analysis. Survival probability was also analyzed by the Kaplan-Meier method with the log-rank test for DFS and DSS. The results were considered statistically significant when the p-value was less than 0.05. SPSS version 21.0 (IBM Corp, Armonk, NY, USA) was used for the analysis.
Results
Clinicopathological data. The clinicopathological data of patients with ccRCC (n=166) are summarized in Table I. The mean age of the patients was 59 years (range=32-84 years). There were 124 (74.7%), 12 (7.2%), 26 (15.7%), and 4 (2.4%) patients with T stage 1, 2, 3 and 4 disease, respectively. The Fuhrman nuclear grades were as follows: 30 (18.1%) were grade 1, 110 (66.3) were grade 2, 20 (12.1%) were grade 3, and 6 (3.6%) were grade 4.
Clinicopathological information of 166 patients with clear cell renal cell carcinoma.
PD-L1 and PD-1 expression. Of the 332 cores, 58 cores had hemosiderin pigment or artificial brown pigment, and one core was not available due to loss of the specimen. In total, 59 cores were not informative. Ultimately, 273 available cores were used for the analysis.
Of the 273 cores evaluated, 123 showed PD-1 expression in inflammatory cells and no PD-1 expression in tumor cells. No cores showed PD-L1 expression in tumor and inflammatory cells. The positive control for PD-L1 showed high expression. PD-1-positive inflammatory cells showed a membranous staining pattern.
Relationship between PD-1 expression and clinicopathological data. The relationships between PD-1 expression and clinicopathological data are shown in Table II. PD-1 expression was significantly related to male sex (p=0.046) and T stage=1 (p<0.001) but not to age (p=0.597) or Fuhrman nuclear grade (p=0.086).
Correlations among clinicopathological factors and PD-1 expression.
PD-1 expression and survival analysis. Univariate and multivariate analyses of survival according to PD-1 expression in 273 available cores are shown in Table III. In the univariate analysis, several variables were associated with poor DFS, including age ≥60 (p=0.001), Fuhrman grades 3 and 4 (p<0.001), T stage ≥2 (p<0.001) and PD-1 expression (p<0.001). Poor DSS was also associated with age ≥60 (p=0.021), Fuhrman grades 3 and 4 (p<0.001), T stage ≥2 (p<0.001) and PD-1 expression (p=0.002). Moreover, multivariate analysis revealed that PD-1 expression was an independent factor for unfavorable DFS (hazard ratio=2.171; 95% confidence interval=1.103-4.275; p=0.025).
Cox proportional hazards analysis of PD-1 expression in 273 available cores.
Discussion
Tumors are usually infiltrated by inflammatory cells. The composition of inflammatory cells and the number of each subtype differ between different tumors. These inflammatory cells interact with each other and affect the growth of tumors. In addition, these inflammatory cells can be related to a good prognosis or a poor prognosis in patients (22). Tumor microenvironments are mostly composed of tumor-infiltrating lymphocytes including CD4+ and CD8+ T cells (23). These T cells are regulated by positive and negative signals (24). Among inhibitory immune checkpoint proteins, PD-1 and PD-L1 have been actively studied, and their relationships to cancer, infectious disease, transplantation, and autoimmunity have been demonstrated (25-27). For example, a strong correlation between PD-1 and PD-L1 expression and prognosis in cancer patients has been actively demonstrated (8, 11, 12, 15, 16, 25).
Additionally, there has been significant research on PD-1 and PD-L1 and ccRCC. Usually, PD-L1 is expressed in both immune cells and tumor cells, while PD-1 is mainly expressed in tumor infiltrating lymphocytes (28). Many previous reports have also shown that PD-L1 is an independent poor prognostic factor for ccRCC (16, 17, 19). However, previous studies on the correlation between PD-1 and ccRCC are limited and controversial. Stenzel et al. (19) reported that high PD-1 expression in inflammatory cells is significantly associated with favorable cancer-specific survival. In contrast, Ueda et al. (16) reported that PD-1 expression is significantly associated with adverse outcomes in metastatic ccRCC.
Our results showed that PD-1 expression was significantly correlated with male sex and higher T stage. PD-1 expression was related to unfavorable DFS and DSS in the univariate analysis of patients with ccRCC. Moreover, PD-1 expression was related to unfavorable DFS in multivariate analysis in patients with ccRCC. Based on our results, we hypothesize that PD-1 expression inhibits T cell-mediated antitumor responses in ccRCC. This finding suggests that PD-1 pathway blockade will enhance antitumor effects in ccRCC.
Our study has limitation. Tissue microarray is a valuable technique evaluating immunohistochemical markers in tumors and used as an alternative for whole tissue sections (29). However, the possibility of intratumoral heterogeneity in biomarker expression is concerned in small tissue microarray specimen (30). There have been a few studies on PD-L1 expression and heterogeneity. Intratumoral and intertumoral heterogeneity was present in more than half of the cases (31). However, to our knowledge, there have been no studies on the intratumoral and intertumoral heterogeneity of PD-1 expression in inflammatory cells. Therefore, further studies of PD-1 expression in ccRCC with whole tumor sections are needed.
Conclusion
This study showed that PD-1 expression in tumor infiltrating inflammatory cells serves as an independent factor for unfavorable DSS in patients with ccRCC.
Footnotes
Authors’ Contributions
MHK and DHS conceived and designed this study. MHK, GHK, JHL, JSL, DCK, JWY, JMN, HJA and DHS collected samples, performed pathological diagnosis and analyzed the immunostained samples. MHK and DHS analyzed all the data. MHK and DHS wrote the first draft of the manuscript. GHK, JHL, JSL, DCK, JWY, JMN, HJA and DHS critically reviewed and corrected the manuscript. All Authors reviewed and approved the final version of the manuscript.
This article is freely accessible online.
Conflicts of Interest
The Authors declare that they have no competing interests in relation to this study.
- Received March 3, 2021.
- Revision received March 18, 2021.
- Accepted March 22, 2021.
- Copyright© 2021, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.