


Abstract
Background/Aim: Neurofibromatosis type 1 (NF1) is an autosomal dominant tumour predisposition syndrome that can cause plexiform neurofibromas (PNFs). This study examines the surgical procedures that have been performed on large PNFs of the lower extremities. Patients and Methods: Surgical procedures on the lower extremity performed on 90 patients with NF1 with PNFs were evaluated. The topography of the tumours was classified according to dermatomes and functional units. Results: A total of 243 surgical interventions on the regions of interest were performed. Neurological complications were rarely noted and usually occurred temporarily. There was no preference for dermatomes affected by PNF. The proportion of patients with malignant peripheral nerve sheath tumours (MPNSTs) in this group was 4/90 (4.4%). Conclusion: PNFs often require repeated local interventions to achieve the treatment goal. Local tumour recurrences are to be expected even after extensive tumour reduction. Rapid tumour growth combined with new pain sensations can be signs of a MPNST.
- Neurofibromatosis type 1
- buttocks – surgery
- lower extremity – surgery
- foot – surgery
- plexiform neurofibroma
- MPNST
- peripheral nerve sheath tumour
The autosomal dominant transmitted hereditary disorder, neurofibromatosis type 1 (NF1), develops with relative frequency in humans (1-5). NF1 is a tumour predisposition syndrome (6, 7), with individuals affected carrying a substantial risk of developing tumours of neurogenic origin (1), in particular peripheral nerve sheath tumours (PNSTs). The tumours are usually large in number (8) and termed neurofibromas (9). The most frequent PNST in NF1 is cutaneous neurofibroma (CNF) (9). This type of neurofibroma causes primarily aesthetic problems due to the large number of mushroom-like tumours arising in the skin (10, 11).
In contrast, another type of nerve sheath tumour in patients with NF1 arises from larger nerve trunks or covers large areas of the skin and invades the subcutaneous tissue (12, 13). In addition to the aesthetic impairment, these tumours often also result in functional deficits (14-16). The tumours are very likely congenital in origin and are termed ‘plexiform neurofibromas’ (PNFs) (12, 13), which constitute one out of six clinical findings allowing the diagnosis of NF1 (11). The term is derived from characteristic histological findings (17). PNF is a characteristic tumour in NF1, which is identified in about 30% of patients. Indeed, sporadic PNF is a very rare diagnosis. A finding of sporadic PNF without further diagnostically relevant features of NF1 may represent the so-called segmental type of the disease (18-22). In a large, unicentric study on the surgical treatment of PNSTs, benign, sporadic neurofibromas were the largest diagnostic group (21). Therefore, in order to characterize a study group for the treatment of PNSTs, information on the genetic background of the tumour disease is important. PNF is regarded as a precancerous lesion, potentially giving rise to a malignant peripheral nerve sheath tumour (MPNST) (21-26). NF1 is the most common inheritable disease with a predisposition to cancer development.
Surgery is the most effective measure to treat patients with PNFs (25-30); however, due to the large extent of many PNFs, complete resection of the lesions is hardly feasible (30). PNFs are slowly growing lesions that can develop significant increases in volume (31). A particularly striking shape of PNF growth is the tumour-associated enlargement of an extremity or parts of it. This phenotype has been described as ‘elephantiasis neuro(fibro)matosa’ (32, 33). Alternatively, enormous neurofibromatous tumours are also termed ‘massive soft tissue neurofibromas’ (17). This tumour type appears to be restricted to generalized NF1 (17, 34-42) and is often highly vascularized (43). The massive tumour rarely develops into a MPNST (17, 44, 45). On the other hand, the large volume of tumours is the prerequisite for unnoticed growth of malignant tumours. PNF in association with NF1 may develop with variable extension and size in the buttocks, legs and feet (17). Many reports have been published on the diagnosis and treatment of PNF in NF1 and have been presented as case reports or clinical studies (46-79). The aim of this study is to contribute to the classification of surgical interventions for PNFs in the region of the buttocks, legs and feet, by analysing clinical data. This information may contribute to improving the treatment process in affected patients.
Patients and Methods
Patient population and study material. The archive of surgical reports of the senior author was searched for the operation reports of patients with neurofibromatosis undergoing surgery on the buttocks and lower extremities. All these patients have been operated on by the senior author in the Department of Oral and Craniomaxillofacial Surgery, Eppendorf University Hospital in Hamburg, Germany. The surgical interventions took place between the spring of 1990 and April 2017. Patients were excluded if they had been affected by NF2 or schwannomatosis (11). The patients participating in this retrospective study all fulfilled the diagnostic criteria for NF1 (80, 81). The first sighting of files provided 235 patients with appropriate information on the timing and location of the procedure and diagnosis. Of these 235 patients with NF1 operated on for NF1-associated pathologies of the leg, foot, buttocks or inguinal area, a total of 90 patients with the plexiform type were selected and included in the study. In the remaining 145 patients who were not operated on for a PNF, the main reasons for surgery were excision of (multiple) CNFs or iliac crest biopsy/graft associated aesthetic and reconstructive measures. All paper files were subsequently ordered and checked, digital files examined, digital photographs viewed and photos on celluloid (slides) screened.
One patient had changed their sex from male to female. Since the patient was last operated on as a man with regard to PNF treatment and gender transformation took place later, the patient was included as a ‘male’ in the statistical evaluation. Another patient had developed squamous cell carcinoma of the sole of the foot. This patient had no PNFs in the affected region of the body and was excluded from further evaluation (82).
The following data were collected from these 90 patients for further calculations: i) date of birth, ii) gender, iii) affected body side (right, left or bilateral), iv) neurofibroma surgery in other parts of the body, v) diagnosis of malignancy (MPNST), vi) elephantiasis neuro(fibro)matosa, vii) age at the first surgical intervention in the hospital, viii) date of surgery, ix) duration of operation, x) number of interventions in the region of interest per individual, xi) recording dates for inpatient stay and discharge (duration of stay in hospital), xii) pathological findings, xiii) blood transfusion(s) and xiv) complications related to surgery (Tables I and II). The external size of the lesions was determined on the basis of operation reports and photo documentations. Reports of diagnostic imaging [magnetic resonance imaging (MRI) and computed tomography (CT)] were used to further specify the findings.
Classification of complications related to surgical intervention.
Classification of histological findings of tumours.
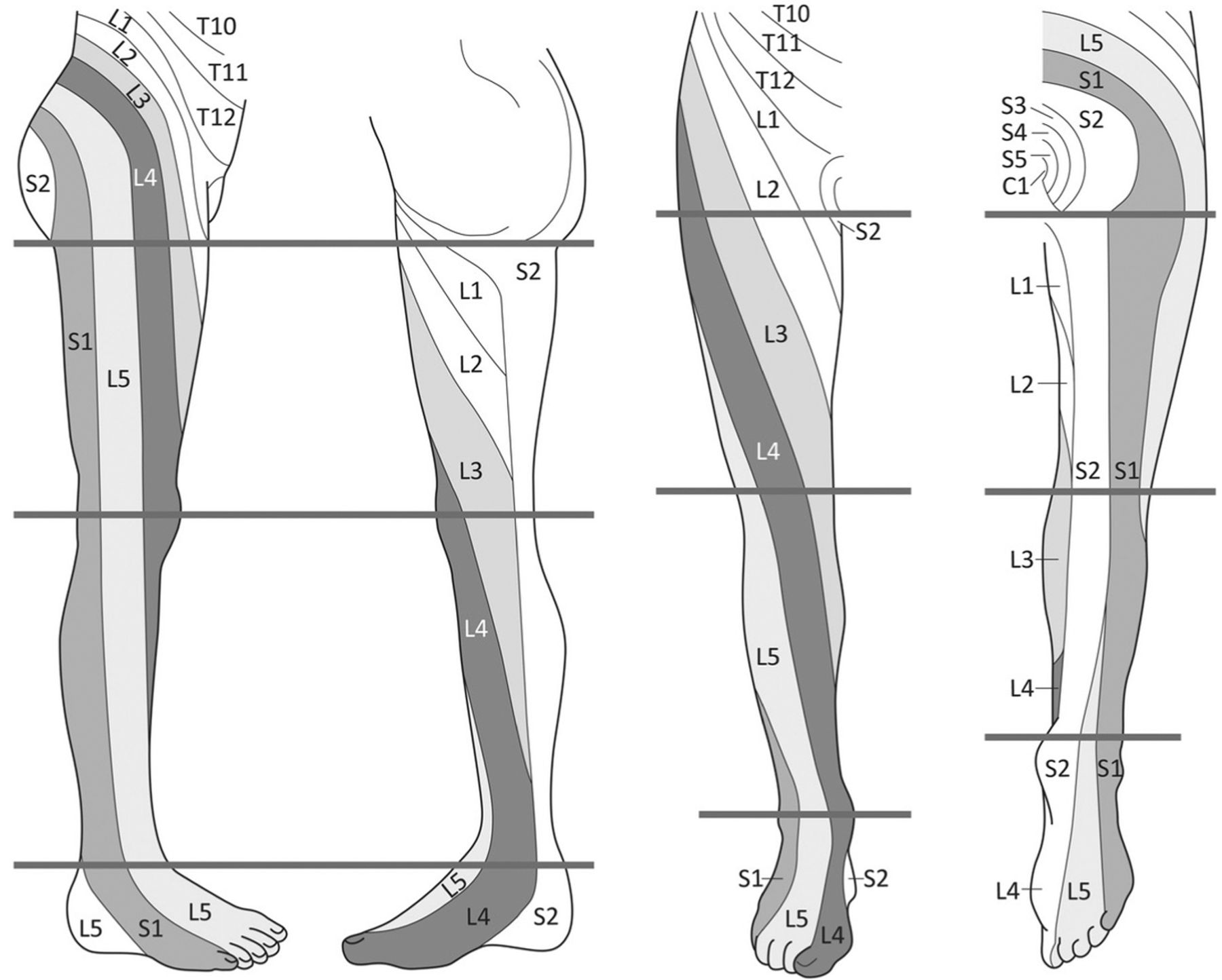
Diagnostic subdivision of the regions into anatomical and functional units. The distribution pattern of dermatomes used for this study was according to Keegan and Garett (83) (Figure 1). Dermatomes are classified according to their sensitive radicular innervation. However, we knew from previous investigations (45) that assignment of tumour extension to dermatomes can cause considerable inadequacy in the graphical representation of tumour spread, because firstly, the tumours may spread out over a wide area and often grow horizontally, which means that they develop perpendicular to the dermatome of the extremity. Secondly, the dermatomes in the regions of interest are of very different sizes, so no estimation about the area and size of the tumour is possible with reference to the assignment to a dermatome. Thirdly, due to the original segmental structure of the dermatomes, some dermatomes are localized close together and narrowly limited, so tumours in this region very easily infiltrate several dermatomes, even if they are small in size. In contrast, tumours of the same size affect only one or a few dermatomes elsewhere (and then dermatomes may be only partially tumorous). Despite these evident weaknesses in the classification of tumour extension according to dermatomes, this determination method was used to obtain an initial estimate of the distribution and extension of the lesion in the region of interest. The measurements can provide some information on the treatment needs of the patients.

Classification of dermatomes. Image adapted from Keegan and Garett 1948 (83), supplemented by a classification of the region of interest defined by functional levels (horizontal lines). The abbreviations indicate the assignment of the skin areas to the respective spinal nerves. T: thoracic; L: lumbar; S: sacral; C: coccygeal.
Since a descriptive anatomical classification according to the affected skin area is obviously of limited value for determining the extension of tumours, a functional classification, according to the vertical level of the limb, was chosen as an alternative. This classification of the lower extremity tumour extension by levels defines tumour extension by arbitrarily drawn horizontal lines, according to the long axis of the extremity (Figure 1). The classification of tumour extension according to levels allows combinations of levels if the tumour exceeds the defined limits. A three-digit alphanumeric code is used for describing the affected region and dermatome. The first of two letters mean: G=gluteal, U=upper (leg), L=lower (leg) and F=foot. The second letter indicates the spinal nerves of the respective skin area: L=lumbar and S=sacral. The third letter of the code is a number that refers to the respective spinal nerve(s).
Data registration and statistics. An evaluation sheet was developed for data collection of each patient. The evaluation sheet was used both for the analysis of paper and digital files and photographs of the lesions. An examination form was completed for each surgical procedure. For this purpose, the local findings were recorded according to both dermatome and level, then numerically coded for further data processing. The data concerning surgical complications and histological findings were further differentiated and transformed into numerical codes (Tables I and II). Subsequently, the results were summarized in an Excel sheet and evaluated using software SPSS™ (Version 24) (IBM, Armonk, NY, USA) and STATA™ (Version 14) (StataCorp, College Station, TX, USA) for statistical computing. The chi square test was used to determine differences, and regression equations were used to uncover correlations. A p-Value<0.05 was defined as statistically significant.
Ethics. This study was accepted by the local authority of Eppendorf University Hospital (appointed by the University of Hamburg) as a prerequisite for the preparation of a medical dissertation in dentistry (CTT). All patients gave informed consent regarding the scientific evaluation of medical data prior to their treatment in the hospital. All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Data were anonymized prior to analysis, and the investigators studying the radiographs were blinded as to the diagnosis, identity of individuals, and assignment of the single case to a diagnostic group. These investigations were carried out in accordance with the Hamburg Health Service Act (Hamburgisches Gesundheitsdienstgesetz). This type of study does not require an ethics vote.
Results
Gender. Thirty affected men and 60 affected women were recorded and statistically evaluated.
Age at the first operation. The age range was between 1 and 61 years [male: 1-61 years (yrs), mean±SD=31.57±18.97 yrs; female: 5-60 yrs, mean±SD=26.35±12.14 yrs].
Body side. The location of the nerve sheath tumours was recorded with reference to body side. In some patients, the predominantly unilaterally growing PNF exceeded beyond the midline of the body, preferentially identified in lesions arising in the buttocks. This finding was considered a bilateral spread of the PNF. Thirty-eight patients (42.2%) were affected on their right side, and 32 patients (35.6%) were affected on their left side. There were 20 patients (22.2%) with a continuous spread of the lesion to both halves of the body.
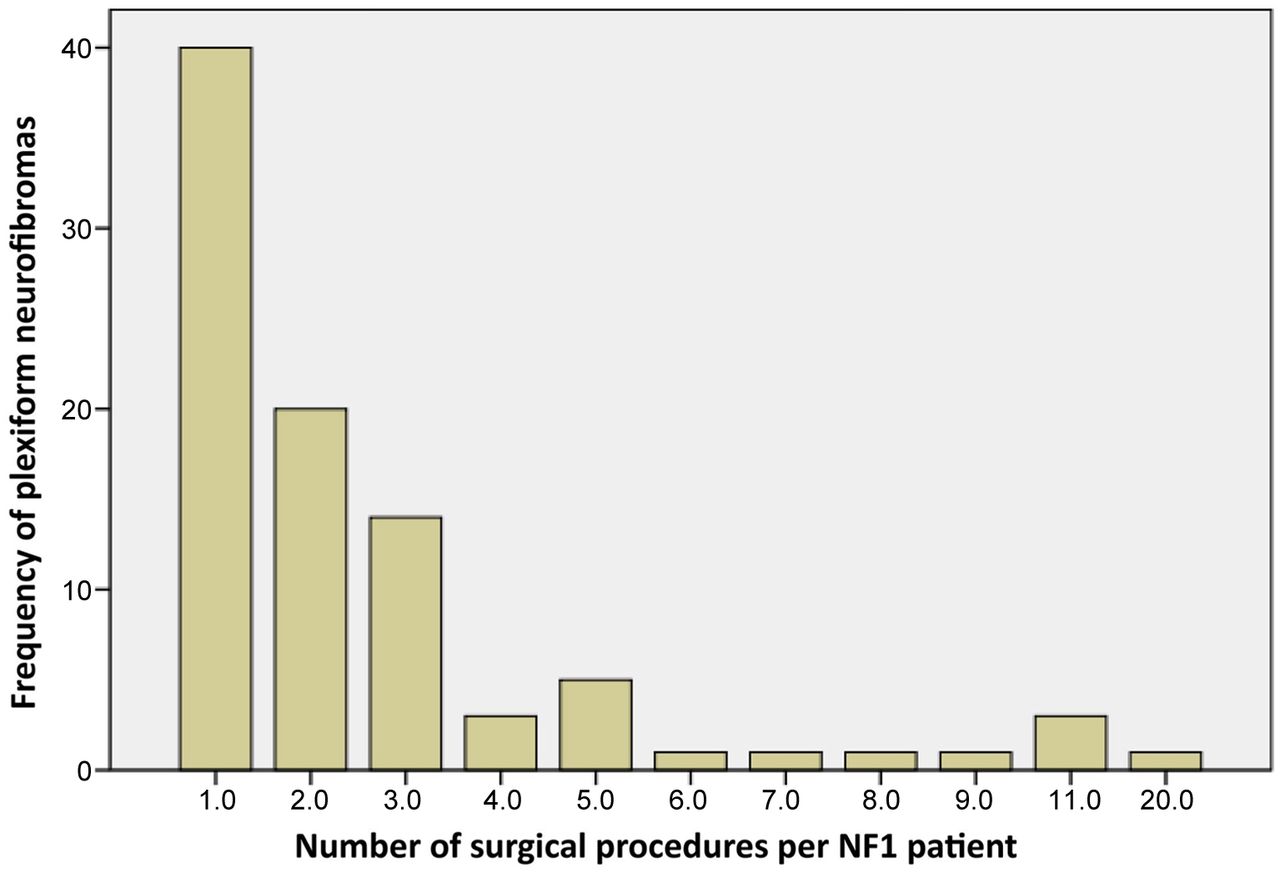
Number of surgical interventions per patient. Most patients were operated on 1-3 times but exceptions were not uncommon. On average, a patient experienced surgical procedures in the region of interest about 2.7 times. Forty patients (44.4%) had surgery only once. Table III and Figure 2 show the distribution of number of procedures and patients (minimum=1, maximum=20, mean±SD=2.69±2.93, median=2).
Number of surgeries for NF1 patients with plexiform neurofibromas.

Graphical description of number of surgeries for NF1 patients with plexiform neurofibromas.
Blood transfusion. Most patients were treated without the need for blood substitution [86 patients (95.6%)]. Only four patients (4.4%) needed this measure. Out of 243 surgical interventions, blood transfusions were performed 18 times, corresponding to 7.41% of all surgical procedures [no transfusion in 225 procedures (92.59%)]. It is noticeable that a small group of patients (extensive tumours, necrotizing MPNST) more often required a blood transfusion, while the majority of patients did not need this measure.
Duration of surgical procedures. A single procedure lasted 63.45 minutes on average (minimum: 10 min, maximum: 180 min, median±SD=56±33.1 min, n=243 procedures) (Figure 3).

Duration of plexiform neurofibroma surgeries. (Mean±SD: 63.45±33.096; N=243).
Complications. Table IV shows the relationship between complications in terms of number of patients (n=90). No complications were recorded during the treatment of 63 patients (70%). Sixteen patients (17.8%) had some oozing blood, 4 patients (4.4%) had wound healing disorders, while in 3 patients (3.3%) a hematoma had to be drained and two patients (2.2%) had a wound infection. Only one patient (1.1%) had a revision surgery. A total of 182 of all operations (74.9%) took place without complications.
Type 1 neurofibromatosis patients affected by complications that occurred during surgery or post-surgery following debulking procedures for large plexiform neurofibroma. Complication rate in relation to the number of patients (N).
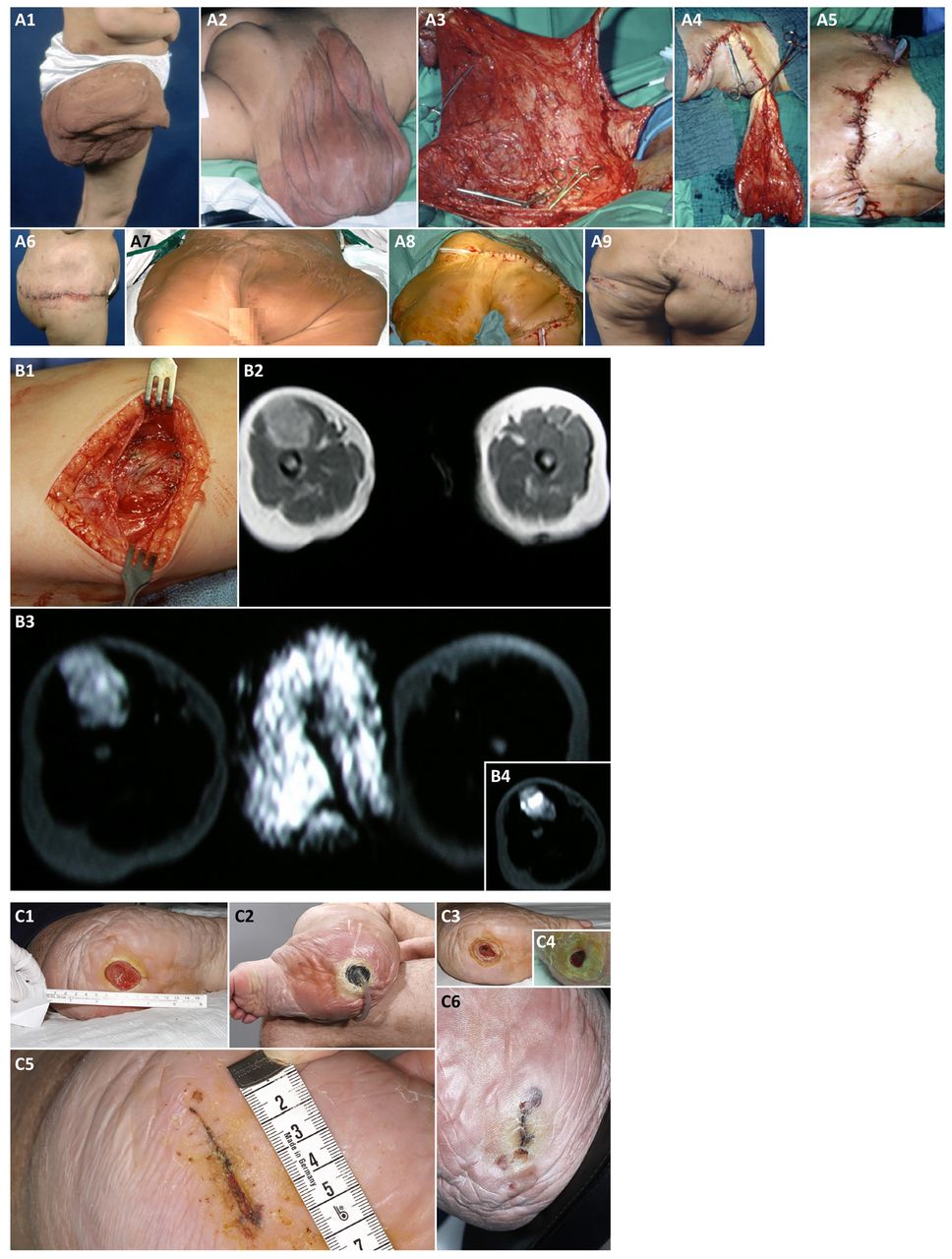
Out of a total of 243 procedures, 37 (15.2%) were associated with regular oozing bleeding. Of these, 14 operations (5.8%) were associated with a wound healing disorder, 5 (2.1%) were caused by a need for hematoma drainage, 3 (1.2%) were caused by wound infection and one (0.4%) was a revision surgery (Table V). In one case, the peroneal nerve was damaged as a result of the resection of a large, nodular PNF of the buttocks. The tumour had grown within a short period of time, causing considerable pain, causing inability to take a pain-free sitting position, impairment of driving a car and restricted movement of the affected leg. The operative site shows the large tumour with peripheral nerve growing into the lesion (Figure 4A). The case is unusual in that the patient with genetically confirmed NF1 was missing all the cutaneous stigmata of the disease at the time of tumour resection. The patient had developed multiple PNFs that were distributed deep in the body and continued to increase in number and size over time (follow-up: 20 years). Some of these nodular neurofibromas were removed and identified as PNFs. During this long follow-up period, the patient also developed few CNFs at different body sites.
Type 1 neurofibromatosis patients affected by complications that occurred during surgery or post-surgery following debulking procedures for large plexiform neurofibroma. Complication rate in relation to the number of interventions (N).

Plexiform neurofibroma phenotypes. A1-A5: Painful, rapidly growing tumour of the buttocks. A1-A2: MRI shows nodular mass of right side of buttocks with inhomogeneous internal enhancements (arrows) of the tumour in axial and coronal sections. A3: The nodular tumour was resected in toto. A4: A nerve inserts into the tumour, in which the strand-like structure (arrow) cannot be further identified. A5: The incised tumour is solid and shows inhomogeneities in the tissue distribution, but no visible necrosis. B1: Small-size plexiform neurofibroma of the leg. B2: Large tumour resection specimen of the leg. B1 is a 2×2 cm neurofibroma taken from the right dorsal lower leg and B2 is about a 30×15 cm piece of tissue that was excised from the left dorsal thigh. Both specimens were histologically diagnosed with diffuse plexiform neurofibroma (WHO grade 1).
Hospitalization. In the total of 243 surgeries, the shortest hospital stay was 3 days and the longest hospital stay was 88 days. The arithmetic mean was 15.72 days (SD=13.51; median=11 days) (Figure 5).

Duration of hospital length of stay following plexiform neurofibromas surgery.
Elephantiasis neuro(fibro)matosa. Thirty patients were classified as suffering from elephantiasis neuro(fibro)matosis. Only the diagnoses from the written paper documents and digital files were considered. In comparison to photographs showing findings prior to the intervention and during the surgical procedure, the term describes tumours spreading like lumpy masses, extending from one or more body levels and having caused a noticeable deformation of the body region. The term is an imprecisely used qualitative judgment, which is mainly used for diffuse PNFs. A more precise description of the structure of the body region (e.g., asymmetry of the skeleton) is not associated with the metaphorical terminus. Elephantiasis in connection with the planning of the procedure addresses a large, spreading tumour, however, without further specification of the finding. The somewhat more abstract term ‘massive soft tissue tumour’ (17) fully corresponds to the descriptive term ‘elephantiasis’.
Pathology. Table VI indicates all pathological findings of patients with NF1. As already detailed, the pathological findings were divided into six different diagnoses, of which PNF was the most frequently diagnosed type in 43 patients (47.8%), followed by dermal diffuse neurofibroma in 24 patients (26.7%), and MPNST in four patients (4.4%). Four other patients (4.4%) had atypical neurofibroma, one tumour was a lipoma (1.1%), four patients (4.4%) had a PNF with a schwannoma in the neurofibroma and in 10 patients (11.1%), the pathological findings were inconclusive or missing.
Histology of peripheral nerve sheath tumours of NF1 patients (Institutes of Pathology and Neuropathology, UKE).
The histological finding of PNFs differs from the clinical use of the term PNF in the sense of describing a large tumour mass with diffuse infiltration of the skin, subcutaneous tissue and possibly the muscles. Therefore, the histological findings were evaluated. This shows that there are clear differences between the clinical assessment of the lesion and the histological findings. Furthermore, the histological diagnosis has no correlation to the macroscopic extent of the tumour but to the texture of the tissue. The comparison of visible tumour size and histological tumour diagnosis shows that the independence of both characteristics has a significant impact on the topographical scale used in the evaluation (i.e., the dermatome infiltrated by the tumour). Here are photographs of two surgical specimens of two different patients that are very different in size to illustrate the divergence of macroscopic and microscopic aspects (Figure 4B).
Affected dermatomes of the whole group. A total of 6,318 individual dermatomes in the various body regions were counted and evaluated (Table VII). In 3,872 dermatomes, the corresponding areas were not affected by a PNF (61.3%). The number of affected dermatomes was 1,536 (24.3%) (Tables VIII, IX, X). However, in 910 dermatomes (14.4%), no corresponding tumour localization could be made due to insufficient visual representation of the tumour region on photographs. The dermatomes in the buttock area were largely equally affected (Tables VIII and Table IX, Figure 6).
Total number of individual dermatomes from operations of NF1 patients with plexiform neurofibroma.
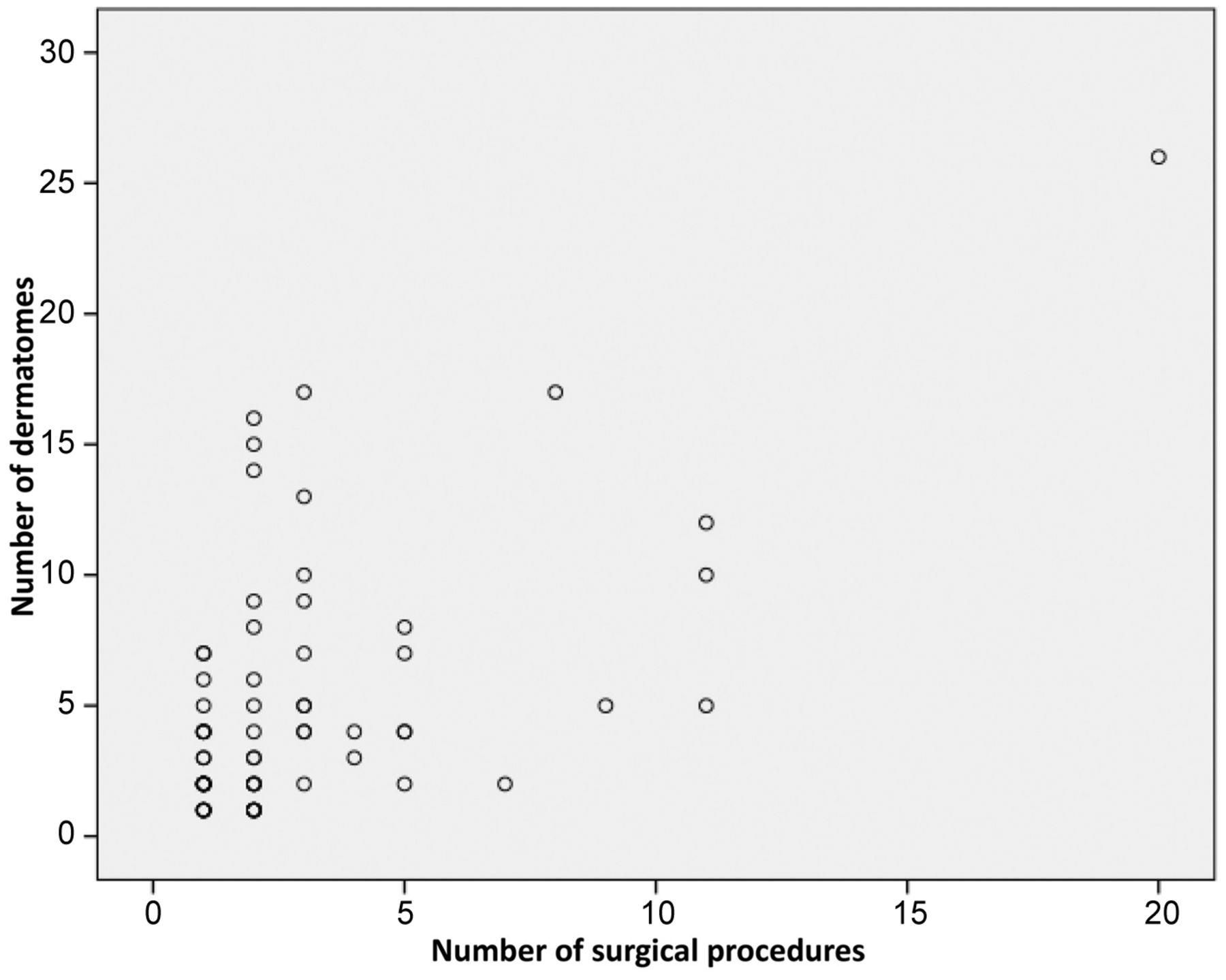
Scatter diagram for the number of dermatomes with respect to the number of operations.
Number of not-affected dermatomes in NF1 patients subjected to surgical procedures of the gluteal region, lower extremity and foot.
Number of affected dermatomes in NF1 patients subjected to surgical procedures of the gluteal region, lower extremity and foot.
The segmental structure of the skin innervation was precisely mapped (85, 86), but the individual sensitive innervation fields showed very large differences. Tumour extension hardly fit into the skin regions assigning the developmental history of the peripheral nervous system in terms of affected dermatomes. Overall, the frequency proportions of the dermatomes of the investigated body regions affected by a PNF vary only within a narrow range. The investigation revealed a largely uniform distribution of tumour spread in relation to the dermatomes, and, thus, the random distribution of somatic mutations that cause the development of the tumours.
Levels. The classification of the tumour locations according to level also showed the frequent need for the treatment of tumours in the gluteal region (about 40%, Figure 7). On the other hand, locations, such as the foot and upper leg were also very often affected when all patients with tumours from this region were included (Table X). All in all, the classification of tumours by level showed the well-known invasive growth, which can be descriptively assigned to a specific region of the body.

Bar graph indicating the frequency of the plexiform neurofibroma affected levels and level combinations. G: gluteal region; U: upper leg; L: lower leg; F: foot.
Frequency of NF1 patients by localization of the plexiform type of neurofibromatosis type 1 affected topographic areas (levels) and level combinations (buttocks, legs and feet).
Correlation analysis. The number of affected dermatomes varied considerably (minimum: 1, maximum: 26; mean±SD=5.03±4.85, median: 4). However, correlation analyses revealed that the number of dermatomes and indication for blood transfusion were associated and had a statistically significant impact on surgical treatment (Tables XI, XII, XIII). The indication for blood transfusion influenced the duration of surgery. For example, if there was a blood transfusion, the surgical procedure lasted, on average, 36 minutes shorter than if there was no transfusion. This correlation shows that the surgical concept aimed to ensure local wound control and adapt the surgical measure accordingly, especially through repeated tumour reductions, to allow for easier control.
Linear mixed model to study impact factors on the duration of surgical intervention with patients as random factors.
Examination of various criteria in comparison to the number of dermatomes.
Factors influencing the number of dermatomes in NF1 patients.
The number of dermatomes had an influence on the duration of surgery (Figure 3). For example, with each dermatome, the duration of surgery increased on average by 1.7 minutes. This proved a linear relationship between the area and the operating time. No other factors had a significant effect on the duration of surgery (p>0.05).
Malignancy (MPNST). A total of four patients were diagnosed with MPNST. Of these four patients, the legs of three patients were amputated during the course of disease. Two of these patients survived. In all four patients (4.4%), an extensive PNF had transformed to malignancy (MPNST). In 86 patients (95.6%), there was no malignancy in the region of interest. Two patients have developed a MPNST later during the course after reducing a PNF in the study area. One patient came to the hospital with an already confirmed diagnosis of MPNST. One child, who was diagnosed with MPNST for the first time and was not subjected to further surgical measures following diagnostic exploration, underwent multiple rounds of chemotherapy and died 2 years later with a diagnosis of tumour progression at the age of 5 years.
Neurofibromas in other parts of the body. Of the 90 patients examined, 52 (57.8%) had neurofibromas manifested not only in the lower extremities but also in other parts of the body. Large PNFs growing in continuity from the lower trunk to the gluteal region were included in the ‘gluteal’ region and thus not considered for registration of tumours in other body regions. Neurofibromas in other parts of the body were registered irrespective of neurofibroma type. Surgery for PNFs in the buttocks or legs was the only surgical procedure for treatment of PNST in 38 patients (42.2%). Figure 8 illustrates some findings and surgical procedures.

Case survey of three NF1 patients (A, B, C). A1-A9) Patient with extensive tumour masses of the buttocks on both sides. A3-A5) Tumour reduction and coverage of the wound surface with Z-flaps (here: right side). A6) Regular wound healing. A7-A9) Corrective intervention fifteen years later due to recurrent tumour growth and sagging of the soft tumour masses caudally. B1-B4) Thigh tumour in a small child with NF1. B1) The massive tumour had grown firmly attached to the surrounding connective tissue. B2-B4) Magnetic resonance imaging shows the continuous transition of the lesion into the skin layers and the inhomogeneous structure of the lesion. The diagnosis of the lesion was malignant peripheral nerve sheath tumour. C1-C6) Impaired wound healing following tumour reduction of the lower leg alio loco. The ulcer did not heal and enlarged in diameter due to functional stress on the foot. C2-C5) Negative pressure conditioning of the wound was carried out over several weeks. With this measure, the defect in the sole of the foot was considerably reduced (C3-C4), so that the wound could definitely be closed by approximating the skin edges (C5-C6).
Discussion
The study presents the clinical data of long-term care for patients with NF1 who have been surgically treated for extensive tumours of the buttocks, legs and feet (30). The data can be used to orient treatment plans for patients with this phenotype.
Gender. The motivation for choosing surgical measures for patients was either the clarification of the biological characteristics of the lesion or the functional and aesthetic improvements of the tumorous region. The literature on surgery in NF1 gives no evidence of gender dimorphism of PNFs arising in the lower extremity and buttocks.
Age. The average age of men at the first operation is approximately 31.6 years and of women 26.4 years. The age difference is probably due to the earlier assessment of women and that an attempt at treatment is preferable to a wait-and-see attitude. However, these assessments should be checked by analysis of the age structure of patients with this diagnosis, phenotype and treatment request from other centres. The age structure of surgically treated patients with NF1 changes significantly when analyses for the treatment of bone asymmetries of the extremities and pseudarthroses are presented, in particular in children (27, 29) and in studies on MPNST in NF1 (25).
Topography. The findings disclose the irrelevance of body side in the development of PNFs. PNF can arise bilaterally in an individual. In these cases, the buttocks usually were affected and the extension of the tumours to both branches of the trunk was not symmetrical. In fact, a symmetrical expansion of the tumours could only be assumed if the tumours had developed relatively narrowly around the median sagittal plane and were of small size. Neurofibromas in the area of the anal cleft or in the area of the mons pubis that overlap on both halves of the body were also evaluated as arising on both sides. Bilateral PNFs occurring separately on both sides of the lower body region (legs) were rarely recognized.
When discussing the laterality of the neoplasm, it is necessary to point out that the surgical interventions were predominantly in diffuse PNF tumour type. As is well known, there are patients with NF1 with nodular PNFs affecting a body part or even the whole body. These tumours develop deep in the body, arise in larger nerves or plexus, do not have to grow into a disfiguring tumour mass and may completely escape view from the outside (15, 16). However, this nodular type of tumour can occur singularly or as multiple findings within larger diffuse PNFs (45). The alternative term for the NF1-specific tumour spread is massive soft tissue neurofibroma (17), which is the object of this investigation. It has been explicitly pointed out that all variants of PNSTs can be detected in this type of tumour (17); however, it was emphasized that the development of a MPNST is rarely observed with this manifestation. On the other hand, two out of four MPNSTs in this study developed in massive soft tissue tumours.
The MRI-based differentiation of large PNSTs (collectively referred to as ‘plexiform’) into those with superficial, nodular or invasive growth patterns, is a helpful imaging classification for assessing tumour biology and planning surgical measures (15, 16, 45). Despite this, the image-based morphological classification has no correlation to the histological findings, in particular to subtyping of diffuse PNF.
Histological diagnosis: Nomenclature. The macroscopic finding of a PNF with extensive lobular spread in the skin and subcutaneous tissue may differ from the histological assessment (17). Histological diagnosis may be a diffuse PNF. A diffuse neurofibroma with a rather superficial spread potentially will be easy to treat in the case of limited extension. Therefore, the practitioner must be aware that the histological diagnosis is different from the clinical estimation in some cases. Tumour size does not play any role in the histological diagnosis of PNF (67); however, the histological finding, especially in the case of extensive tumour masses, is always the inductive conclusion, which infers from individual specimens to the characteristic of the totality of the lesion (45).
The majority of PNFs presented here corresponds to plexiform and diffuse PNFs in the microscopic assessment. Topographically, the tumours have either grown to a variable extent in the skin and subcutaneous tissue or have expanded diffusely and invaded into the deeper layers of the organs. The transition from diffuse PNF to elephantiasis neuro(fibroma)matosa is gradual. Local hyperplasia of the long bones with the consequence of asymmetrical extremities is a finding that occurs especially in diffuse PNFs.
Histological diagnosis: Schwannoma in NF1. In syndromic diseases, schwannomas predominantly occur in NF2. If the diagnosis of NF2 is excluded, multiple tumours of this type in one individual make the diagnosis of schwannomatosis likely (81); however, the majority of schwannomas are sporadic cases. Schwannomatous parts within a neurogenic tumour are well recognized in histopathology (17). This finding is also known in NF1-associated neurofibromas (84). On the other hand, Riccardi is of the opinion that no schwannomatous parts can arise in peripheral nerve sheath tumours of NF1 patients (4).
Elephantiasis neuro(fibro)matosa. Unfortunately, there is no precise and uniform definition for the traditional term elephantiasis neuro(fibro)matosa (32-34, 36-38, 48, 55, 62). The definition and assignment of the term depends on the practitioner and their own estimation of the lesion’s size. A clear definition of which anatomical structures are affected (85, 86), in particular with regards to whether the bone is affected, is an important consideration in diagnostics and therapy, but is not included in the designation ‘elephant-like’ lesion. For good reasons, the term is rejected as outdated, even for some time. However, the alternative description of the phenotype as massive soft tissue neurofibroma (17) conveys little diagnostic clarity and does not indicate the morbidity of the lesion to the patient, which usually comprises much more than a neurogenic tumour, and does not indicate the biological potential of the tumour (39, 40, 43, 51, 63, 76).
Blood transfusion, resection planning. The portion of patients who had blood transfusions to compensate for blood loss is comparatively low. One reason for the rare indication for blood transfusion is the adaptation of the surgical procedure to the conditions of the surgical unit. The goal in all cases was to achieve primary wound care. For this reason, skin flaps were lifted which, with sufficient mobilization and careful haemostasis of the donor region, enabled coverage of the primary defect. Free grafts were never used for wound closure after debulking procedures for PNFs (73). Vascularized transplants were successfully used to cover defects in debulking procedures of NF1-associated PNFs (73). The risk of malignant tumour in a body region of the patient with NF1 also applies to the transplanted segment (87). The advantage of using local flaps for wound closure is that wound areas, which often bleed quite heavily, can be compressed and closed very quickly. The disadvantage of the procedure is the often smaller resection area adapted to the local conditions. However, the chosen treatment regimen reduces the mean treatment time. In addition, the length of hospital stay does not differ significantly from other interventions in the region in which regional flaps were used instead of tumour-invaded tissue for wound coverage. This assessment of the indication for transfusion in PNFs is consistent with a recently published study on this topic (77).
Malignancy (MPNST). The percentage of patients with MPNST was relatively low. In two patients, exploration of the tumour region (PNFs of the entire leg) in the thigh was suspected for a MPNST. The diagnosis was confirmed histologically. One patient survived this tumour after amputation and has been tumour-free for more than 10 years. The second patient was a boy of three at the time of diagnosis. The exploration of the limb was suspicious for a MPNST. The biopsy confirmed the finding. The child was treated exclusively with chemotherapy and died with evidence of tumour metastasis. An essential characteristic of the study group is the indication for the operative measure for aesthetic or functional reasons. The data do not contradict the relatively high risk of the patient with NF1 suffering from a MPNST (23-26). Rather, the data reflect the need of many patients to receive improvement in their physical conditions by correcting the often disfiguring and function-impairing lesions. In patients with NF1, the most important clinical parameters that alert the clinician to check the patient for a MPNST are unusually rapid tumour growth and local pain (4, 81). Of course, these findings are not limited to NF1-associated tumours, but because of their, often, multiple tumour burden, patients with NF1 may be less alert to changes in their body’s palpable findings and their general self-assessment.
Cross-sectional imaging techniques can assist in the diagnosis (44, 66, 68, 70). In individual cases, amputation can be avoided in patients with NF1 with a MPNST of the extremities (78).
Duration of surgery. The duration of the surgical measures indicates that these interventions can be easily integrated into the daily schedule of a surgical unit. However, for specially selected, locally very extensive tumours (79) or surgical concepts with interventions that affect larger anatomical units (64), far longer treatment times must be planned and are not covered in this time regime. Alternative surgical techniques require a separate categorization of the duration of the operation in relation to the size, extent, and type of PNF (64, 65). Embolization of nutrient vessels has been recommended as a means to reduce blood loss during surgery. We did not use this intervention as a presurgical treatment due to the unforeseeable impact of the measure on wound healing.
Complications. The complication rate is relatively low, in particular concerning the management of bleeding. However, deep suturing of the resection region prior to ablative measures is no guarantee of undisturbed wound healing or the safe prevention of bleeding during and after the operation. Wound healing in the PNF region is delayed. However, even adequately adapted, bilaterally, clearly visible tumour-infiltrated wound margins are capable of providing a functionally resilient epithelial closure of the wound.
Number of operations per patient. The number of operations per patient shows that a significant proportion of the patients had only one operation. However, the correlation of the number of dermatomes with the frequency of surgical measures shows that there is a correlation between the number of measures and the number of dermatomes. This classification therefore provides clues as to which patients need more frequent interventions. Despite this, recurrences of the PNF are difficult to predict (35).
Inpatient treatment time. An important question is whether or not the patient has to accept a longer hospital stay due to the complications that arise in the context of surgical measures. The difference between both long and short length of stay is not significant and complications arising during the course of treatment are not associated with prolonged hospitalization. In this evaluation we did not include the duration of the patient’s outpatient care by the family doctor. Additional outpatient care was rarely necessary, because the patients came from all over the republic. The vast majority of patients had to travel long distances between home and hospital. Therefore, discharge from inpatient treatment in terms of adequate wound care was a priority. There were only a few cases that preferred further local treatment of the increasingly shrinking wounds in outpatient care. The patients were always discharged with a local skin finding, which enabled the local wound care of a mobile patient. References to restrictions on the generalization of expected inpatient treatment time for PNFs of the buttocks, legs and feet derived from the presented data are necessary, because the sociopolitical requirements for inpatient treatment of patients can be very different in other countries. This information is particularly important for the treatment planning of patients with PNFs, because there is usually no malignant tumour that justifies a rapidly scheduled surgery and, thereafter, possibly a long-lasting inpatient intervention.
Male patients are affected by an average of 2.88 more dermatomes compared to female patients. The reason for this difference may be that men take longer time to look for treatment, because they are less disturbed by the lesions. It is unlikely to conclude from this result that larger tumours preferentially affect men. It is quite possible that the ‘affected dermatome’ factor is an additional factor concerning the age difference between men and women at the time of initial surgery. However, these studies, just like an earlier study on this topic (45), show that the assignment of tumours to a dermatome is very problematic. Apparently, the externally visible local growth behaviour of the PNF is no longer determined from the original (cutaneous) limitation of the terminal nerve branches. In fact, the tumours are largely evenly distributed over the dermatomes.
Our initial assumption about the distribution of surgically treated tumour regions preferentially arising in the buttocks is confirmed because the distribution of dermatomes in the buttocks and inguinal area was the most commonly treated region, accounting for 25.4%. Aesthetic reasons may have been decisive for the frequent demand for treatment. In order of frequency, the region of the foot is the second most common region of surgical interventions, accounting for 19.7%. It is very likely that aesthetic and functional reasons for the desired treatment are balanced in this region. The problem of finding only insufficiently suitable footwear was described very often in the medical reports. The size and distribution pattern of the tumours in relation to the dermatomes indicate the need for treatment.
All the patients in this study met the diagnostic criteria for NF1 (81). Patients with mosaic formation of NF1 were excluded from the evaluation based on clinical records. It is currently assumed that the proportion of patients with mosaic type NF1 is well below 10%. The mosaic NF1 phenotype is usually milder, and the need for treating PNFs may be less frequent than in patients with the complete NF1 phenotype. However, recent studies show that epidemiological assessments of the prevalence of the NF1 mosaic status probably need to be checked, because patients with NF1 mosaic status can escape discovery, despite very precise examination techniques (88). However, these considerations so far have no impact on surgical treatment planning concerning PNFs arising in the region of interest.
On the horizon of current pharmacological therapy concepts, the option to reduce tumour volume for hitherto untreatable patients with very extensive PNFs has appeared (89, 90). A permanent medication could cause previously untreatable tumours to reach a size that can be surgically treated or at least medication can contribute to reducing the extent of surgical treatment. These current developments may change the spectrum of surgical treatment fields in NF1 in the near future. Whether these potential expansions of therapeutic spectrum will also apply to the treatment of mosaic NF1 (91) and NF1-associated peripheral nerve sheath tumours with currently unknown biological potential is the subject of ongoing research (90).
In conclusion, the surgical treatment of patients with NF1 with extensive, disfiguring PNFs can alleviate tumour symptoms by debulking procedures to adjust the outer shape of the body region to its natural appearance in many cases. However, NF1 is a chronically progressive disease, so relapses have to be expected. The proportion of patients with NF1 with PNFs developing MPNST is relatively low in this study. However, the patient selection of this examination is biased by the predominant patient desire to improve shape and function in the body area. A surgical treatment concept for extensive nerve sheath tumours that is adapted to the individual situation can make a significant contribution to the symptomatic improvement of the patient suffering from disfiguring neoplasms.
Conference Presentation
The results of this study were presented in part in oral form (REF) on the occasion of the first “Chirurgisches Forum Neurofibromatosen Tübingen (CFNT)” connected with the 21st meeting of “Arbeitsgemeinschaft Neurofibromatosen,” Tübingen, Germany, 1-2 December 2017 and as an oral and poster presentation (REF) on the occasion of “Joint Global Neurofibromatosis Conference”, Paris, 2-6 November 2018.
Acknowledgements
The Authors would like to thank Prof. C. Hagel, MD, Institute of Neuropathology, UKE, for his expertise in diagnosing NF1-associated nerve sheath tumours.
Footnotes
Authors’ Contributions
REF treated the patients, designed the study, evaluated the documents and wrote the manuscript. CTT contributed to the analysis of data, designed parts of the graphic work, and was involved in the corrections of the manuscript. Both Authors have approved the final release of the manuscript for publication.
This article is freely accessible online.
Conflicts of Interest
The Authors declare no conflicts of interest regarding the publication of this manuscript.
- Received September 18, 2020.
- Revision received November 19, 2020.
- Accepted December 10, 2020.
- Copyright© 2021, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}