


Abstract
Monomeric C-reactive protein (mCRP), the dissociated form of native C-reactive protein, is a critical molecule that causes and perpetuates inflammation in serious diseases. It has ‘adhesive’-like properties causing aggregation of blood cells and platelets, and can stick permanently within arterial tissue where it can contribute to further complications including thrombosis, linking it potentially to atherosclerosis and subsequent acute coronary events. In this mini review, we discuss briefly the implications and the potential value of measuring and manipulating it for clinical diagnostics and therapeutic purposes.
C-reactive protein (CRP) is a an acute-phase pentraxin produced by the liver, usually during/following infection or tissue trauma in large quantities (up to 1,000-fold increase) compared to normal, systemic circulating levels, and released into the blood directly in response to macrophage, adipocyte or T-cell release of IL-6. It circulates as soluble native CRP (nCRP), which is relatively biologically inactive, and whose main functions are to mediate complement activation and bind to foreign or damaged cells thereby, promoting phagocytosis (1). It was first shown almost 30 years ago, that nCRP could dissociate into 5 identical sub-units of monomeric C-reactive protein (mCRP), which had strikingly different biological properties to the parent molecule (2). The astonishing properties of only the mCRP have been highlighted over the last decade by the explosion in publications year upon year to 2020.
CRP dissociates into mCRP directly upon contact with activated tissue, or cells (including circulating monocytes and platelets), particularly at sites of inflammation or infection (3). The mechanism through which cells, activated platelets or liposomes induce dissociation of CRP involves its binding to cell surface phosphocholine or lyso-phosphatidylcholine, followed by interaction with specific receptors at membrane lipid-rafts (e.g. FcγRI and II in phagocytic cells) through the mCRP-cholesterol-binding region (aa35-47) (4 and references there in). Next, mCRP stimulates enhanced local production of pro-inflammatory cytokines including IL-8, MCP-1, TNF-α IL-6, and associated transcription factors such as Nf-κB (3).
mCRP and Cardiovascular Disease
mCRP is a critical molecule that causes and perpetuates inflammation based on its ability to cause aggregation of blood cells linked to onset of acute coronary disease and atherosclerotic thrombotic plaques (5, 6). It can stick within the walls/intima of major arteries where it contributes significantly to worsening of atherosclerosis and the formation of unstable plaques increasing the likelihood of rupture and concomitant heart attack or stroke (7). Total native CRP levels in the blood correlate strongly with the above and clinical symptoms of unstable angina, myocardial infarction, stroke and peripheral artery disease (8). mCRP contributes significantly to thrombosis, while pentameric nCRP has no involvement in thrombogenesis. Specifically, blood mCRP induces platelet activation and thrombus growth (1). It has been shown that mCRP causes platelet aggregation and recruitment under high flow/sheer stress conditions (9, 10), and trapped mCRP inside growing platelet aggregates stimulated further platelet deposition (11). It has also been shown that mCRP induced increased fibrin polymerization in association with tissue factor expression; both strongly associated with the pro-coagulant activity of monocytes, clot production and thrombosis (12).
CRP and Atherosclerotic Plaque Development
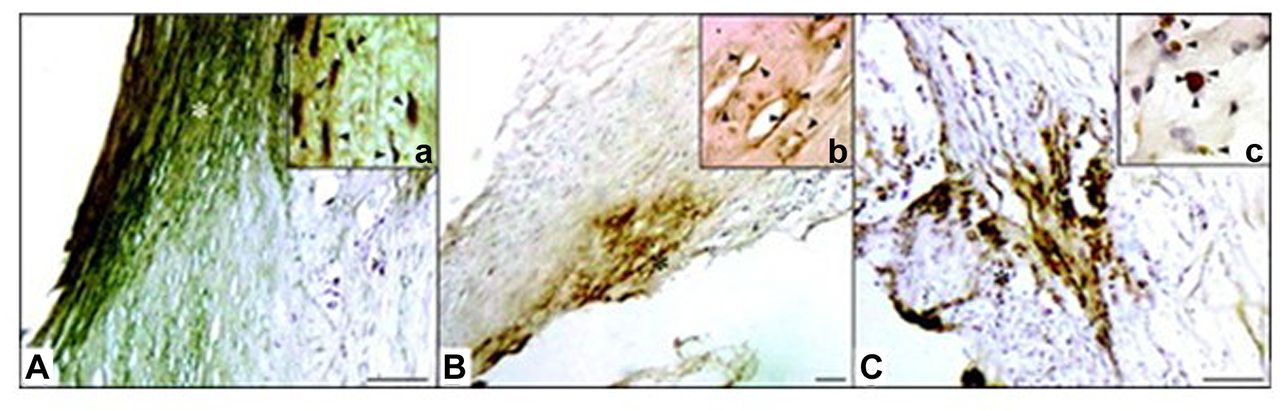
CRP contributes significantly to cardiovascular disease progression through cellular activation and ligand binding, primarily, to the fragment crystallizable region gamma receptors (FcγRs). mCRP is not present in the walls of healthy vessels arteries or in other tissues, but it becomes detectable in the early stages of atherogenesis and accumulates during the progression of atherosclerosis in association with increasing inflammation (13; Figure 1). In addition, mCRP accumulates within the infarcted myocardium after a heart attack and circulating mCRP levels are indicative of the severity of the disease and mortality (14).

Unstable atherosclerotic plaques showing strong neo-vessel rich staining for mCRP (high power inserts; coloured brown-HRP). Our previous work – (13).
Only mCRP is biologically active. It is present in the necrotic core of plaques, inhibits endothelial nitric oxide production and increases reactive oxygen species generation, contributing to atherosclerotic plaque instability by a variety of mechanisms. These include, increasing endothelial cell adhesiveness through the expression adhesion molecules, promotion of leukocyte and monocyte recruitment into the atheromatous plaque (promoting inflammation), enhancement of lipid accumulation, induction of cellular apoptosis and matrix break-down (e.g. through matrix metalloproteinase production), and by enzymatically binding to modified low-density lipoprotein (7, 15 and references therein). Recently, Ullah et al. (16), showed that blood mCRP produced in the local circulation binds with high affinity to fibronectin, significantly enhancing the adhesion of monocytes and promoting the inflammatory response.
mCRP and Vasculogenesis Contribution to the Disease
In addition, mCRP has significant pro-angiogenic and remodelling effects that can promote progression from a stable arterial thickening to an unstable tissue through rapid expansion as a result of the aberrant permeability of angiogenic blood vessels ‘that associates with structural changes, increased inflammation and instability of the atherosclerotic plaque (7, 9). mCRP has been shown to promote aberrant angiogenesis with leaky microvessels in the plaque core contributing to weakening and instability through haemorrhage and leukocyte and macrophage deposition (9). The capacity of mCRP to induce haemorrhagic vascularization in tissue and create permeable endothelial monolayer gap-junctions has been shown in vivo by our group (17) (Figure 2).

mCRP effects on vasculature permeability and patency. A) (top left to right) shows the effect of murine sub-cutaneous injection of PBS, nCRP, mCRP and VEGF in matrigel after 1 week, note the vascular aberrant haemorrhagic angiogenesis in the mCRP-containing sample. B) (left) normal TEM of gap junctions in aortic endothelial cells and (right)after treatment with mCRP, note degradation at the site creating increased permeability and potential inflammation. C) (top/middle images) enhanced permeability of mCRP-treated endothelial monolayer cultures and FITC-labelled dextran (lower)-increased expression of N-cadherin (western blotting) by the endothelial cells after mCRP treatment-a marker of adhesion and activation (16).
CRP-mCRP Detection and Modulation as a Novel Diagnostic, Prognostic and Therapeutic
The studies presented above suggest a possible novel therapeutic (protective, preventative) mechanism by blocking the conversion of nCRP (pentameric) to mCRP.
Our studies have shown that small off-target orphan molecules, particularly acetylcholine, due to its similarities with phosphocholine, demonstrated probable interaction with and binding to mCRP-phosphatidylcholine, blocked endothelial-monocyte activation and platelet aggregation, thereby nullifying inflammation (IL-6/TNF-α) in vitro (4). Regarding nCRP-dissociation inhibition, compounds containing phosphocholine dimers (five molecules between two pentamers) can potentially cross-link two CRP molecules together preventing dissociation into monomers, and has been shown to block CRP binding to LDL and inhibit C1q complement activation (18). Autoantibodies to mCRP (aa35-47) generated by patients with lupus nephritis inhibited the activity of complement factor H and predicted the most severe renal damage and worse outcome (19). Hence, providing a possible therapeutic and diagnostic target for auto-immune diseases. In addition, recently, Singh and Argrawal (20), described an mCRP mutant that was atheroprotective in a murine model of atherosclerosis providing an opportunity to create a novel therapeutic that when bound to LDL would reduce foam cell formation and local inflammation.
In terms of the measurement and detection of mCRP as a potential prognostic indicator of acute coronary events, mCRP may be a marker specific to the underlying pathological processes. Indeed, circulating or microparticle-bound mCRP (or bound to platelets/macrophages etc.) is a far better diagnostic index than nCRP in identifying and profiling myocardial infarction and peripheral artery disease as well as prognosis and follow up of stroke and inflammatory conditions including Lupus and giant cell arteritis. Development of an ELISA that discriminates nCRP from mCRP could provide a far more accurate method for the prediction of acute risk in acute myocardial infarction patients.
Crawford et al. (6) showed that the high-sensitivity CRP assay (hsCRP) did not measure pentameric CRP or mCRP on microparticles (MPs), whereas flow cytometry did. MPs derived from endothelial cells, particularly those bearing mCRP, were elevated in peripheral artery disease (PAD) patients compared to controls. The numbers of mCRP (+) endothelial MPs did not correlate with hsCRP measurements of soluble pCRP, indicating their independent modulation. In a model of vascular inflammation, mCRP induced endothelial shedding of MPs and was proinflammatory, while pCRP was anti-inflammatory. mCRP on endothelial MPs may be both an unmeasured indicator and an amplifier of vascular disease, and its detection might improve risk sensitivity. Melnikov et al. (21) also showed the significantly increased capacity of exosomes and microparticles derived from monocytes to transport mCRP in the blood from patients with coronary artery disease.
Currently, on the market, there is no successful assay to directly measure plasma bound mCRP. However, recently, Zhang et al. described using antibodies although not specific for mCRP, did not bind to the native form of mCRP at low concentrations (22). They successfully used this experimental kit to show that mCRP was a significantly better marker than nCRP in determining inflammatory status of several skin-related autoimmune disorders.
Conclusion
To summarise, there is now significant persuasive evidence implicating mCRP as a significant contributor to cardiovascular disease, creating a positive microenvironment for the perpetuation of inflammation within plaques, and promoting endothelial dysfunction, complement binding, monocyte polarization and platelet aggregation (23). Therefore, there should be a focussed effort to provide new diagnostic methods to measure its circulating levels in relation to diseases and to consider therapeutics that can abate its action within the tissues if not prevent the initial dissociation during acute inflammatory situations.
Footnotes
Authors’ Contributions
YZ-drafted the manuscript, SK and MS made the literature search and provided the figures.
This article is freely accessible online.
Conflicts of Interest
There are no conflicts of interest to declare regarding this study.
- Received November 18, 2020.
- Revision received December 15, 2020.
- Accepted December 17, 2020.
- Copyright© 2021, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.