


Abstract
Background/Aim: For recurrent/metastatic squamous cell carcinoma of the head and neck (R/M SCCHN), popular regimens containing platinum-based anticancer agents and immune checkpoint inhibitors are impractical for platinum-intolerant patients. Herein, the efficacy and safety of paclitaxel and cetuximab combination therapy in R/M SCCHN were evaluated. Patients and Methods: In this retrospective study, paclitaxel (80 mg/m2) and cetuximab (400 mg/m2 loading dose followed by 250 mg/m2 weekly) were administered in 28-day cycles on days 1, 8, and 15. Results: Thirty-eight patients were treated. The overall response and disease control rates of first-line therapy were 43% and 79%, respectively, while those of second-line and later therapies were 20% and 90%, respectively. The median progression-free and overall survival were 5.3 and 12.5 months, respectively. All adverse events were manageable, including grade 3/4 neutropenia and anaemia affecting 8-13% of patients. Conclusion: Paclitaxel and cetuximab combination therapy may be suitable for treating R/M SCCHN.
Recurrent/metastatic squamous cell carcinoma of the head and neck (R/M SCCHN) has a poor prognosis, and the overall survival is usually around one year (1). It is treated with systemic chemotherapy, and extreme regimens (5-fluorouracil+cisplatin/carboplatin+cetuximab) with platinum-based anticancer agents as the key drugs have long been considered as first choice for treatment (2). Additionally, immune checkpoint inhibitors (ICIs) have been widely used for head and neck cancer. However, the response rate of ICIs is not particularly high, and the time taken to manifest efficacy is a shortcoming. Therefore, cytotoxic anticancer agents are often used instead of ICIs in patients with pain, other subjective symptoms, and/or rapidly growing tumours.
In a phase II trial of weekly paclitaxel and cetuximab in platinum-refractory R/M SCCHN, high efficacy was reported (3). Moreover, several real-world retrospective studies on this combination as first-line therapy in patients who failed platinum-based therapy have reported an ORR, median PFS, and median OS of 45-52%, 6.0-7.7 months, and 10.0-16.8 months, respectively (4-7).
At our Institution, we typically administer combination therapy of paclitaxel and cetuximab for platinum-refractory or intolerant R/M SCCHN, and the objective of this study was to retrospectively examine its usefulness in this regard.
Patients and Methods
Patients. The target population included 51 patients who received paclitaxel and cetuximab combination therapy for R/M SCCHN at Tokyo Medical University Hospital from January 2014 to October 2019. Among 48 patients with squamous cell carcinoma, 10 were excluded because target lesions could not be evaluated by imaging, leaving 38 as subjects (Figure 1).
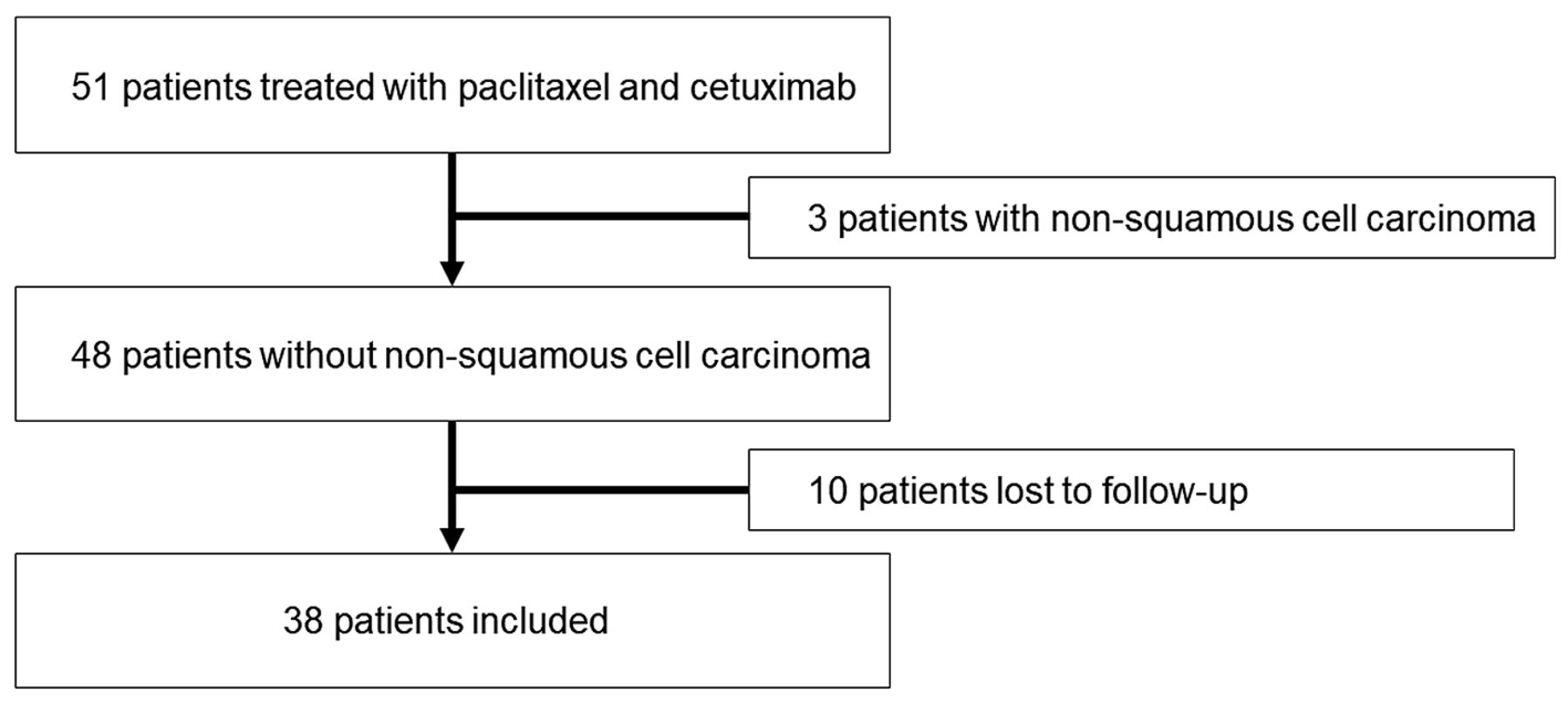
Flowchart outlining the selection of study subjects.
This study received approval from the ethics committee (approval no. T2020-0028) and was conducted according to the Declaration of Helsinki.
Staging methods. TNM classification was performed according to the criteria postulated by the Union for International Cancer Control (8).
Treatment and follow-up. Dosing was performed by following a 28-day cycle in which paclitaxel and cetuximab were administered on days 1, 8, and 15. Paclitaxel was infused at 80 mg/m2 over 1 h. Cetuximab was infused over 2 h at 400 mg/m2 for the first dose and 250 mg/m2 from the second dose onwards. Target lesions were evaluated every 2-3 months using computed tomography or magnetic resonance imaging. Treatment was continued until the disease progressed, intolerable adverse effects appeared, or the attending physician deemed discontinuation necessary for other reasons. No dose reduction criteria were established.
Endpoint. The primary endpoint was ORR [complete response (CR) + partial response (PR)]. The secondary endpoints were disease control rate (DCR) [CR+PR+ stable disease (SD)], PFS, OS, and adverse events (AEs). AEs were evaluated using the Common Terminology Criteria for Adverse Events version 4.0 (9). PFS was defined as the period from the start of administration to disease progression or death, while OS was the period from the start of administration to death or the date of final follow-up. For ORR, target lesions were evaluated using RECIST version 1.1, and ORR was determined as the best overall response (BOR) (10).
PFS and OS were compared between first-line therapies and second-line and later therapies. For patients receiving second-line and later therapies, PFS and OS were compared between those with and without prior nivolumab therapy. PFS and OS were also compared between platinum-sensitive and platinum-refractory patients. Platinum-refractory carcinoma was defined as recurrence or tumour enlargement within 6 months of starting platinum-based anticancer drugs, while platinum-sensitivity referred to recurrence or tumour enlargement after 6 months.
Statistical analysis. PFS and OS were calculated using the Kaplan–Meier method and analysed using the log-rank test. The survival period was analysed according to a Cox proportional hazards model, and p<0.05 was considered statistically significant.
All statistical analyses were performed with EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria) (11).
Results
Clinical characteristics. The patient clinical characteristics are shown in Table I. There were 33 men and 5 women with a median age of 65 years (range=28-78 years).
Patient clinical characteristics.
The median number of doses administered was 13 for paclitaxel (range=5-144), and 13 for cetuximab (range=5-144). There were 28 (74%), 6 (16%), and 4 (11%) patients receiving first-line, second-line, and third-line therapies, respectively. Nine patients had received nivolumab previously. Thirty patients had received platinum anticancer agents, 15 of whom were platinum-refractory and 15 were platinum-sensitive (Table II).
Summary of treatment.
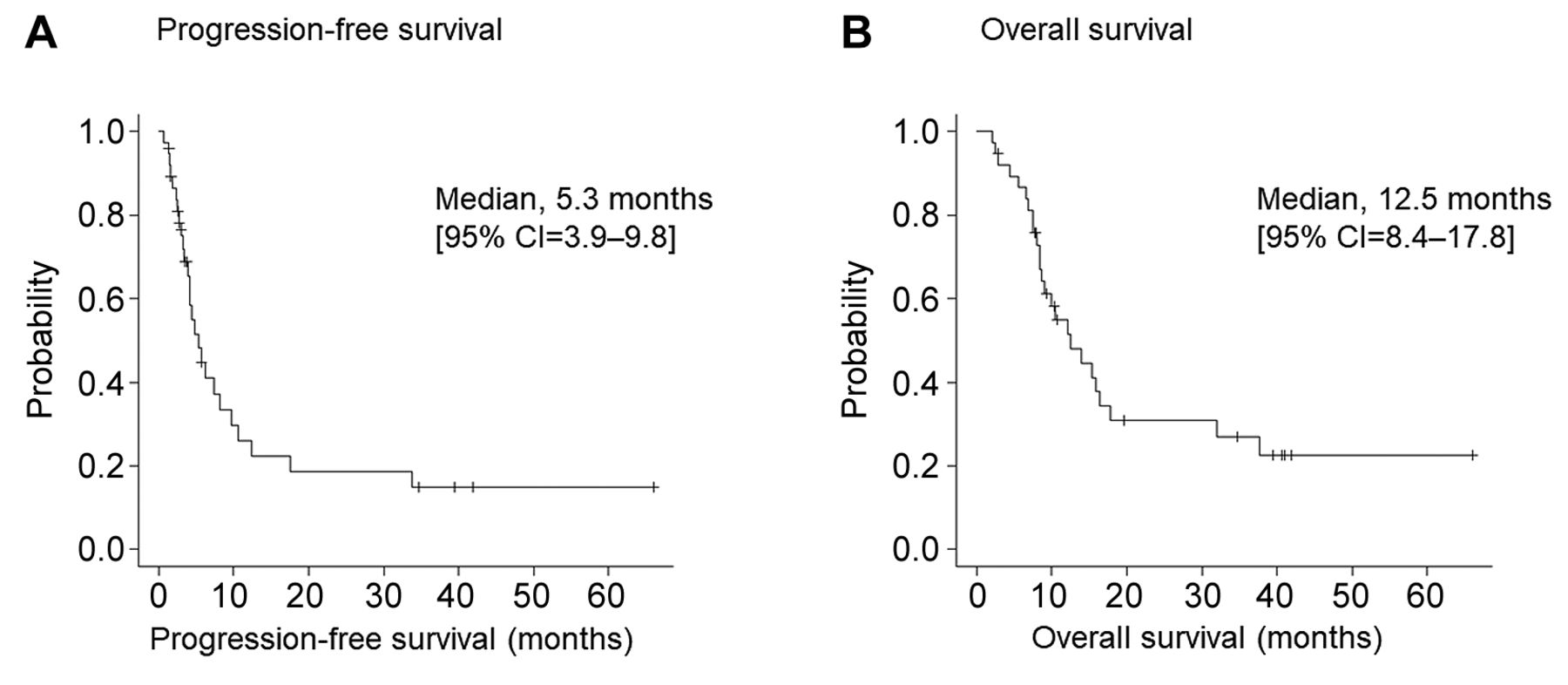
Efficacy. The best treatment outcomes are shown in Table III. The ORR and DCR were 37% and 82% (5 CR, 9 PR, and 17 SD), respectively. For first-line therapy, the ORR and DCR were 43% and 79% (4 CR, 8 PR, and 10 SD), respectively, while for second-line and later therapies, they were 20% and 90% (1 CR, 1 PR, and 7 SD), respectively. The median PFS and median OS were 5.3 months (95% CI=3.9-9.8) and 12.5 months (95% CI=8.4-17.8), respectively (Figure 2). With a median PFS of 6.2 months for first-line therapy, survival was significantly prolonged compared to 3.4 months for second-line and later therapies (HR=2.46; 95% CI=1.01-6.00; p=0.049). Median OS for first-line therapy was 15.3 months which was not significantly different from 12.1 months (HR=1.65; 95% CI=0.62-4.41; p=0.32) for second-line and later therapies (Figure 3).
Tumour responses.
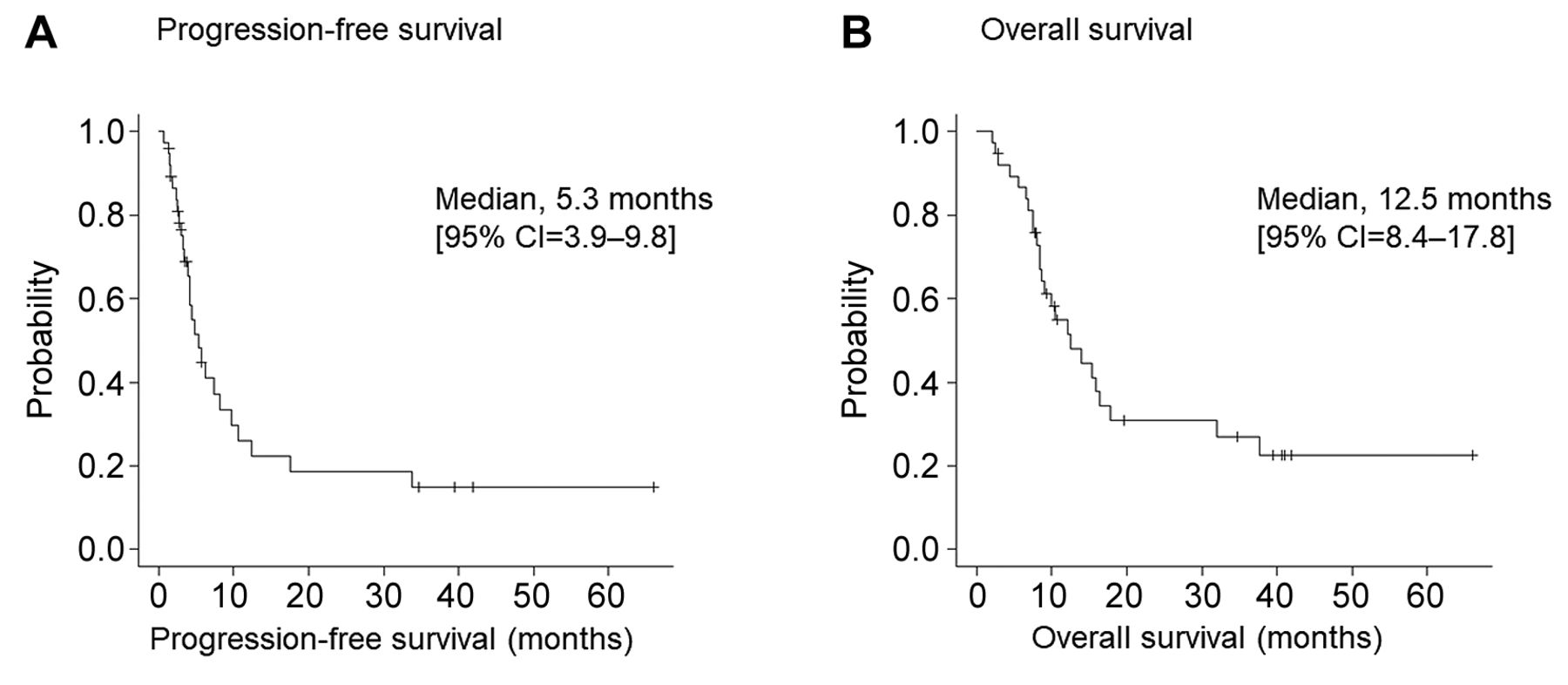
Kaplan–Meier plots (A) progression-free survival and (B) overall survival.

Kaplan–Meier survival curves of comparison of administration line.
Among the 10 patients who received second-line and later therapies, 9 received nivolumab prior and exhibited ORR, DCR, median PFS, and median OS of 22% (1 CR and 1 PR), 89% (CR, PR, and 6 SD), 4.1 months, and 12.1 months, respectively. Considering prior nivolumab use, the median PFS for patients who did not previously receive nivolumab was 6.2 months and those who did was 4.1 months; however, the difference was not significant (HR=2.13; 95% CI=0.85-5.33; p=0.11). Furthermore, the median OS for patients without and with prior nivolumab use was 12.5 months and 12.1 months, respectively; this difference was not significant either (HR=1.51; 95% CI=0.53-4.23; p=0.44). Similarly, the difference between the median PFS for platinum-refractory carcinoma (6.2 months) and that for platinum-sensitive carcinoma (4.4 months) was not significant (HR=1.33; 95% CI=0.55-3.21; p=0.53). At 12.5 months, the median OS for platinum-refractory carcinoma was not significantly different from that for platinum-sensitive carcinoma at 14.0 months (HR=0.91; 95% CI=0.36-2.26; p=0.84).
Safety. The AEs are shown in Table IV. Among the 3 patients with interstitial pneumonia, cetuximab was discontinued in 2 patients with grade 3 pneumonia and administration was continued with paclitaxel alone. There were no grade 5 AEs.
Summary of adverse events.
Discussion
In this study, the ORR and DCR of paclitaxel and cetuximab combination chemotherapy for R/M SCCHN were 37% and 82%, respectively. Median PFS and median OS were 5.3 months and 12.5 months, respectively. The PFS of first-line therapy was significantly prolonged compared to that of second-line and later therapies. There was no significant difference in survival rate between patients with and without prior nivolumab use or between platinum-sensitive and platinum-refractory patients. Moreover, AEs could mostly be controlled. Those of grade 3 and above with a high prevalence were leukocytopenia (18%) and anaemia (13%), but none were life-threatening.
Previous studies on paclitaxel and cetuximab combination chemotherapy in R/M SCCHN are shown in Table V (3-7, 12-15). For first-line therapy, ORR and DCR were 45-54% and 67-83%, respectively, and for second-line therapy, they were 38-71% and 74-100%, respectively, consistent with the results of 37% and 82%, respectively, in the present study. The first-line therapy significantly prolonged PFS over second-line and later therapies, indicating the advisability of initiating early administration.
Summary of literature reports on paclitaxel and cetuximab for squamous cell carcinoma of head and neck.
Re-administration of platinum-based agents is more effective for platinum-sensitive than platinum-refractory carcinoma, and the regimen varies depending on the period from the start of platinum administration to recurrence (16, 17). Based on the CheckMate 141 and Keynote 048 trials, the recommended drugs for platinum-refractory and platinum-sensitive R/M SCCHN are nivolumab and extreme regimens involving pembrolizumab plus (5-fluorouracil and cisplatin/carboplatin), respectively (18, 19). However, in patients with pain and other subjective symptoms or with rapidly expanding tumours, we cannot expect ICIs to be effective because the response rate is not very high and their effects manifest only after some time. As paclitaxel and cetuximab combination chemotherapy showed good efficacy in patients irrespective of whether they were platinum-refractory or -sensitive, we considered it effective in these patients regardless of the duration of platinum administration.
Conversely, chemotherapy after nivolumab improves OS relative to best supportive care, demonstrating its usefulness after ICI administration (20). In patients who received sequential chemotherapy after ICI, 53% received taxane plus cetuximab plus platinum which resulted in an ORR of 30% and DCR 57% (21). In the 9 patients with prior nivolumab use in this study, DCR being 89% and median OS 12.1 months were favourable, indicating the usefulness of paclitaxel and cetuximab as sequential chemotherapy. Thus, the response rate for paclitaxel and cetuximab combination chemotherapy for both first-line and second-line therapies was high. According to the National Comprehensive Cancer Network (NCCN) guidelines, platinum, nivolumab, and pembrolizumab have a higher priority in the treatment of R/M SCCHN (22). Additionally, although they provide details for paclitaxel alone and cetuximab alone, there are none for combination therapy. Nevertheless, the combination therapy achieved good results for second-line and later therapies, which were comparable to those for first-line therapy. As it could be used as sequential chemotherapy after ICI and would not be influenced by whether patients were platinum-refractory or -sensitive, we believe that the paclitaxel and cetuximab combination chemotherapy would be useful in any treatment situation.
Peripheral neuropathy, a characteristic adverse event of paclitaxel and acne-like rash, a characteristic adverse event of cetuximab, could be factors that reduce the quality of life. At 3%, the prevalence of grade 3 or above peripheral neuropathy and acne-like rash was low and controllable. Because paclitaxel and cetuximab combination chemotherapy is palliative, AEs should be minimized. The package insert of paclitaxel distributed in Japan recommends six weeks of administration followed by a 2-week rest period (23). Considering this, in the present study, paclitaxel was administered not on a weekly basis, but with three doses and one rest period to reduce AEs. The prevalence of AEs was lower than that reported in the literature and helped improve the quality of life. The complete absence of discontinuation, a maintained response rate, and a low prevalence of adverse events can be comprehensively evaluated.
Photoimmunotherapy is one of the latest therapies for treating R/M SCCHN. A phase I/IIa study of photoimmunotherapy on R/M SCCHN (RM-1929-101) was conducted in 2015. Based on these results, it was fast-tracked in the US in January 2018. This therapy is based on cetuximab sarotalocan sodium, an antibody-photosensitive substance complex consisting of cetuximab [anti-human epidermal growth factor receptor (EGFR) monoclonal antibody] bound to IR700 dye, a photosensitive substance. The antibody-photosensitive substance complex is believed to selectively bind to EGFRs expressed by cancer cells. When the tumour is irradiated with near-infrared rays through excitation, IR700 causes a photochemical reaction, which rapidly destroys cancer cell membranes, leading to necrosis (24). In patients responsive to cetuximab and paclitaxel combination chemotherapy, photoimmunotherapy could be effective because anti-EFGR antibodies would be bound to cancer cells. In the future, we hope that evidence will be accumulated using a large sample size.
The advantage of paclitaxel and cetuximab combination chemotherapy was that it had a high response rate in both first and second line. Therefore, in R/M SCCHN, a therapeutic effect can be expected regardless of platinum refractory or platinum sensitivity. In addition, adverse events were controllable and could contribute to the maintenance of quality of life.
This study has several limitations. First, as it was a retrospective study using treatment records, selection bias was unavoidable. The choice of chemotherapy regimen was influenced by the overall body condition and prior therapy. Second, not all patients administered ICI at our Institution were analysed. Third, in Japan, not all the drugs recommended in the NCCN guidelines can be used, making a simple comparison with studies from other countries difficult. However, in view of the high DCR and low incidence of AEs, paclitaxel and cetuximab combination chemotherapy is considered a treatment option following ICI therapy for patients who are platinum-refractory or platinum-intolerant, those with subjective symptoms, and those with rapidly growing tumours.
Conclusion
In this retrospective study, the usefulness of paclitaxel and cetuximab combination chemotherapy in both platinum-sensitive and platinum-refractory R/M SCCHN was demonstrated. It showed particular promise as a sequential chemotherapy following ICI therapy.
Acknowledgements
The Authors would like to thank Editage (www.editage.com) for English language editing.
Footnotes
Authors’ Contributions
TO designed this study. TO and IO contributed to collection and interpretation of the data. TO, IO, HS, TI, KM, and KT contributed to data collection and patient management. TO was a major contributor in writing the manuscript.
This article is freely accessible online.
Conflicts of Interest
The Authors declare no conflicts of interest.
- Received January 6, 2021.
- Revision received January 27, 2021.
- Accepted January 28, 2021.
- Copyright© 2021, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Effects of Pembrolizumab in Recurrent/Metastatic Squamous Cell Head and Neck Carcinoma: A Multicenter Retrospective Study
- Induction Chemotherapy With 5-Fluorouracil, Cisplatin, and Cetuximab in Advanced Head and Neck Squamous Cell Carcinoma
- Immune Checkpoint Inhibitors for Nasopharyngeal Carcinoma in a Real-world Setting in Japan
- Cisplatin Versus Carboplatin and Paclitaxel in Radiochemotherapy for Patients With Locally Advanced Head and Neck Squamous Cell Carcinoma