


Abstract
Background/Aim: Transanal endoscopic microsurgery (TEMS) is a form of minimally invasive surgery for selected rectal cancers. The aim of this study was to explore the factors affecting patients’ decision-making concerning the choice of surgical treatment as well as to measure the Quality of Life (QoL) post-TEMS. Patients and Methods: Thirty-four patients with rectal cancer stage T1/T2-N0-M0 that underwent TEMS were studied. The questionnaires used included the Short Form SF12v2, Wexner Score (CCF-FIS) and the Sexual Function Questionnaire (SFQ). The patients’ views on experience and treatment decision were obtained with a custom-designed questionnaire. Questionnaires were completed at a mean of 6.9 years following treatment. Results: The factors that influenced the patients’ decisions were: experience satisfaction (p=0.003), postoperative bowel function (p<0.001), lower incontinence score (p=0.020) and agreement of TEMS experience with preoperative information (p=0.049). Treatment experience satisfaction was associated with family support (p=0.034) and agreement with preoperative information (p=0.047), better bowel function (p=0.026) and mental QoL (MCS) (p=0.003). Conclusion: factors important to patients when reflecting on treatment experience are adequate and reliable information, a good QoL and the presence of family support. Clinicians should incorporate those parameters in their practice when assisting patients in making a surgical treatment choice and provide informed consent on TEMS for rectal cancer.
Colorectal cancer (CRC) is the third most common cancer in men and second in women, globally (1), with the highest incidence of 44% in people over 75 years of age (2), and survival rates around 60% for 10 years or more for rectal cancer alone (3).
Rectal cancer (RC) is an important subgroup of colorectal cancer (CRC): it may result from different gene alterations (4) and its treatment is surgically more challenging. The “gold standard” of RC treatment is total mesorectal excision (TME) by either low anterior resection (LAR) or by abdominoperineal resection (APR) of the rectum with temporary ileostomy or a permanent stoma, respectively (5). Both operations are associated with significant morbidity (6). Sexual and bladder dysfunction, and the impairment of anal sphincter function impact patients’ QoL following treatment (7, 8). Physical, social and emotional functions among patients are worse compared to the general population (7) while in older adults this may cause the loss of their social autonomy (9, 10).
An alternative to TME is the minimally invasive transanal endoscopic microsurgery (TEMS), which was introduced by Buess (11) in the early 1980s for selected early rectal cancers (ERC). The advantages of TEMS, apart from preserving the sphincters and the rectal function, are fast recovery and a shorter hospitalization (average 2 days) with much lower morbidity and mortality than LAR and APR (12, 13). TEMS has gained gradual acceptance and inclusion in international guidelines for the local excision of low-risk early-stage cancer (5, 14). The TEMS technique for ERC was shown to be safe with low local recurrence, high survival rates (13, 15) and equal oncological results with radical surgery (16-18). Although there are reports suggesting that the local recurrence rate after TEMS is higher compared to radical surgery (17, 18), in 90% of those cases “salvage surgery” with LAR/APR can be curative and the final mortality is no different compared to initially performed radical surgery (19, 20).
Hence, the decision regarding treatments that are similar in clinical and oncological outcomes rely on patient experience and QoL following treatment. Furthermore, in older and frail patients the surgical trauma should be kept to a minimum (9) with organ preservation, aiming for functional advantages and better QoL. Only few studies have addressed the QoL after TEMS with small samples and follow-up up to one year in most cases. The findings show that QoL returns to pro-TEMS levels in one year postoperatively and faecal continence seems to be affected temporarily (21, 22). Some aspects of QoL are better in TEMS patients than in TME (23), but the overall QoL compared to general population is found to be similar (21, 23). Nonetheless, it is not clear what QoL patients have after TEMS (24), and to which extend it justifies their treatment decision.
Patient involvement in treatment decisions is fundamental in modern health care and known to be beneficial to patient experience (25, 26). To the best of our knowledge, there is no literature regarding factors influencing patient decision-making towards the TEMS option against radical surgery. The aims of this study were to explore factors affecting patients’ decision-making in choice of surgical treatment and to measure the QoL post-TEMS.
Patients and Methods
This study was conducted in a tertiary Coloproctology Unit at King’s College Hospital, London, which is a center of excellence in TEMS. Patients were prospectively registered and followed up in a secure database. Prior to circulation of any study material, we identified deceased patients via our database, as well the electronic patients records (EPR). A unique identifier was given to each eligible individual, and all relevant clinical details were assigned to it in order to ensure data confidentiality. A separate anonymized list of eligible patients was created that included demographics and clinical data.
Sample. Participants were patients with confirmed diagnosis of stage T1-T2 -N0-M0 rectal cancer who underwent TEMS from 2002 to 2012. The inclusion criteria were patients who were operated with curative intent and also had a minimum of 3 years follow-up. We excluded patients who had recurrence after local excision (those were submitted to “salvage surgery”) or high-risk pathology of the excised tumour specimen (those were submitted to “completion surgery”). All operations on patients enrolled in the study were performed by the same specialist surgeon (author SP).
Ethics. This study was granted permission by the NHS Lothian Research Ethics Committee (Protocol number REC reference: 15/SS/0077); it has also been approved by the local Ethics Committee of King’s College Hospital NHS Foundation Trust: Registration KCH15-180.
Instruments. We used three validated questionnaires for assessing QoL, bowel continence and sexual functioning: SF-12 – version 2.0 (27), Cleveland Clinic Florida Faecal Incontinence Score CCF-FIS (Wexner Score) (28) and Sexual Functioning Questionnaire (29). In addition, for the purpose of the study a questionnaire was specifically designed regarding patients’ TEMS experience and reflection upon the choice and decision of treatment. These questionnaires are described in Table I.
Research instruments: SF12v2, Wexner score, SFQ and TEMS evaluation questionnaire.
Data collection. Data was collected over 3 months. Initially we prepared a research pack of 4 questionnaires, where each pack was assigned a unique ID. The questionnaire pack with an explanatory cover letter and a pre-paid envelop was posted to eligible candidates. To achieve an increase in the response rates, 4 weeks later a reminder was sent out. Consent was implied by the participants returning the questionnaire.
Statistical analysis. We applied simple descriptive statistics to describe our results, which followed each questionnaire’s manual scoring; missing data were handled according to the provided guidelines. Normality was tested using the Kolmogorov-Smirnov test. Normally distributed numerical variables were expressed as mean (standard deviation) while variables with skewed distribution were expressed as median (interquartile range). Qualitative variables were expressed in absolute and relative frequencies. For the comparison of continuous variables between two groups, a Student’s t-test or Mann-Whitney U-test was used, as appropriate. Pearson’s or Spearman’s correlation coefficients were used to explore the association of two continuous variables. Correlation coefficients between 0.1 and 0.3 were considered low, between 0.31 and 0.5 moderate and those over 0.5 were considered high. Data were modelled using multiple linear regression analyses; the SFQ subscales and the overall score were the dependent variables. The regression equation included terms for gender, age, time of follow-up, Wexner score, PCS and MCS, as well as terms concerning the patients’ present symptoms. Regression coefficients (β) with standard errors (SE) were computed from the results of the linear regression analyses using logarithmic transformation due to the lack of normal distribution of the dependent variables, using the stepwise method (p for entry 0.05, p for removal 0.10). All reported p-values are two-tailed. Statistical significance was set at p<0.05 and analyses were conducted using SPSS (version 19.0, IBM, NY, USA).
Results
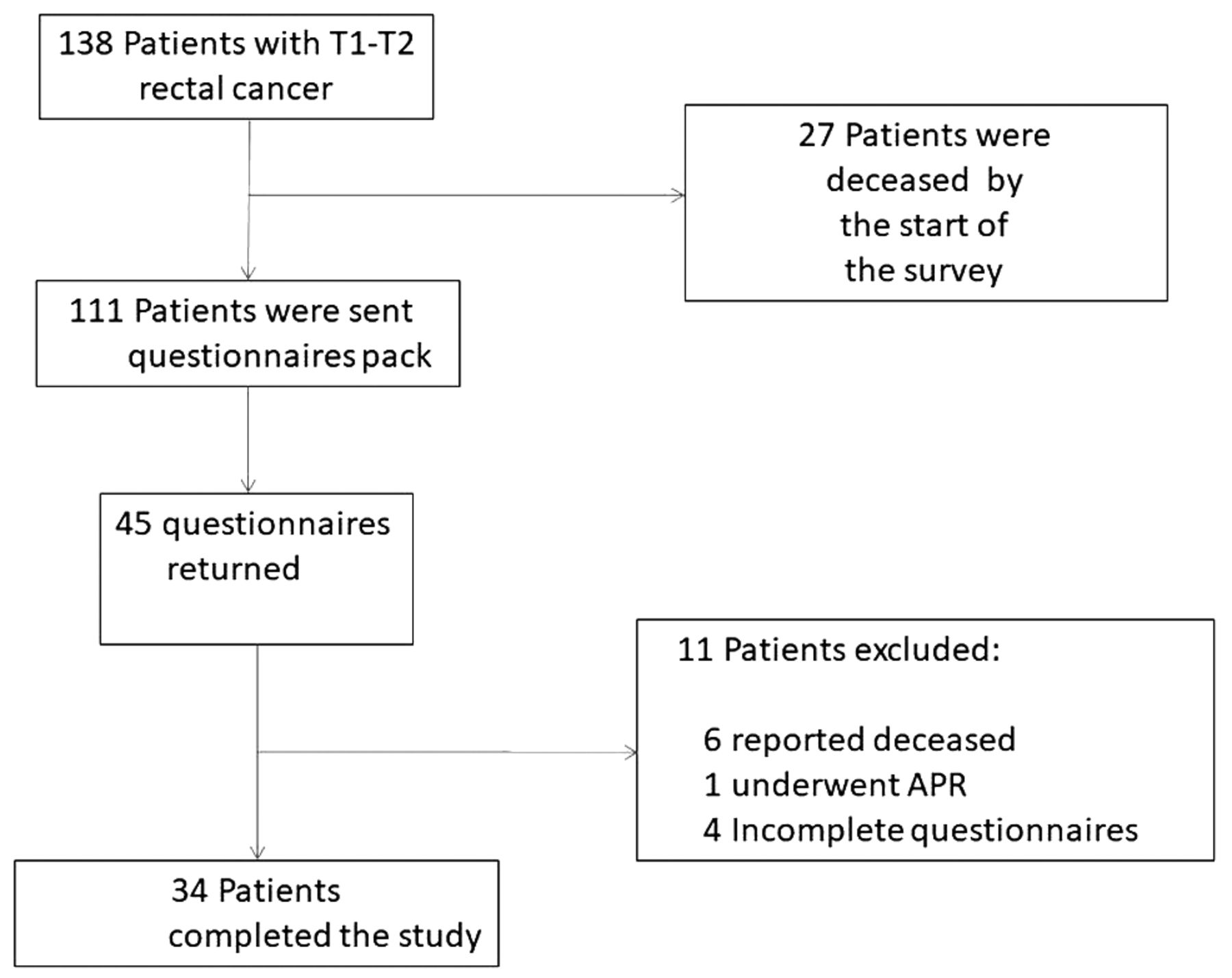
Out of 138 cases identified from a primary search on EPR from 2002 to 2012, 34 patients completed the questionnaires, a response rate of 31% (34/111). The process of data collection is presented in Figure 1.

Process of data collection.
The mean follow-up time was 6.9 years (SD=2.0), ranging from 4 to 12 years. The mean age of the study population was 75.6 years (SD=8.2) and the mean age at surgery was 68.2 years (SD=8.5). The male: female ratio was 22/12. Sample basic characteristics and instrument scores are summarized in Table II. Non-respondents’ (n=66) characteristics did not differ from respondents: mean age was 76.7 years (SD=12.5), while mean age at surgery was 69.2 years (SD=12.2) and the follow up mean was 7.0 years (SD=2.0).
Patients’ characteristics, SF12v2, Wexner and SFQ scores.
Quality of life. The mean physical QoL of the studied population was lower compared to the UK general population: 44.4 (SD=12.0) vs. 50.0 (SD=9.7), p=0.001. The male physical QoL was lower than in the general population: 41.1 (SD=12.3) vs. 51.2 (SD=9.2), p<0.001.
The mental QoL of the study population was comparable to the general UK population: 49.3 (SD=10.9) vs. 50.0 (SD=9.7), p=0.667. No differences were found in comparisons adjusted for sex: male 48.9 (SD=11.0) vs. 51.4 (SD=8.9), p=0.186; female 50.0 (SD=11.5) vs. 49.0 (SD=10.2), p=0.729 (Table III).
Comparison of Quality of Life scores with the general UK population.
Similar results were found when compared to the US general population: physical QoL 44.4 (SD=12) vs. 49.37 (SD=9.75), p=0.002; mental QoL 49.3 (SD=10.9) vs. 49.37 (SD=9.75), p=0.891. No significant differences were found in PCS and MCS when compared with age-appropriate population norms (p>0.05) (27).
Continence. Twenty-eight (82.4%) patients reported good or perfect continence (61.8% and 20.6%, respectively). Mean Wexner Score (WxSc) for our population was 3.97 (SD=3.86) out of 20 (Table II) and did not differ between sexes. The percentage of patients who had at least one episode of solid stool or liquid accident in the last month was 17.64% (n=6) and 23.5% (n=8) respectively; overall 32.35% (n=11) had liquid or stool episodes at least once per month. Greater WxSc was associated with worse outcomes in physical and mental QoL: r=–0.40; p=0.019 and r=–0.38; p=0.025, respectively.
The patients’ own perception regarding having incontinence and the clinical objective measurement (WxSc) differed. Incontinence for stools, as a current symptom, was reported by 7 patients (24.1%) with a mean Wexner Score of 9.7. Patients with a WxSc score up to 5 felt free of incontinence and those who reported WxSc between 6-17 had incontinence. One person with WxSc of 8 viewed his present condition as free from incontinence.
Sexual functionality. The Overall SFQ score and subscale scores did not differ between males and females (Table IV). Only 24% (n=7) stated that they were sexually active in the past month. The most common reason for sexual inactivity was lack of a partner (33%; n=7), followed by “having a physical problem” (23.8%, n=5).
Sexual functioning questionnaire scores: comparison between genders.
Sexual functioning, QoL, continence and age. The relationship between SFQ, QoL, Wexner Score and age is summarized in Table V. Multiple linear regression analysis was applied for possible risk factors that affect sexual functionality. Poorer function regarding desire and masturbation was significantly associated with increasing age. Better physical QoL was associated with better sexual functioning and arousal. Fewer sexual problems and higher satisfaction were significantly associated with better mental QoL. Additionally, a higher Wexner score, indicating more incontinence symptoms, was associated with a greater medical impact (worse sexual functioning). Factors influencing patients’ decision-making. The patients’ TEMS experience, current symptoms, a service-referral evaluation and decision on treatment responses are presented in Table VI.
Sexual functioning, QoL, continence and age: results of multiple linear regression analysis having SFQ subscales as dependent variables.
TEMS treatment evaluation.
Twenty-five patients (86.2%) would have persisted with their TEMS treatment decision and the majority (57%) would travel to have this treatment. The majority of the patients (71.4%) did not receive any additional treatment after TEMS. From the remaining 28%, 2 patients had adjuvant radiotherapy and 6 underwent further endoscopic resection.
There was satisfaction with the provided information regarding treatment options by 84.6% of patients (explained very well by 61.5% and well by 23.1%); two out of three patients stated that post-TEMS experience was in agreement with preoperative information.
Treatment information was understood by the majority of patients (59.3%, n=16) who discussed it thoroughly with their family. Satisfactory counseling with the clinical nurse specialist (CNS) was reported by 13 patients (68.4%); still one third of patients (31.6%) needed more time for discussion with the CNS. Postoperative pain was rated as 1 (median; IQR=0-5.5) on a scale of 0-10 (no pain at all to very painful), and postoperative bowel disruption was rated acceptable or relieving in 66.7% of patients (63% and 3.7%, respectively).
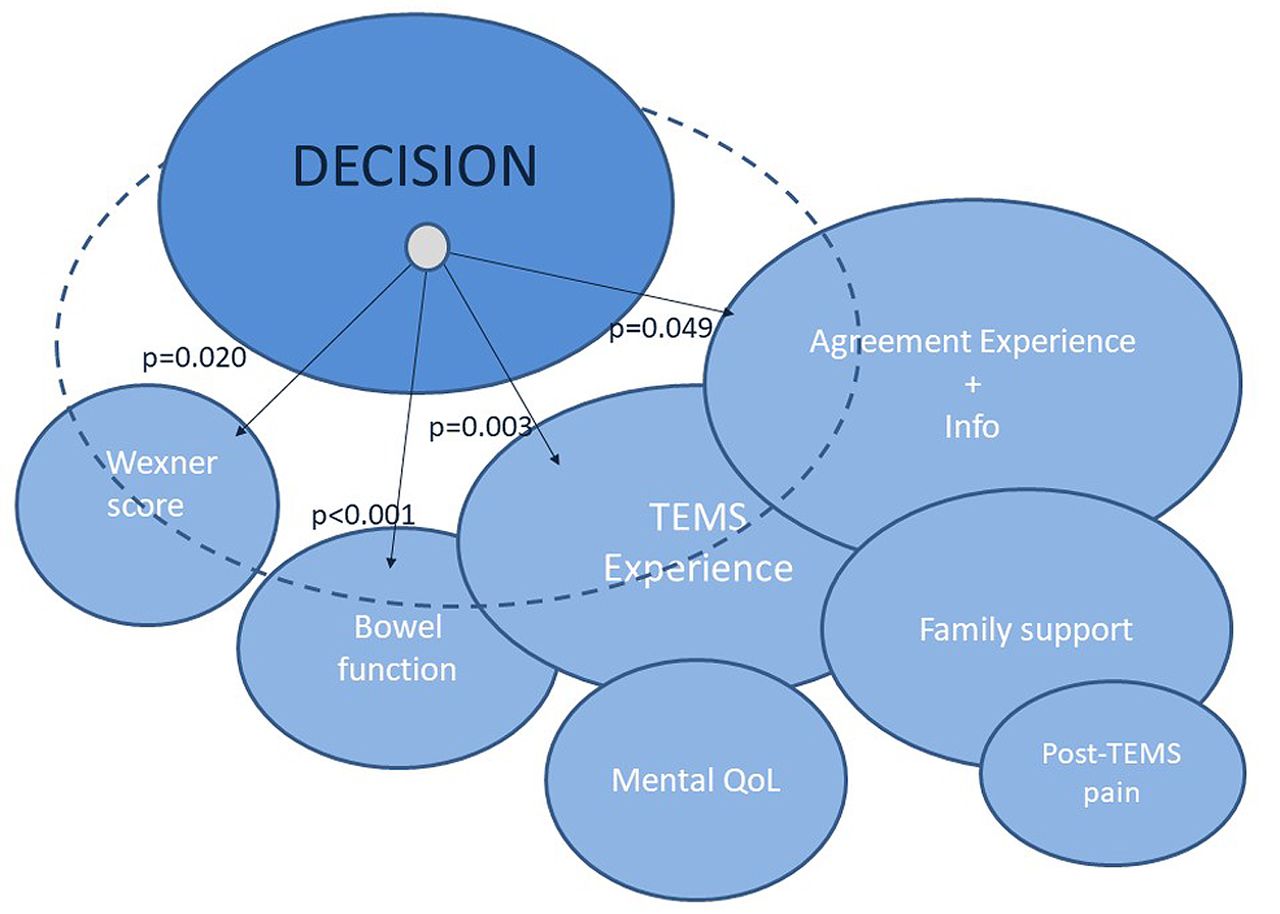
Patients were asked if they would have the same TEMS surgery in a similar situation. This decision statement was influenced by the patients’ experience (p=0.003), post-TEMS bowel function of an acceptable and relieving level (p<0.001), a lower Wexner score (p=0.020) and patient experience in agreement with information prior to surgery (p=0.049) (Figure 2).

Factors reflecting on decision satisfaction and their interrelations with treatment experience and QoL. Decision: “Would you have the TEMS surgery again in a similar situation?” Agreement Experience and Info: “Was your experience after TEMS in accordance with what was told to you beforehand?” Family support: “Did you feel you had the chance and enough time to digest the information and discuss with your family?” TEMS Experience: “Would you rate your experience from TEMS surgery as positive or negative on a scale of 0-10?”
The patients’ TEMS experience was rated on a scale of 0-10 (negative-positive) with a mean of 7.9 (SD=2.8). Treatment satisfaction was associated with family support (p=0.034) and post-TEMS bowel function when acceptable and relieving (p=0.026). Patients who had higher mental QoL score were satisfied more as well (p=0.003). The association of TEMS experience with the quality of written information tended to but did not reach a statistical significance (p=0.073), similarly to the information on treatment options (p=0.088).
Family support influenced the patients’ understanding of information, the agreement of treatment experience with preoperative information (p=0.004) and overall satisfaction (p=0.047). However, association with information on what to expect after TEMS did not reach statistical significance (p=0.059). Lower post-operative pain was reported by patients who had more family support (p=0.009) (Figure 2).
Discussion
This study showed that provision of adequate information, reliability of information and family support are factors that significantly affect the patients’ decision-making in choosing TEMS as opposed to radical surgery for rectal cancer. Also, it demonstrated that the long-term QoL post-TEMS leads patients to feel justified regarding their decision on operating choice.
The long term QoL in our patients was found to be no different than in the general population, when corrected for similar age groups. Comparable QoL scores between patients post-TEMS and the general population have been reported earlier (21, 23), though with a shorter follow up time; the present study reports the longest reported follow up with a mean follow up of 6.9 years. Lower scores in males and in the whole study population in respect to the physical QoL could be attributed to the development of various comorbidities, unrelated to CRC. Moreover, a significantly impaired QoL has been seen in older (over 75 years) compared to younger patients, 4 years post-TEMS (30).
Continence in the majority of our patients after 4-12 years post-TEMS showed a good Wexner score with a mean equal to 3.97. Previous research has shown TEMS to affect short term faecal continence due to rectal dilatation during the operation; this is however temporary (31), as the bowel function returns to the pre-operative levels after 6 months to 1-year post-operation (21, 32). It does not however improve in all cases (22, 33).
Prevalence of faecal incontinence (FI) in the general population ranges between 8.3% and 12.4%, and in the population over 70 years old this condition increases to 14.15%-18.39%, showing a strong association with increasing age (based on liquid or solid episodes, at least once per month) (34, 35). The self-reported incontinence in the present study was higher compared to the general population, but lower compared to rectal cancer groups after sphincter preserving surgery; in these groups, the reported prevalence was 32% for liquid and 15% for solid stool 4 years post-surgery (36), based on incontinence episodes of at least once per week.
We applied the sexual functioning questionnaire (SFQ) because it has a multidimensional construct and assesses sexual functionality within four phases of the sexual response cycle, problems and relationship. Men and women in our sample reported similar sexual functioning in all subscales, with the overall SFQ score being lower than the score obtained by other cancer groups: the SFQ score mean was equal to 2.559 (SD=0.773) in prostate cancer male patients (37), 3.2 (SD=1.0)/2.1 (SD=1.1) in cancer male/female survivals 5 years after haematopoietic cell transplantation (38) and 2.41 (SD=0.93) in breast cancer female patients (39). However, these were younger populations, the mean age was 61.19 (SD=8.16), 47.0 (SD=8.9) and 37.8 (27-66 range), respectively.
Age and health problems are negatively associated with many aspects of sexuality, while the experience of sexual dysfunction is generally associated with a poor QoL (40). In support of this, we found increased sexual functioning to be associated with higher physical QoL; and increased mental QoL reflected in higher satisfaction and fewer sexual problems, which is in agreement with Laumann and Waite’s study (41), with the exception of their results showing satisfaction in the relationship to be associated with fewer sexual problems. In our study, a poorer sexual desire was associated with ageing. Research evidence shows low scores of sexual desire from 5% in ages 45-49 to 59% in ages 80-84 (42).
The continence level (WxSc) as a current condition was reflected in a higher medical impact score (worse sexual functioning) and affected physical and mental QoL as well, all reflecting the age of our sample. As reported previously, incontinence is associated with psychosocial function (43) and impaired QoL after TEMS as well as symptoms like diarrhoea and constipation, which are found to be worse in patients older than 75 years (30).
This study identified that patient experience and its agreement with information prior to surgery as well as bowel function were factors that affect the patients’ decision towards TEMS. The positive experience following TEMS surgery in this study confirms that the minimally invasive nature of endoscopic local excision surgery results in increased patient satisfaction. Undoubtedly, the absence of postoperative pain and immobility and the very low rate of complications play a role in patient experience. The satisfactory post-TEMS bowel function justified the patients’ choice and confirmed the presumed advantage of TEMS as opposed to radical surgery. Likewise, Planting et al. (22) found 24 of 30 patients were satisfied with TEMS and would prefer the same treatment choice.
There is substantial research evidence that communication and family support are of great importance to clinical outcomes, decisional conflict and treatment choice (25, 26, 44, 45). This study demonstrates that communication in terms of provided information and its understanding had a positive influence on patient experience. More than two thirds of the patients admitted that the treatment they received was exactly as they were told during counselling, which reinforces confidence and a healthy relationship between the healthcare providers and the patient. Moreover, patients who had thorough discussion with their family scored better in treatment experience, postoperative pain and expected outcomes - all factors that affected their treatment choice. Furthermore, the positive association between mental QoL and treatment experience, which in turn was associated with pre-operative information, has been seen in other cancer patients as well. Vogel et al. (46) found that patients that were better informed and satisfied for being involved in the decision-making process had better QoL, even months after surgery.
Still, one third of our patients remember having been “told little” about “what to expect after TEMS”. The patients’ retention of information which relates to the postoperative period is poor (47) and might be attributed to the absence of a family member during the information exchange (44). This gap may be filled by an important member of a multidisciplinary team. The role of a colorectal nurse specialist (CNS) is indispensable; research evidence shows that 80% of patients found talking to a CNS to be helpful (48). We believe that consultation with a CNS is of great importance in information embracing, and the majority of our patients valued it highly; interestingly, one third would prefer to have more time for discussion with a CNS. This important finding, points to more attention and time needed when patients are facing a complex treatment decision.
One limitation of our study is the low response rate at this age group, which resulted in small sample as has been seen elsewhere (32, 33). Moreover, participation gradually decreases as time passes on (21, 30). Another limitation is that there was no pre-assessment on patients’ incontinence and sexual functioning. However, with regard to incontinence, the majority of our patients had a good Wexner score and high satisfaction, which resulted in a good overall TEMS experience. Moreover, it has been established that the presence of rectal tumours and also rectal radiotherapy has an effect on faecal continence, and this is why neither we nor other researchers do a routine pre-operative scoring of continence unless there is relevant clinical history. There was an age difference in the sexual functioning assessment norms; however, an age-appropriate comparison was made with the general population.
Conclusion
This study showed that the factors which are significant to patients in choosing local excision as opposed to radical surgery for rectal cancer are a) availability of adequate information, b) reliability of information, and c) the presence of family support; all reflected in outcomes on postoperative pain, faecal continence, bowel function and treatment experience. In order to enhance the trust of patients, clinicians should incorporate those parameters in everyday practice when assisting patients to reach a decision on the choice of surgery for rectal cancer.
This study found that TEMS is associated with good postoperative long-term QoL, and it is the first to report that post-TEMS QoL leads to patients feeling justified in retrospect regarding their decision on the operating choice.
Acknowledgements
The Authors are grateful to all patients who participated in this study.
Footnotes
Authors’ Contributions
Alexandra Koreli: investigation, data curation, formal analysis, writing of original draft, reviewing. George Briassoulis: methodology, interpretation of the data, writing, reviewing and editing. Michail Sideris: investigation, writing, reviewing and editing. Anastas Philalithis: writing, reviewing and editing. Savvas Papagrigoriadis: conceptualization, study design, methodology, resources, writing, reviewing and editing, supervision.
This article is freely accessible online.
Conflicts of Interest
None declared.
- Received January 2, 2021.
- Revision received January 22, 2021.
- Accepted January 27, 2021.
- Copyright© 2021, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.