


Abstract
Background/Aim: Hepatocellular carcinoma represents the most frequently encountered liver malignancy worldwide; however the dimensions of these lesions rarely surpass 20 cm. In such cases surgical treatment might encounter significant technical difficulties. Case Report: We present the case of a 49-year-old patient diagnosed with a 22/25/21 cm left lobe hepatocellular carcinoma. Results: In order to achieve a safe and effective resection total vascular exclusion was needed. Moreover, due to the anatomical relationship between the tumor and the cava vein, an intrathoracic approach of the inferior cava vein was the option of choice. The time of total vascular exclusion was of 26 minutes while the length of surgery was of 210 minutes; meanwhile the estimated blood loss was of 650 ml, while the postoperative outcome was uncomplicated. Conclusion: Total vascular exclusion by double approach might be a safe alternative in order to minimize the risks of severe intraoperative and postoperative complications.
Hepatocellular carcinoma represents the most common malignant tumor affecting the liver, being more frequently encountered in men then in women; therefore, it represents the fifth most common neoplastic disease in male patients and the seventh most commonly encountered neoplasia in female patients (1, 2). Whenever hepatocellular carcinoma is suspected, the first intention treatment which should be taken in consideration is the surgical one; however, the decision of submitting to surgery such patients is taken after meticulous analysis of each case. Not only the dimension of the tumor, but also the liver function and association of other comorbidities represent significant criteria that should be carefully analysed (3, 4).
Case Report
After obtaining the approval of the Ethical Committee no 312/2020, data of the patient were reviewed and presented in the current paper. The 49 year old patient with good general condition self-presented for diffuse abdominal pain, nausea and weight loss. The anamnesis revealed no significant medical antecedents; the patient had been submitted to appendectomy at the age of 15 and presented no history of hepatitis or other chronic viral infection, no previous exposure to toxic agents and denied chronic alcohol consumption. Meanwhile no significant family history of malignant diseases was revealed.
Results
The 49-year-old patient with no significant medical antecedents was initially investigated for diffuse abdominal pain, nausea and weight loss of 15 kg in the last 6 months. The patient was submitted to an abdominal ultrasound which revealed the presence of a large hepatic mass located at the level of the left hepatic lobe measuring 22/25/21 cm while the remnant parenchyma presented normal aspect.
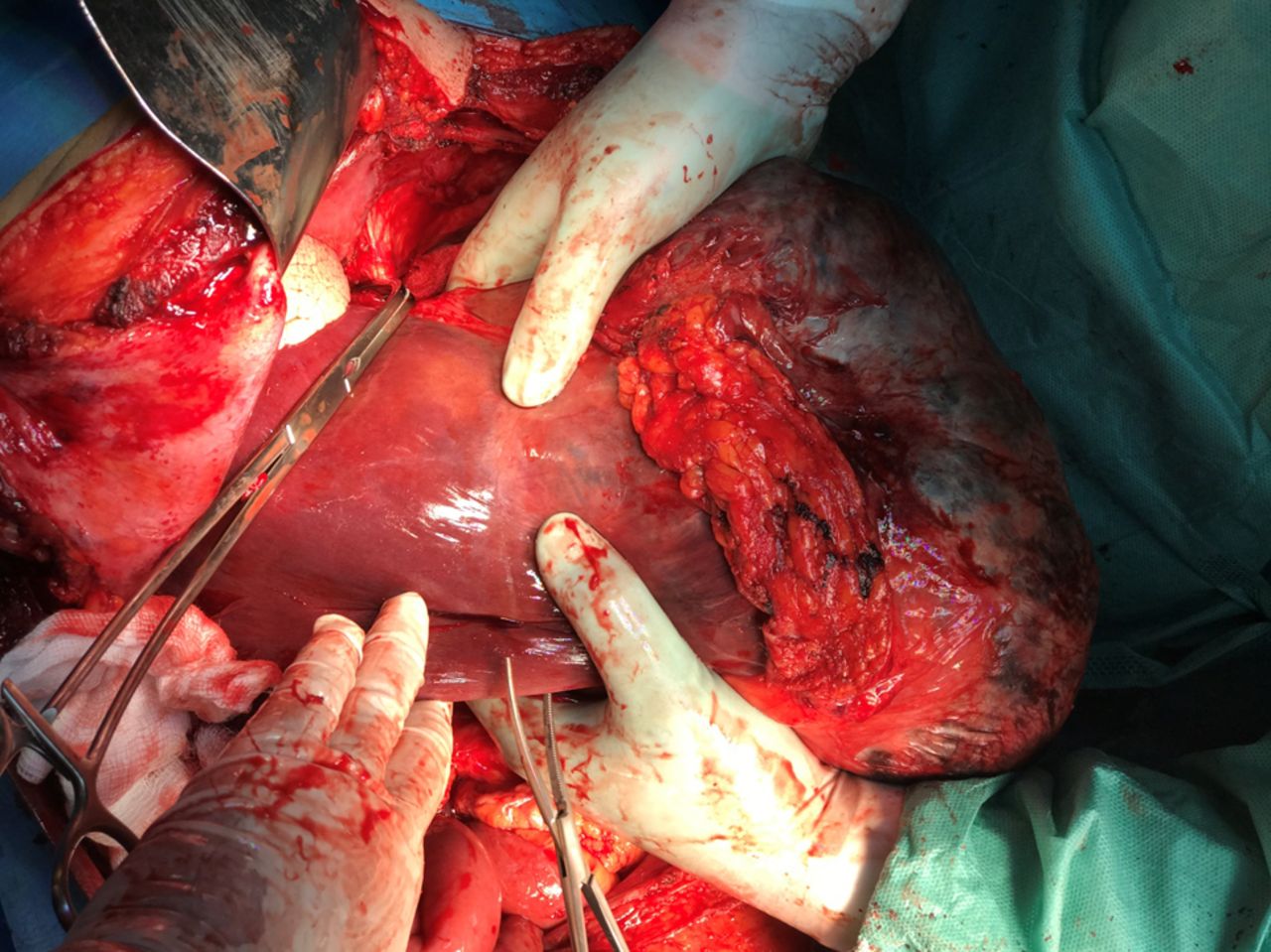
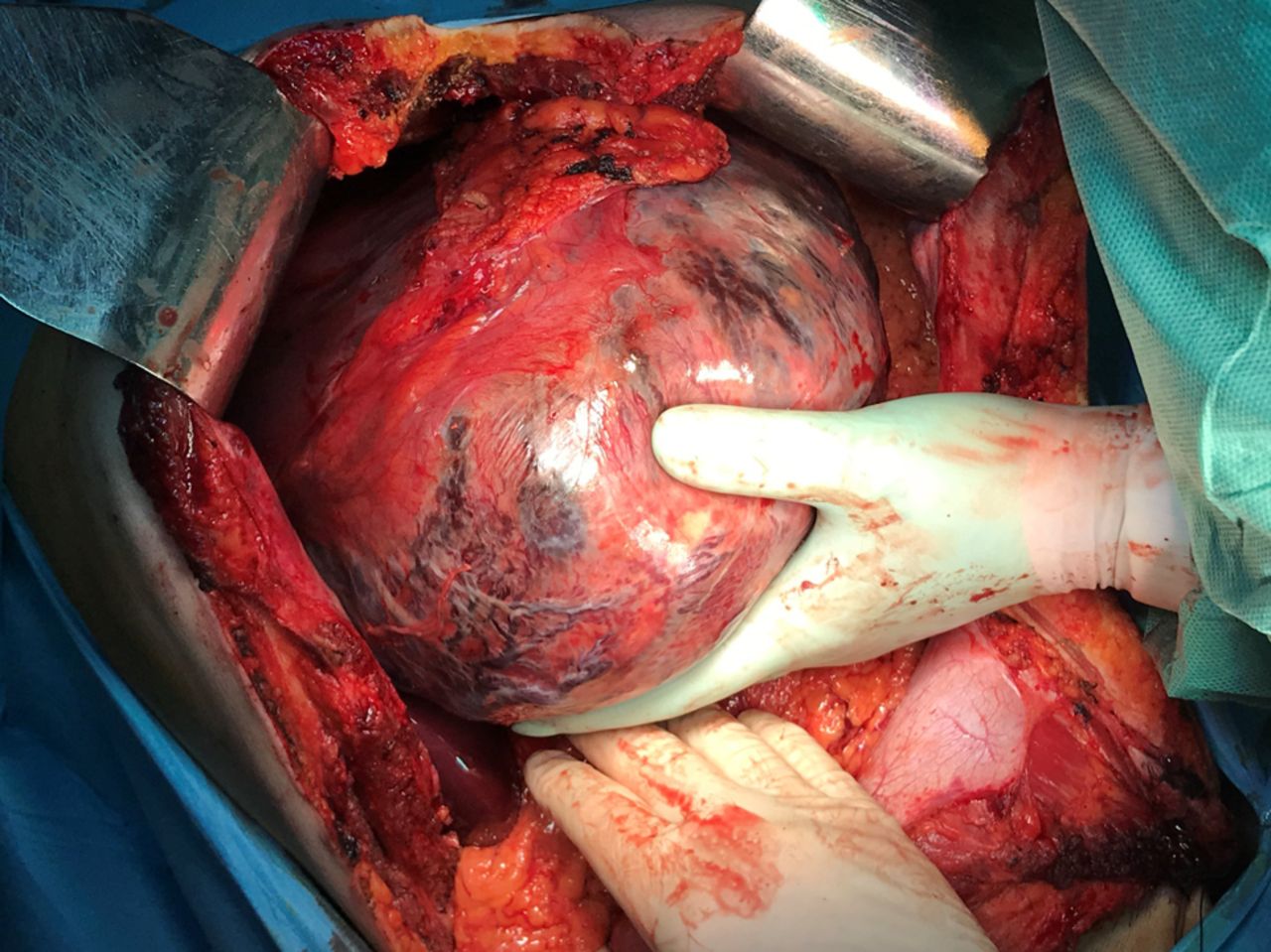
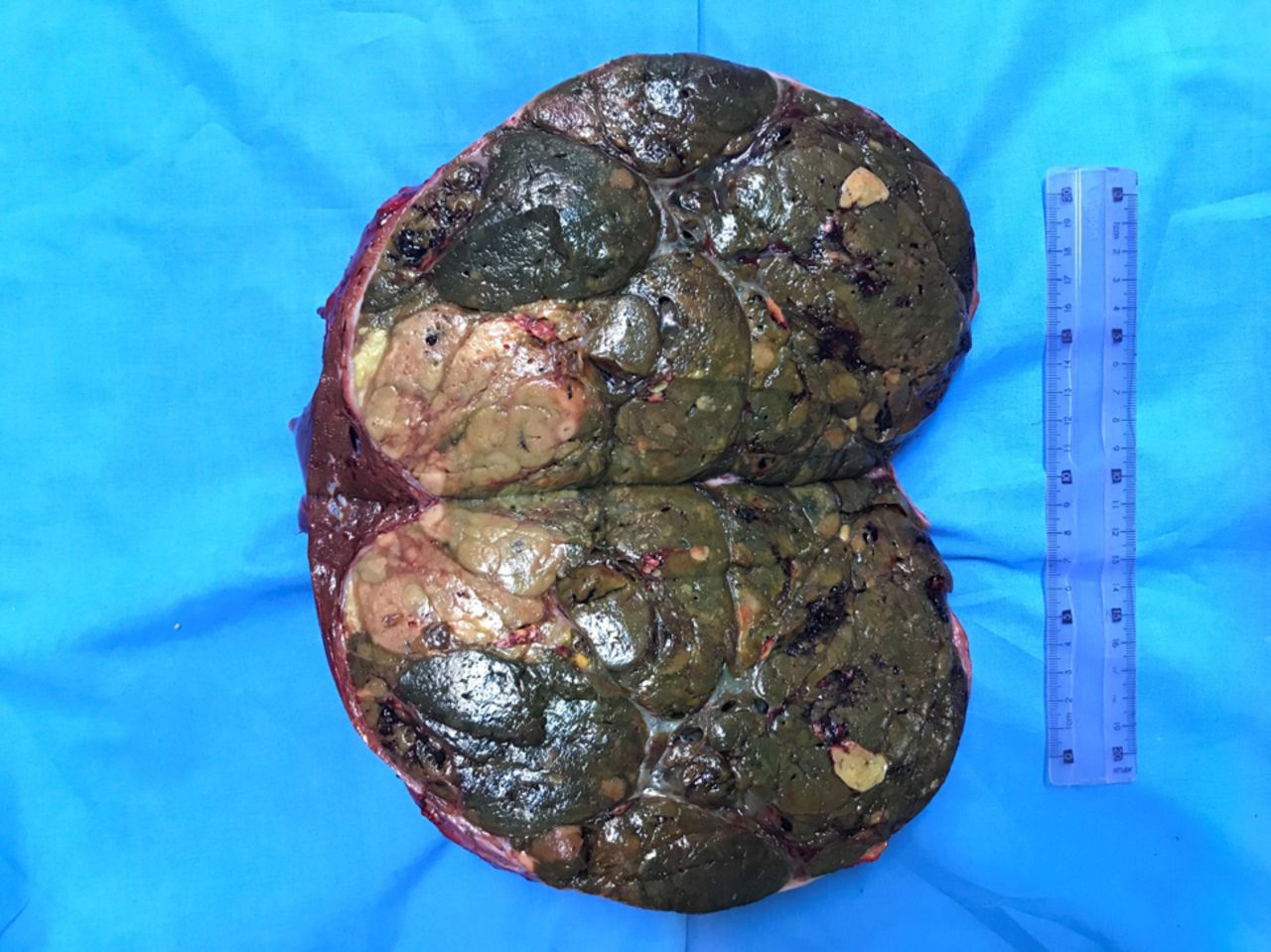
The patient was further submitted to a computed tomography which confirmed the presence of this large hepatic tumor entirely deforming the left lobe, with no other suspect nodules at the level of the remnant parenchyma. Meanwhile, no other pathological aspects were observed; however, the patient was further submitted to upper and lower digestive endoscopy in order to exclude the metastatic origin of the lesion but no lesion was found. The serological tests for hepatitis demonstrated the absence of viral infections while the serum levels of tumoral markers demonstrated the presence of a high level of alpha fetoprotein (AFP) as well as an increased level of serum carcinoembrionic antigen (CEA); therefore the serum levels of AFP were 734 ng/ml while the serum levels of CEA were 598 ng/ml. Due to the fact that the imaging studies demonstrated the presence of a very well developed vascularization of the tumor preoperative biopsy was not performed, the patient being submitted to surgery. Intraoperatively, due to the local anatomical conditions – giant tumor, very well developed vascular network – total vascular exclusion was needed; therefore the abdominal incision was prolonged at the level of the thorax and the diaphragm was sectioned in order to achieve an adequate approach of the suprahepatic cava vein. In these conditions total vascular exclusion by clamping the portal pedicle, the suprahepatic veins and the intrathoracic cava vein were performed. Once this manoeuvre was completed, the left lobe was completely mobilized and atypical left hepatectomy was performed with no intraoperative incidents (Figures 1, 2, 3, 4 and 5). The total time of complete vascular exclusion was 26 minutes while the length of surgery was 210 minutes; meanwhile the estimated blood loss was of 650 ml, the patient being transfused with one unit of erithrocitic mass. The histopathological studies demonstrated the presence of a 24/22/21 cm well differentiated hepatocarcinoma.

Initial intraoperative aspect – large tumor located at the level of the left hemiliver; in order to have a better access on the inferior cava vein the abdominal incision was prolonged at the level of the thorax.
The aspect after complete vascular exclusion and mobilization of the tumor. Preparing the transection of the liver parenchyma.

The final aspect after typical left hepatectomy, before suturing the diaphragm.

The specimen – the left lobe is entirely transformed and included in the tumorl mass.

Transected specimen measuring 24/22/21 cm. The histopathological studies demonstrated the presence of a well differentiated hepatocarcinoma.
Discussion
According to their dimensions, liver tumors are classified as small (<5 cm), big (5-10 cm) and giant (>10 cm); meanwhile, tumors larger than 20 cm are extremely rare (5, 6). In such conditions the treatment of choice remains surgery, especially in otherwise healthy patients presenting no other significant comorbidities (7); however, the surgical technique should be adapted in each case due the anatomical particularities of each case and due to the high risks of developing intra- and postoperative life threatening complications such as fulminant, uncontrollable intraoperative haemorrhage or postoperative acute liver dysfunction due to the low remnant volume of functional parenchyma (9-13). Therefore, in order to prevent the development of an intractable intraoperative bleeding, in the case we presented a total vascular exclusion was the option of choice; moreover, an intrathoracic control of the inferior cava vein was preferred due to the extent of the lesion. As for the risk of postoperative acute liver failure, this complication was prevented in our case due to the presence of a perfectly normal function of the right lobe, fact which was also demonstrated by the presence of preoperative normal serum levels of liver enzymes (6, 8).
In order to minimize the risks of perioperative complications in patients submitted to surgery for such a complex pathology, different study groups such as Barcelona Clinic Liver Cancer (BCLC), American/European Association for the Study of Liver Diseases created different staging and stratification systems aiming to identify cases which could benefit most after surgery (3, 4). Therefore, the most important factors that should be taken in consideration before deciding to perform an extended liver resection for large hepatocellular carcinomas are represented by the performance status, the functionality of the remnant liver, the presence of underlying liver disease (characterised by the presence and degree of portal hypertension), stage of disease and feasibility of complete and safe resection (14).
When it comes to the most severe complications which might develop intraoperatively, particular attention should be paid to the risk of perioperative bleeding. Therefore, it is widely known the fact that intraoperative bleeding and blood transfusions seem to negatively impact on the long-term outcomes, being related with a higher rate of local recurrences and lower rates of disease-free survival (15-17). In this respect, in order to minimize the intraoperative bleeding rate and the necessity of blood transfusion various technical approaches have been proposed, Pringle maneuver, selective, hemiselective or total vascular exclusion being the most commonly investigated surgical techniques (18). Initially imagined by J. H. Pringle in 1908, the maneuver with the same name has been widely used initially in order to reduce the intraoperative blood loss and to diminish the necessity of intraoperative transfusions (19, 20). However, the method seems to have certain disadvantages such as the one of inducing warm ischemia and ischemia reperfusion lesions (21). This fact seems to be correlated with the development of transient increase of the transaminases during the early postoperative period but also with a higher risk of developing liver recurrences. Therefore, it seems that prolongation of the time of warm ischemia might induce local hypoxia and increased cytokine activity increasing in this way the rate of proliferation of hepatic cells and the risk of postoperative recurrence; in this respect decreased recurrence-free survival intervals have been reported in cases submitted to longer times of liver induced ischemia (22-24). One of the most suggestive studies which stated this aspect was conducted by Liu et al. and demonstrated that application of Pringle manoeuvre in excess of 15 minutes was significantly correlated with the rates of local tumor recurrence; this phenomenon was explained by the authors through the fact that prolonged ischemia time increases the vulnerability of the residual liver to delayed damage by activating cells signals for local invasion and distant migration (23). Meanwhile, one should not omit the fact that Pringle manoeuvre controls the inflow at the level of the liver pedicle, without influencing the backflow from the hepatic veins; therefore, close monitoring of the suprahepatic veins is also mandatory if complex resections are taken into consideration. Moreover, in cases presenting large tumoral volumes developed in the close proximity of the hepatic veins and of the inferior cava vein particular attention should be paid when approaching these structures due to the fact that a rupture at this level might lead to development of a severe air embolism and, secondarily, to cardio-pulmonary collapse (26-29). In such conditions in order to prevent haemorrhagic or embolic accidents, attentive dissection of the hepatic veins and cava vein are needed in order to achieve a good control before initiating the resection phase; moreover, in certain cases intrathoracic approach of the cava vein might be needed in order to preserve the oncological safety of the resection (30). In this respect, in the case we came to present a double abdominal and thoracic approach was the option of choice in order to avoid any dilacerations of the venous structures and meanwhile, not to preclude the oncological safety of the procedure.
Conclusion
Total vascular exclusion by using a double approach (thoracic and abdominal approach) might be useful in order to increase the safety and effectiveness of typical hepatic resections for giant hepatocellular carcinoma. Therefore, such combined approach seems to decrease the risks of intraoperative accidents and improve the perioperative outcomes. However, one should not omit the fact that prolongation of the time of warm ischemia might have a negative impact on the long-term outcomes; therefore, this time should be shortened as much as possible, without precluding the safety of the procedure.
Footnotes
Authors’ Contributions
NB, SD and IP performed the surgical procedure; NB, LA and IB reviewed literature data and prepared the draft of the manuscript; IP reviewed the final version of the manuscript. The Authors read and approved the final version of the manuscript.
This article is freely accessible online.
Conflicts of Interest
The Authors have no conflicts of interest to declare regarding this study.
- Received November 3, 2020.
- Revision received December 14, 2020.
- Accepted December 16, 2020.
- Copyright© 2021, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.