


Abstract
Background/Aim: Chronic obstructive pulmonary disease coexisting with non-small-cell lung cancer (NSCLC) was reported to be associated with a longer progression-free survival (PFS) in patients treated with immune checkpoint inhibitors (ICIs). In the present study, we investigated the impact of emphysematous change on the treatment response to ICIs in patients with NSCLC. Patients and Methods: A total of 153 patients with advanced NSCLC who received ICIs (nivolumab, pembrolizumab, or atezolizumab) at our hospital from January 2016 to May 2019 were retrospectively enrolled. Results: According to the Goddard scoring system, 71 (46.4%) patients were classified as having emphysema and 82 (53.6%) as having no emphysema. Multivariate analysis showed that a good performance status and coexisting emphysema (hazard ratio=0.49; 95% confidence intervaI=0.28-0.84; p=0.010) were independent predictors of a better PFS. Conclusion: Recognizing emphysema coexisting with NSCLC may help predict the therapeutic efficacy of ICIs in such patients.
Lung cancer is a major cause of cancer-related death worldwide (1). Although immune checkpoint inhibitors (ICIs) are an approved treatment for advanced non-small-cell lung cancer (NSCLC), primary resistance to ICIs is common (2-4). Expression of programmed cell death ligand 1 (PD-L1) in tumor cells (5), tumor mutation burden (6), and the gene-expression signature of inflammation (7) have emerged as potential predictive biomarkers of the efficacy of inhibitors of the programmed cell death 1 (PD1) axis. However, these biomarkers are insufficient for evaluating a patient’s response to ICIs.
Cigarette smoking is the most common risk factor for lung cancer and chronic obstructive pulmonary disease (COPD) (8). COPD is considered an important risk factor for lung cancer (9) and has been shown to worsen the survival of patients with lung cancer (10). Previous studies revealed that current or former smokers with NSCLC are more likely to respond to ICI therapy (2, 3). Recently, it was reported that the presence of COPD was associated with longer progression-free survival (PFS) in patients with NSCLC treated with ICIs (11-13).
COPD is a heterogeneous syndrome consisting of emphysema, chronic bronchitis, and small airway disease. Emphysema is characterized by abnormal and permanent enlargement of airspaces distal from terminal bronchioles, which can be visualized by computed tomography (CT). To the best of our knowledge, no previous study has evaluated the prognostic significance of pulmonary emphysema in patients with NSCLC treated with ICIs. In the present study, we investigated the impact of emphysematous change on the treatment response to ICIs in patients with NSCLC.
Patients and Methods
Patient population. Patients with advanced NSCLC who received ICIs (nivolumab, pembrolizumab, or atezolizumab) at Hiroshima City Hiroshima Citizens Hospital from January 2016 to May 2019 were retrospectively enrolled in this study. The characteristics and clinical data of the patients before administration of single-agent anti-PD1/PD-L1 were obtained. This study was approved by the Ethical Review Board of Hiroshima City Hiroshima Citizens Hospital (approval number No. 2019-62, July 11, 2019). Patient approval or the requirement for informed consent was waived because this study was performed during routine clinical practice.
Assessments and data collection. We investigated the presence of emphysema on CT scans with a 1-5 mm slice thickness. The CT images at the time of diagnosis were independently evaluated by two pulmonologists who were blinded to the clinical data. The kappa coefficient was used to assess the degree of interrater agreement on specific comparisons. Final decisions were agreed upon by consensus between the two pulmonologists. The presence of emphysema was scored using the Goddard scoring system (14). Briefly, emphysema was scored visually in the bilateral upper, middle, and lower lung fields. The score for each of the six dimensions was calculated according to the percentage of low-attenuation area in each lung field as follows: score 0, <5%; score 1, ≥5%-<25%; score 2, ≥25%-<50%; score 3, ≥50%-<75%; and score 4, ≥75%. In the present study, we defined a total score of more than 8 points as the presence of emphysema. Demographic data, including age, sex, smoking history, and Eastern Cooperative Oncology Group (ECOG) performance status, were collected from electronic medical records.
Study design. PFS was measured from the date of starting ICIs to the date of initial disease progression, death from any cause, or the date last known to be alive without disease progression. Overall survival (OS) was measured from the date of starting ICIs to death from any cause or the date last known to be alive. The objective response rate and disease control rate were evaluated using the Response Evaluation Criteria for Solid Tumors, version 1.1 (15). Immune-related AEs (irAEs) were assessed according to the Common Terminology Criteria for Adverse Events, version 4.0 (16).
Statistical analysis. Data are presented as means±standard deviation or number (%) of patients. Differences between groups were assessed by Student’s t-test and Fisher’s exact test. The Kaplan-Meier method was used to estimate PFS and OS rates, and the log-rank test was used to determine the differences in survival rates. Cox proportional hazards models were used for univariate and multivariate analyses to estimate hazard ratios (HRs) with 95% confidence intervals (CIs). All statistical analyses were performed using EZR software (Saitama Medical Center, Jichi Medical University, Saitama, Japan), a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria); EZR is a modified version of R commander designed to add frequently used statistical functions (17). p-Values of less than 0.05 were considered significant.
Results
Patient characteristics. Of 153 patients with advanced NSCLC, 72 underwent nivolumab monotherapy, 63 underwent pembrolizumab monotherapy, and 18 underwent atezolizumab monotherapy. This was the first exposure to ICIs for all patients. According to the Goddard scoring system, 71 (46.4%) patients were classified as having emphysema and 82 (53.6%) as having no emphysema (Table I). The kappa coefficient of diagnostic agreement was 0.81. No significant difference in age, body mass index, ECOG performance status, or lines of treatment was observed between the two groups. Patients with emphysema had a male predominance and a greater number of tobacco smoking pack-years (p<0.001) compared with patients without emphysema. In addition, they also had a higher prevalence of squamous-cell carcinoma. PD-L1 expression was evaluated in 94 patients, and there was no difference in the PD-L1 tumor proportion score (TPS) between patients with and those without emphysema. Among the patients without emphysema, 17 were positive for mutation of epidermal growth factor receptor (EGFR) gene, and one was positive for anaplastic lymphoma kinase (ALK) gene translocation.
Characteristics of the study patients (N=153).
ICI treatment outcomes of NSCLC in patients with and those without emphysema. The objective response rate was significantly higher in patients with than in those without emphysema (32.4% versus 15.9%; p=0.022), and the disease control rate was also higher in patients with emphysema (67.6% vs. 46.3%; p=0.012) (Table II). In addition, patients with emphysema had a better PFS (median 6.6 versus 2.7 months; HR=0.47, 95% CI=0.32-0.69; p<0.001) and OS (median 19.5 versus 11.6 months; HR=0.58, 95% CI=0.36-0.94; p=0.03) compared with patients without emphysema (Figure 1A). We next examined the impact of emphysema on PFS in the patients with a history of smoking. In the overall cohort, tobacco exposure of 30 pack-years or more was associated with a better PFS (median 4.9 versus 2.7 months, HR=0.58, 95% CI= 0.40-0.86; p=0.006). Notably, patients with emphysema had a better PFS compared with those without, even among those with ≥30 pack-years (median 9.3 versus 3.8 months, HR=0.49, 95% CI=0.30-0.80; p=0.004), although no significant difference in OS was observed (Figure 1B). Multivariate analyses showed that a good ECOG performance status and coexisting emphysema (HR=0.49, 95% CI=0.28-0.84; p=0.010) were independent predictors of better PFS (Table III); however, coexisting emphysema did not remain a statistically significant predictor of OS in the multivariate analysis (Table IV).
Response rates of patients with and without emphysema.
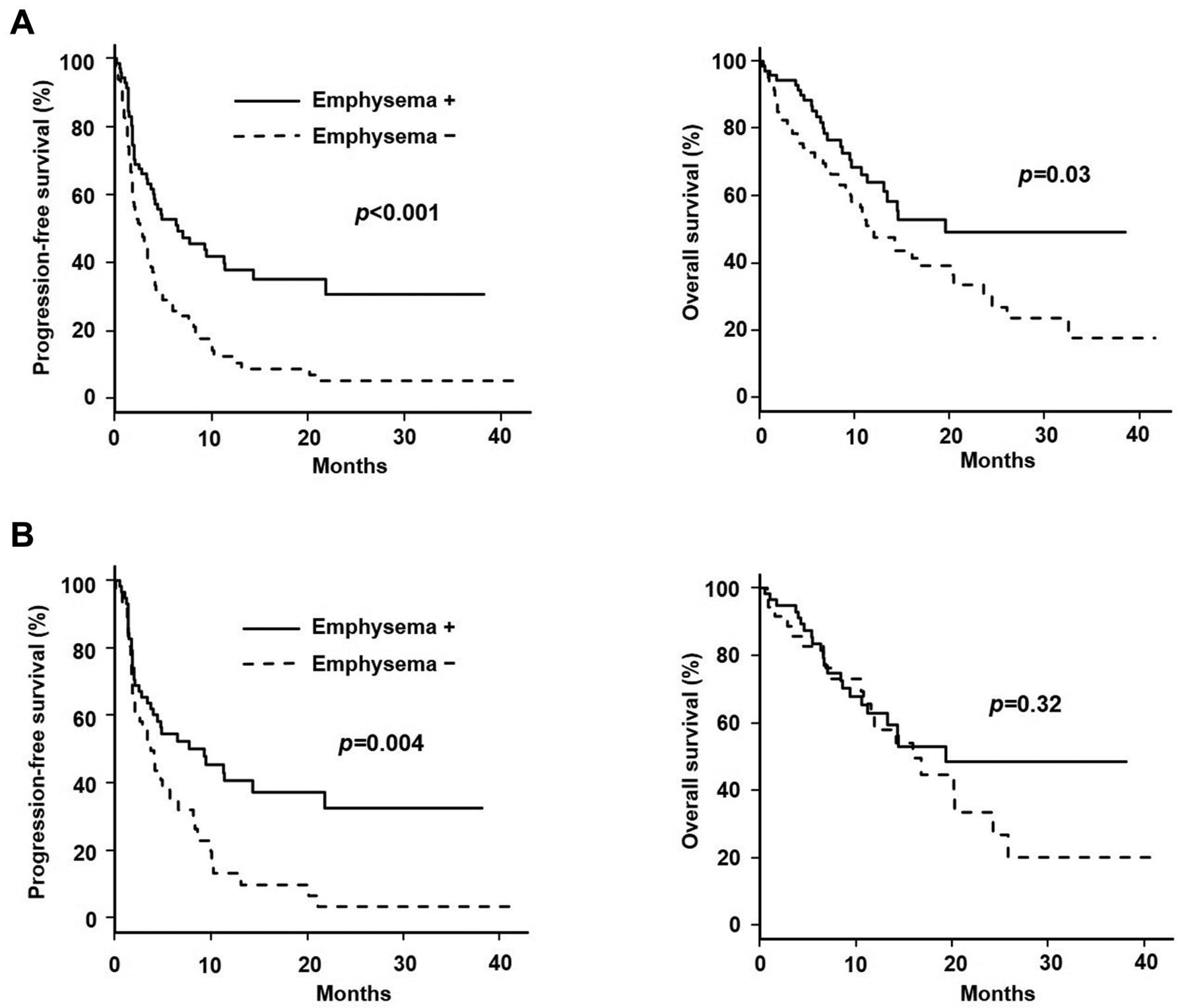
Kaplan-Meier curves of progression-free survival (PFS; left) and overall survival (OS; right) in patients with (+) and those without (−) emphysema in the overall cohort (N=152) (A) and in patients with ≥30 pack-years (N=95) (B).
Univariate and multivariate analyses for progression-free survival.
Univariate and multivariate analyses for overall survival.
Outcome of ICI treatment of patients with NSCLC according to coexisting emphysema and PD-L1 expression. We examined the prognostic significance of coexisting pulmonary emphysema according to PD-L1 expression. The PD-L1 expression status was evaluated in 94 patients. As expected, PFS tended to be longer in patients with PD-L1 TPS≥50% compared with TPS<50% (median 6.0 versus 3.4 months, HR=0.68, 95% CI=0.42-1.12; p=0.128) (Figure 2A). Moreover, patients with both high PD-L1 expression and coexisting emphysema tended to have a longer PFS than that of patients with only one of these factors (Figure 2B).

Kaplan-Meier curves of progression-free survival (PFS) according to the level of programmed cell death ligand 1 (PD-L1) expression (N=94) (A) and PD-L1 expression with/without coexisting emphysema (B). The median PFS (95% confidence intervaI) was 7.1 (4.1–not reached) months in patients with a PD-L1 tumor proportion score (TPS) ≥50% with emphysema (N=29), 4.2 (1.9-9.3) months in patients with a PD-L1 TPS<50% with emphysema (N=25), 3.8 (1.6-6.6) months in patients with PD-L1 TPS≥50% without emphysema (N=21), and 4.1 (0.8-5.8) months in patients with PD-L1 TPS<50% without emphysema (N=19) (B).
Analysis of immune-related adverse events. The irAEs that developed are summarized in Table V. irAEs of any grade were observed in 56 patients (36.6%) and grade 3/4 irAEs in 16 patients (10.5%). However, no difference in the irAE rates was observed between patients with emphysema and those without.
Immune-related adverse events (irAEs) in patients with and without emphysema.
Discussion
The present study showed that emphysema coexisting with NSCLC was associated with a longer PFS and OS and a higher objective response rate in patients treated with ICIs. In addition, the survival benefit of coexisting emphysema in patients with NSCLC treated with ICIs persisted even after adjustment for all relevant covariates. Moreover, no difference in the rates of irAEs was observed between patients with and those without emphysema.
To our knowledge, this is the first study to show an association between coexisting emphysema and an improved response to ICIs. We used a visual CT scoring system to assess the presence of emphysema. Previous studies have reported that visual CT scores are correlated with pathological findings (18) and respiratory functions (14, 19). Notably, the Goddard semiquantitative scoring system can be performed easily and quickly (14). Moreover, almost all patients with lung cancer undergo chest CT scans for diagnosis and staging during the initial evaluation. Thus, it may be clinically useful to identify emphysema using visual CT scores, such as the Goddard scoring system, in predicting the efficacy of ICIs in patients with NSCLC.
The mechanism underlying the better outcome of emphysematous NSCLC patients treated with ICIs remains unclear. However, a few mechanisms underlying an improved outcome in patients with COPD treated with ICIs have been proposed. Firstly, CD4+ T-cell differentiation is skewed toward the interferon-γ-producing T-helper type 1 phenotype in the setting of COPD (20). Th1 immunity in a subset of patients with COPD may be responsible for a better ICI treatment outcome because the existence of an interferon-γ-related gene signature was recently shown to predict a favorable anti-PD1 treatment response (21). Secondly, it was reported that patients with NSCLC with COPD displayed tumor-infiltrating T-lymphocyte exhaustion, identified by enhanced immunostaining of PD1 and T-cell immunoglobulin mucin 3 in CD8+ cells (12, 20). Thus, immune activity was suggested to be enhanced in patients with NSCLC with COPD. We speculate that high ICI efficacy in NSCLC is obtained in patients with emphysema by the same mechanism as in patients with COPD.
Current or former smokers with NSCLC are more likely to respond to ICI therapy (2, 3), and similar results were found in the present study. Notably, PFS was better in patients with emphysema than in those without even among the patients with a smoking history of 30 or more pack-years. In addition, multivariate analysis showed that emphysema had a stronger association with PFS than did smoking status. A previous study reported that COPD and tobacco smoking have a synergistic impact on CD8+ tumor-infiltrating T-lymphocyte exhaustion and on the prognostic value of immune cells (12), supporting our results.
It has been reported that patients with high PD-L1 expression in tumor cells are more likely to respond to treatment with ICIs (2, 3), and similar results were found in the present study. The relationship between PD-L1 expression and emphysema remains unclear, even though some studies (22, 23) have evaluated this. In the present study, there was no difference in PD-L1 expression between patients with and those without emphysema. Therefore, we speculate that the PD-L1 expression status and emphysema are independent prognostic factors for PFS in patients with NSCLC treated with ICIs. In our study, patients with both high PD-L1 expression and emphysema tended to have a longer PFS compared with patients with only one of these factors. Treatment with ICIs may have a favorable antitumor effect in these patients.
In the present study, no difference in the rate of irAEs was observed between patients with emphysema and those without. Previous studies indicated that the presence of emphysema is not associated with the occurrence of ICI-induced interstitial lung disease (24, 25). Thus, the presence of emphysema is likely not a factor hindering treatment with ICIs.
The present study has several limitations. Firstly, this was a retrospective, single-center study with a small sample size. Secondly, ICIs have shown minimal therapeutic benefit in patients with EGFR mutations (2, 4, 26). In the present study, a higher proportion of the patients without emphysema had EGFR mutations. However, the driver mutation status, such as EGFR gene mutations and ALK gene translocation, was not associated with PFS in the multivariate analysis. Thirdly, we used the Goddard scoring system to assess the existence of emphysema. Although this method is simple and can be performed quickly, visual inspection is thought to be affected by interobserver and intraobserver variabilities. Therefore, additional detailed examinations using quantitative standardized assessments with computer algorithms are required to assess the existence of emphysema.
Conclusion
In this study, emphysema coexisting with NSCLC was associated with longer PFS and OS and a higher response rate to ICI treatment. In addition, emphysema had a stronger association with PFS than did smoking status. Therefore, recognizing coexisting emphysema may help predict the therapeutic efficacy of ICIs in patients with NSCLC.
Footnotes
Authors’ Contributions
Y.T and H.S. devised the project and main conceptual ideas. Y.T and T.N. performed the retrospective chart review, carried out radiological measurements, and conducted the statistical analysis. Y.F, S.M, and K.M. supervised the project. All Authors gave final approval for publication.
This article is freely accessible online.
Conflict of Interest
The Authors declare no conflicts of interest associated with this study.
- Received September 30, 2020.
- Revision received October 13, 2020.
- Accepted October 14, 2020.
- Copyright© 2021, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}
{kind=link}