


Abstract
Background/Aim: Adjuvant chemotherapy for high-risk Stage II colorectal cancer (CRC) is weakly recommended; however, no consensus exists on “high-risk” definition. Prognostic biomarker identification is important for selecting patients with poor prognosis who may benefit from adjuvant chemotherapy. Materials and Methods: Using Microarray data analyses, ELF3 was identified as a candidate gene highly expressed in Stage II CRC with distant recurrences. ELF3 mRNA expression in 168 Stage II CRC patients was subjected to quantitative RT-PCR analysis and ELF3 protein expression in 185 patients was quantified by immunohistochemical analysis. The relationship between mRNA and protein expression levels and patient characteristics were also investigated. Results: The overall recurrence rate and relapse-free survival were significantly poorer in the ELF3 high-expression than the low-expression group at the mRNA and protein levels. High ELF3 mRNA and protein expression levels were independent poor prognostic factors. Conclusion: High ELF3 expression was associated with recurrence of Stage II.
The incidence of colorectal cancer (CRC), which is the second leading cause of cancer-related death in Japan, continues to increase worldwide (1-3). The tumor-node-metastasis (TNM) staging system of the International Union Against Cancer is the gold standard to determine an appropriate therapeutic strategy, including adjuvant chemotherapy (4-6). The risk of recurrence is an important factor to consider when choosing a postoperative treatment strategy and is therefore being intensively studied worldwide. Postoperative adjuvant chemotherapy for Stage III CRC patients is considered the standard treatment to improve survival. However, adjuvant chemotherapy is only weakly recommended for high-risk Stage II CRC, as there is currently no consensus on the definition of high-risk Stage II CRC (7-15). The prognosis of high-risk Stage II CRC is poor, similar to that of Stage III disease. Hence, the efficacy of postoperative adjuvant chemotherapy or more intensive surveillance is currently being investigated to improve the prognosis of these patients, and research is ongoing to identify factors that define high-risk disease. According to the American Society of Clinical Oncology guidelines, risk factors for recurrence of Stage II CRC include the dissection of less than 12 lymph nodes, T4, perforation, poorly differentiated adenocarcinoma, signet ring cell carcinoma, and mucinous carcinoma (16). According to the European Society for Medical Oncology guidelines, risk factors for the recurrence of Stage II CRC include T4, poorly differentiated gland cancer or undifferentiated carcinoma, vascular invasion, lymphatic invasion, perineural invasion, initial symptoms of intestinal obstruction or intestinal perforation, and dissection of less than 12 lymph nodes (17). Meanwhile, exploration of the risk classification for Stage II CRC patients is ongoing internationally. The aim of the study was to identify useful biomarkers for the selection of subgroups of Stage II CRC with poor prognosis using comprehensive data of gene copy number combined with gene expression analysis.
Materials and Methods
Identification of candidate genes by microarray gene expression analysis. Microarray data from a previous study were used in the current study (18). The gene expression and the copy number data were deposited in the Gene Expression Omnibus repository [GSE64258, GSE64256 (gene expression), and GSE64257 (copy number analysis)]. Prognosis information for Stage II CRC in the previously analyzed microarray data was updated and re-analyzed. The copy number and gene expression data were compared between the two groups to identify candidate genes as potential biomarkers of the recurrence of Stage II CRC. Genes with a gain in copy number involved in disease recurrence were identified using logistic regression analysis (p<0.05), while genes that were significantly upregulated in disease recurrence were identified using the Welch t-test (p<0.05). Genes that were common to both groups were selected as candidates for further analysis. Finally, E74-like E26 transformation-specific transcription factor 3 (ELF3) was selected as the target gene for further analysis in the present study.
Patients. From 2009 to 2014, a total of 185 patients underwent curative surgery for Stage II CRC at the Tokyo Medical and Dental University (Tokyo, Japan). The median follow-up time for these patients was 59 (range=1-113) months. Tissue samples from 168 patients, including 27 with disease recurrence, were used for quantitative reverse transcription polymerase chain reaction (qRT-PCR) analysis. In addition, formalin-fixed paraffin-embedded samples were available for all 185 patients, including 32 with disease recurrence, and used for immunohistochemical (IHC) analysis. Clinical data were obtained from the medical records of each patient, and histopathological evaluations were assessed by reference to the TNM criteria of the Union for International Cancer Control, 8th edition. The study protocol was approved by the Institutional Review Board of Tokyo Medical and Dental University and conducted in accordance with the tenets of the Declaration of Helsinki. Informed consent was obtained from all patients prior to inclusion in this study.
Quantitative reverse transcription polymerase chain reaction. Total RNA (10 ng) was isolated from bulk samples of cancer and adjacent non-neoplastic tissues and reverse-transcribed into complementary DNA (cDNA) using a High Capacity cDNA Reverse Transcription kit (Applied Biosystems, Foster City, CA, USA). A TaqMan gene expression assay (Applied Biosystems: ELF3; Hs00963877_g1, ACTB; Hs99999903_ml) was used to investigate the expression of ELF3, with β-actin as an internal control. The qRT-PCR reaction was performed using TaqMan Universal PCR Master Mix (Applied Biosystems). All calculated concentrations of the target genes were normalized to the amount of the endogenous reference using the comparative Ct (ΔΔCt) method for relative quantification with Relative Quantification Study Software (StepOne Realtime PCR System, Applied Biosystems). Each assay was performed in duplicate. Gene expression was analyzed with the use of the ratio of cancer tissue expression to non-neoplastic tissue expression (T/N ratio).
Immunohistochemical (IHC) analysis. IHC analysis of ELF3 was conducted using formalin-fixed paraffin-embedded tissue blocks from each patient. The slides were deparaffinized in xylene and rehydrated with a series of graded concentrations of ethanol. Antigen retrieval by microwave was conducted for 15 min in Antigen Retrieval Buffer (100× ethylenediaminetetraacetic acid buffer, pH 8.0; Abcam, Cambridge, UK) at 98°C. Afterward, the slides were incubated in a solution of 3% hydrogen peroxide in 100% methanol for 15 min at room temperature in order to quench endogenous peroxidase activity and then incubated overnight with rabbit polyclonal antibody against ELF3 (dilution, 1:100; Sigma-Aldrich Corporation, St. Louis, MO, USA) at 4°C. The slides were then incubated with peroxidase-labeled antibody (Histofine® Simple Stain™ MAX PO (MULTI); Nichirei Bioscience, Inc., Tokyo, Japan) for 30 min at room temperature. Peroxidase activity was detected with Histofine Simple Stain DAB Solution (Nichirei BioScience, Inc.) for 20 min at room temperature. Finally, the slides were counterstained with 1% Mayer’s hematoxylin for 12 s. Staining intensity was graded by two independent observers who were blinded to the patient information.
Statistical analysis. All statistical analyses were performed using IBM SPSS Statistics for Windows, version 22.0. (IBM Corporation, Armonk, NY, USA). The Mann-Whitney U-test and the Chi-square test were used where appropriate to identify significant differences between groups. The overall recurrence rate (ORR) was defined as the rate of any recurrence after surgical resection. Relapse-free survival (RFS) was defined as the time from the date of surgical resection to any recurrence or death other than from the primary cancer. Overall survival (OS) was defined as the time from the date of surgery to death from any cause. Survival curves were plotted using the Kaplan-Meier method, and differences between the curves were estimated using the log-rank test. Potential prognostic factors were screened using univariate and multivariate analyses with a Cox proportional hazards model. A Cox model was used to estimate the hazard ratio (HR) and the corresponding 95% confidence interval (CI). A probability (p) value of <0.05 was considered statistically significant.
Results
Gene expression and copy number analyses for identification of candidate genes. Comprehensive analysis of gene expression and copy number showed that 396 genes were up-regulated in the recurrence group compared to the non-recurrence group, and 72 genes had gains in copy number. Seven genes were common in both groups. Among these genes, ELF3 was selected as a candidate gene because it is reported to be up-regulated or down-regulated in other solid tumors, although the clinical significance of this gene in CRC remains unclear. Therefore, ELF3 was the focus of the subsequent analyses.
Validation of ELF3 mRNA expression. qRT-PCR analysis of ELF3 mRNA expression showed that the T/N ratio of the recurrence group was marginally higher than that of the non-recurrence group (p=0.093).
Relationship between ELF3 mRNA expression and prognosis of CRC. For statistical evaluation purposes, the 168 samples used for qRT-PCR analysis were allocated to one of the following two groups based on the cutoff value determined from a receiver operating characteristic (ROC) curve in order to predict recurrence after surgery: a high-expression group (T/N value>1.2, n=67) or a low-expression group (T/N value<1.2, n=101) (Table I). The ORR was significantly higher in the high ELF3 mRNA expression group than in the low-expression group (Figure 1a). Univariate analysis indicated that lymphatic invasion (p=0.001) and ELF3 mRNA expression (p=0.01) were significantly associated with the ORR. Multivariate analysis indicated that ELF3 overexpression is an independent and significant poor prognostic factor of the ORR (p=0.017; RR=3.150; 95% CI=1.230-8.068) (Table II). RFS was significantly lower in the high mRNA ELF3 expression group than in the low mRNA expression group (Figure 1b). Univariate analysis indicated that lymphatic invasion (p<0.001), preoperative carcinoembryonic antigen (CEA) level (p=0.021), number of harvested lymph nodes (p=0.038), and ELF3 mRNA expression (p=0.037) were significantly associated with RFS. Multivariate analysis indicated that ELF3 mRNA overexpression is an independent and significant poor prognostic factor of RFS (p=0.036; RR=1.965; 95% CI=1.045-3.697). OS was significantly lower in the high ELF3 mRNA expression group than in the low mRNA expression group (Figure 1c). Univariate analysis indicated that age (p=0.024), preoperative CEA level (p=0.037), and number of harvested lymph nodes (p=0.012) were significantly associated with OS. ELF3 mRNA expression was not significantly associated with OS. All patients with high microsatellite instability (MSI) had no recurrence, therefore MSI was excluded from further analysis.
Correlation between clinicopathological features and ELF3 mRNA expression in Stage II CRC.

Bar graph showing overall recurrence rate (ORR) (a) and Kaplan-Meier curves showing relapse-free survival (RFS) (b) and overall survival (OS) (c) of 168 Stage II CRC patients by ELF3 mRNA expression level.
Univariate and multivariate analyses of clinicopathological features affecting the ORR, RFS, and OS based on ELF3 mRNA levels.
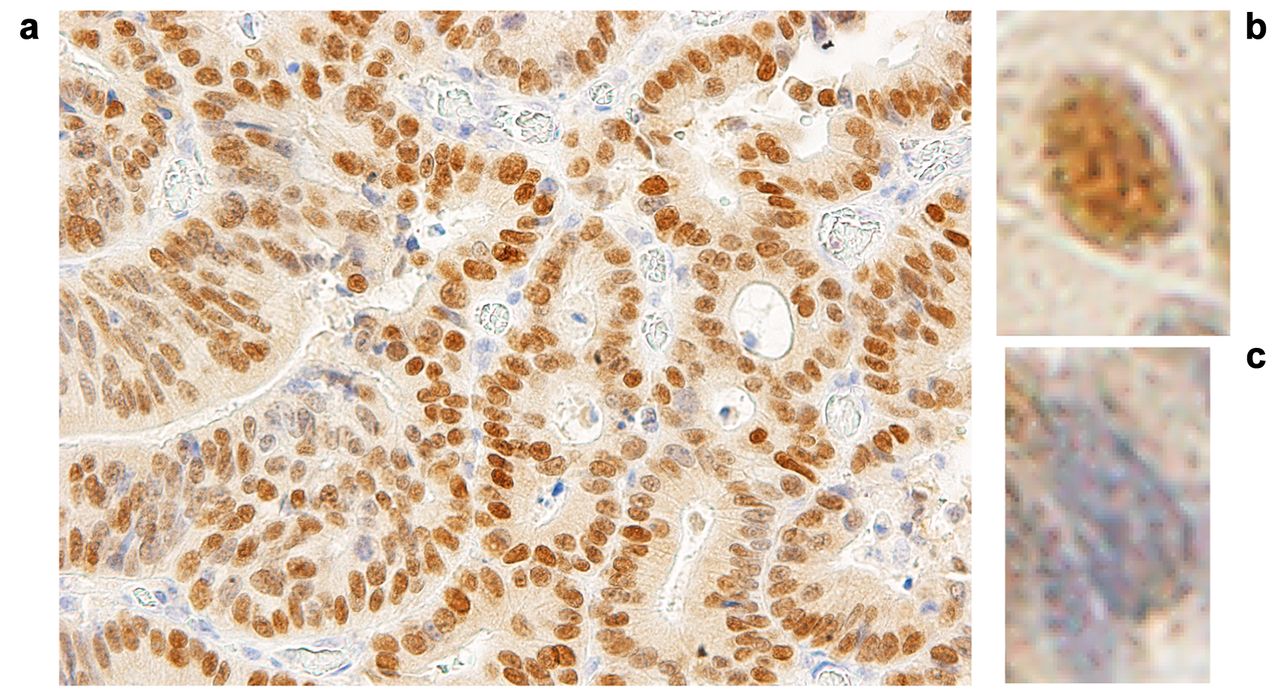
Validation of ELF3 protein expression. IHC analysis indicated that ELF3 was located in the nuclei of CRC cells and staining for ELF3 at the invasive tumor front tended to be weak, but tended to be strong at the ulcer randwall Therefore, staining intensity was graded at three sites with strong expression in each tumor ulcer randwall: blue staining of the nucleus was considered negative, while the lack of blue staining was considered positive (Figure 2). The average scores of three positively stained sites (0-100) was adopted as the protein score. IHC analysis showed that ELF3 protein expression was significantly higher in the recurrence group than in the non-recurrence group (p<0.001) (Figure 3a).

Representative immunostaining for ELF3 in ulcer randwall of colorectal cancer: (a) ulcer randwall (´400), (b) positive staining, (c) negative staining.

Bar graph showing overall recurrence rate (ORR) (a) and Kaplan-Meier curves showing relapse-free survival (RFS) (b) and overall survival (OS) (c) of 185 Stage II CRC patients by ELF3 protein expression level.
Relationship between expression of ELF3 protein and prognosis. The 185 samples subjected to IHC analysis were allocated to one of the two following groups based on the cutoff value determined from a ROC curve to predict recurrence after surgery: a high-expression group (IHC score >40, n=43) or a low-expression group (IHC score <40, n=142) (Table III). ORR was significantly higher in the high ELF3 protein expression group than in the low protein expression group (Figure 3a). Univariate analysis indicated that lymphatic invasion (p<0.001) and ELF3 protein expression (p<0.001) were significantly associated with the ORR. Multivariate analysis indicated that ELF3 protein overexpression is an independent and significant poor prognostic factor of the ORR (p<0.001; RR=30.701; 95% CI=9.769-96.488) (Table IV). RFS was significantly lower in the high ELF3 protein expression group than in the low protein expression group (Figure 3b). Univariate analysis indicated that lymphatic invasion (p<0.001), preoperative CEA level (p=0.004), number of harvested lymph nodes (p=0.006), and ELF3 protein expression (p<0.001) were significantly associated with RFS. Multivariate analysis indicated that ELF3 protein overexpression is an independent and significant prognostic factor of RFS (p<0.001; RR=6.648; 95% CI=3.519-12.559). OS was significantly lower in the high ELF3 protein expression group than in the low protein expression group (Figure 3c). Univariate analysis indicated that age (p=0.005), preoperative CEA level (p=0.025), number of harvested lymph nodes (p=0.002), and ELF3 protein expression (p=0.016) were significantly associated with OS. Multivariate analysis indicated that ELF3 protein overexpression is an independent and significant poor prognostic factor of OS (p=0.003; RR=3.085; 95% CI=1.450-6.563).
Correlation between clinicopathological features and ELF3 protein expression in stage II CRC.
Univariate and multivariate analyses of clinicopathological features affecting the ORR, RFS, and OS based on ELF3 protein levels.
Discussion
This study is the first to demonstrate the clinical significance of ELF3 expression to predict recurrence of Stage II CRC. Gene expression and copy number analyses identified an association between ELF3 expression and disease recurrence. High ELF3 expression was an independent and important poor prognostic factor of ORR and RFS after curative surgery for Stage II CRC. Similar results were obtained at both the mRNA and protein levels.
The ELF3 gene, a E26 transformation-specific member of the ETS family of transcription factors, is located on chromosome 1q32.1 and encodes a protein consisting of 371 amino acid residues. Analysis of the mRNA expression profile of the ELF3 gene across normal human tissues showed strong expression in the gastrointestinal tract (19). Diseases associated with ELF3 include cancers of the bladder, ovary, biliary tract, stomach, cervix, breast, prostate, lung, liver, and colon (20-27, 31). These studies reported that mutations to the ELF3 genes have a tumor suppressive role in some cancers. Conversely, other groups reported high ELF3 expression in cancer cells.
ELF3 has been suggested to be involved in CRC malignancy via β-catenin accumulation and regulation of TGFβR II. Aberrant regulation of the Wnt/β-catenin pathway plays a key role in colorectal carcinogenesis, as many cases of CRC are characterized by β-catenin accumulation. It has been reported that overexpression of ELF3 induces β-catenin accumulation in both the nucleus and cytoplasm without input from the Wnt/β-catenin pathway (28, 29). β-catenin accumulates in the cytoplasm and nucleus of colon cancer cells; therefore, overexpression of cancer-related genes, such as cyclinD1 and c-myc, induces abnormal cell proliferation (30). Abnormal cell proliferation promotes cancer growth. Therefore, ELF3 overexpression is considered to be a poor prognostic factor in Stage II CRC. Wang L et al. reported that suppressing ELF3 in CRC cells attenuates β-catenin signaling and decreases cell proliferation, migration and survival, and targeting ELF3 in xenograft tumors suppressed tumor progression in vivo (28). It is considered that the high expression of ELF3 increases the intracellular accumulation of β-catenin, although high expression of β-catenin could not be confirmed in ELF3 protein high-expression patients by IHC staining in the present study. The detailed mechanism of β-catenin accumulation due to overexpression of ELF3 is expected to be elucidated in the future. Nakarai et al. reported that ELF3 may be practical to detect lymph node metastasis of CRC, and ELF3 controls the intestinal epithelial differentiation by regulation of the expression of transforming growth factor β receptor type II (TGFβR II), which behaved as a tumor suppressor. ELF3 activated the TGFβR II promoter and regulates TGFβR II, which is connected to extracellular matrix remodeling and tumorigenesis (31). Although our study did not examine the association between TGFβR II and ELF3, it is worth investigating the association in clinical tissues of CRC in the future. Overexpression of ELF3 may have been related to poor prognosis of Stage II CRC via β-catenin and TGFβR II.
Recent studies have been conducted to identify useful biomarkers other than clinicopathological factors. Although MSI status, the Oncotype DX Colon Cancer Assay, and the ColoPrint genomic classifier have been applied for the evaluation of genes as predictors of recurrence, none of these technologies have been clinically applied in Japan (32-38). A study on the validity of the recurrence score generated by the Oncotype DX Colon Cancer Assay in patients following curative resection of Stages II and III colon cancer (SUNRISE study) is currently underway in Japan. A prospective observational study on risk stratification by ColoPrint (PARSC study) of 1,200 patients with Stage II/III CRC, including 575 with Stage II disease, is ongoing in Europe, the USA, and Asia. The results of the present study showed that high ELF3 expression might be a high-risk factor for recurrence of Stage II CRC patients and a potential candidate marker for preoperative adjuvant chemotherapy to decrease the rate of recurrence.
The primary limitation of this study was the small number of samples of Stage II CRC with recurrence because the recurrence rate of Stage II CRC recurrence is not particularly high. A further verification study with a larger number of Stage II CRC patients with recurrence is needed to confirm our results.
In conclusion, the results of the present study showed that ELF3 expression was significantly increased in the Stage II CRC recurrence group, suggesting the potential of the ELF3 protein as a prognostic factor of recurrence. The focus of this study was highly expressed genes and the identified gene was further investigated as a biomarker for use in clinical practice, such as preoperative endoscopic biopsy samples. In the future, it is expected that ELF3 will be confirmed as a candidate biomarker, while attempts are being made to classify and stratify recurrence risk using other technologies, such as the Oncotype DX genomic test.
Acknowledgements
The Authors wish to thank Ms. Yoko Takagi and Ms. Junko Inoue (Department of Specialized Surgeries, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, Bunkyo-ku, Tokyo 113-8519, Japan) for their excellent technical assistance.
Footnotes
Author’s Contributions
AT, TI, SO and HU were involved in the conception and design of the study, and development of the methodology. AT performed the experiments and collected clinicopathological data. AT, SW, FM and TT analyzed the results. AT, TI and SO edited the manuscript. AK, SY, TM assisted with all assays. TI, MT, HU, YK supervised the study. All Authors have read and approved the final manuscript.
This article is freely accessible online.
Conflicts of Interest
The Authors declare that they have no conflicts of interest.
- Received September 11, 2020.
- Revision received September 26, 2020.
- Accepted September 30, 2020.
- Copyright© 2021, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.