


Abstract
Hearing loss is one of the major worldwide health problems that seriously affects human social and cognitive development. In the auditory system, three components outer ear, middle ear and inner ear are essential for the hearing mechanism. In the inner ear, sensory hair cells and ganglion neuronal cells are the essential supporters for hearing mechanism. Damage to these cells can be caused by long-term exposure of excessive noise, ototoxic drugs (aminoglycosides), ear tumors, infections, heredity and aging. Since mammalian cochlear hair cells do not regenerate naturally, some therapeutic interventions may be required to replace the damaged or lost cells. Cochlear implants and hearing aids are the temporary solutions for people suffering from severe hearing loss. The current discoveries in gene therapy may provide a deeper understanding in essential genes for the inner ear regeneration. Stem cell migration, survival and differentiation to supporting cells, cochlear hair cells and spiral ganglion neurons are the important foundation in understanding stem cell therapy. Moreover, mesenchymal stem cells (MSCs) from different sources (bone marrow, umbilical cord, adipose tissue and placenta) could be used in inner ear therapy. Transplanted MSCs in the inner ear can recruit homing factors at the damaged sites to induce transdifferentiation into inner hair cells and ganglion neurons or regeneration of sensory hair cells, thus enhancing the cochlear function. This review summarizes the potential application of mesenchymal stem cells in hearing restoration and combining stem cell and molecular therapeutic strategies can also be used in the recovery of cochlear function.
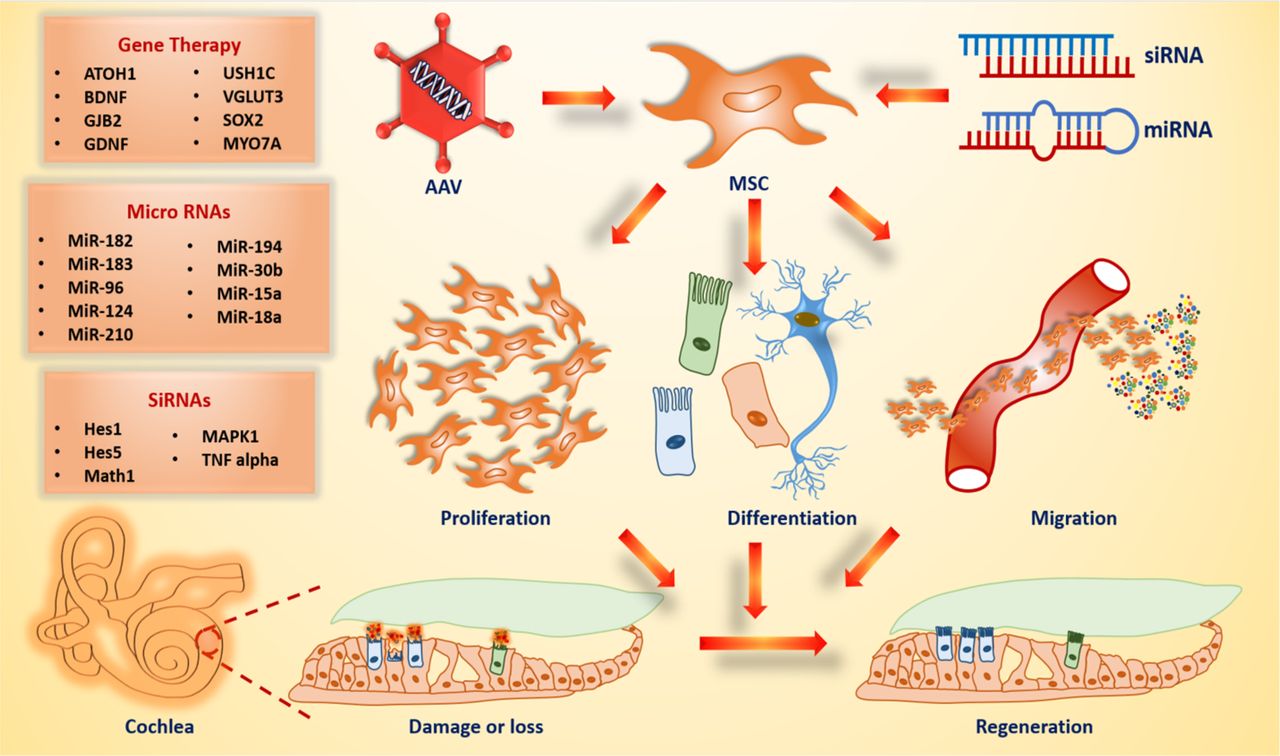
Ear is the sensitive organ that senses soundwaves from the external environment and transmits them to the inner ear through external auditory meatus. It is composed of three compartments outer, middle and inner ear. Each compartment has its specific role in the hearing process. The major hearing problems arise due to damage or injury in the middle ear and inner ear. Conductive hearing loss (CHL) and sensorineural hearing loss (SNHL) are the main categories of hearing loss. Conductive hearing loss is the problem of conducting sound waves in the middle ear (eardrum and auditory ossicles), which primarily caused by the earwax or fluid accumulation in the ear canal, perforated eardrum, benign tumors, severe middle and external ear trauma and chronic otitis media (1). Sensorineural hearing loss occurs when there is damage in the inner ear hair cells or insufficient function of hair cells and auditory neurons or impaired function of auditory neural pathways (2). Frequent exposure to loud noises, intake of ototoxic medications, viral infections, tumors, presbycusis (age-related hearing loss), heredity and malformation of the inner ear are the major causes of SNHL. No major treatments are available for SNHL. However, some external devices, including hearing aids and cochlear implants are available for improving auditory dysfunctions. Currently, novel approaches such as stem cell therapy, gene therapy, delivering small interfering RNA (siRNA) and microRNA (miRNA) molecules to the inner ear have been emerged to restore the abnormal hearing function (Figure 1). In inner ear regenerative medicine, mesenchymal stem cells (MSCs) are being a better therapeutic option due to their significant properties including self-renewal, multipotency, paracrine action, immunomodulatory function and wound healing (3). Therefore, this review mainly focuses on the application of mesenchymal stem cells in inner ear hearing regeneration. Even though the mesenchymal stem cell approach shows beneficial outcome in hearing regeneration, a combination strategy of MSCs with different molecular approaches also currently evolved in hearing loss studies. Thus, we also highlighted MSCs in gene therapy, siRNA and miRNA for inner ear regeneration.

Application of gene manipulation techniques in mesenchymal stem cell enhances the possibility of regeneration of damaged or lost hair cells in the cochlea by inducing proliferation, differentiation, migration or secretion of paracrine factors. The list of important genes, microRNAs and siRNAs are used to study the hair cell regeneration (left).
Inner Ear Regeneration. Cochlea is an important portion of inner ear structures, consists of specific numbers of small specialized cells called hair cells (HCs) and spiral ganglion neurons (SGNs), which are essential for transducing sound stimuli into electrical signals. Many cells in the body are able to regenerate themselves when injury occurs. But mammalian cochlear hair cells lack regenerative capacity, once they are impaired, their growth is irreversible and may end up with permanent hearing loss (4). Cochlea is mainly comprised of three chambers, scala vestibuli (vestibular duct), scala media (cochlear duct) and scala tympani (tympanic duct). The Reissner’s membrane and basilar membranes separate the scala media from scala tympani and scala vestibuli. Perilymph and endolymph are the important fluids circulating in the inner ear. Perilymph is an extracellular fluid that circulates within the tympanic duct and vestibular duct and endolymph fluid filled the cochlear duct of the inner ear. The key components of these fluids are sodium and potassium ions, which are necessary for the appropriate sound stimuli transduction in the cochlea (5). Moreover, the lateral wall of the cochlea lining exists with spiral ligament and stria vascularis. The spiral ligament is made up of extracellular connective tissue materials and provides mechanical support for stria vascularis (6). Stria vascularis mainly regulates the endocochlear potential in the scala media and is functionally integrated with spiral ligament to mediate ion homeostasis in the cochlea. A core element of the scala media is the organ of Corti, which contains a series of inner hair cells, three series of outer hair cells and different types of non-sensory supporting cells. Different types of supporting cells (Deiter’s cells, Pillar cells, Hensen’s cells, Claudius cells, and Boettcher cells) present at the base of each hair cell with different morphological features and this presence offers structural and physiological support to the hair cells (6, 7). However, these supporting cells are not contributing in sound transduction, playing an important role in hair cell regeneration through mitotic division or direct transdifferentiation (8). In the cochlea, numerous in vitro studies are being targeted auditory hair cells, ganglion neuronal cells, supporting cells and spiral ligament fibrocytes by different therapeutic approaches including stem cell therapy, gene therapy, siRNA nanoparticles, and miRNA.
Stem Cells. Different types of stem cells (embryonic stem cells, adult stem cells and induced pluripotent stem cells) have been involved in sensory hair cells and auditory neurons regeneration. Embryonic stem cells are pluripotent cells, derived from early embryos, that can differentiate into any embryonic cell type. ESCs were used in numerous studies to regenerate sensory hair-like cells and neuronal cells (9-11). Many countries have raised ethical concerns with the use of ESCs (12). Recently, a novel method has been developed for the first-time differentiation of human ESC, iPSC into otic cell types of the cochlea using three-dimensional organoid culture system (13). Developing a new protocol for the hearing regeneration may provide better knowledge about the inner ear development. However, this method needs to be optimized in a wide range of pluripotent stem cells. Induced pluripotent stem cell (iPSC) is a type of pluripotent stem cell that are artificially made from somatic cells. These stem cells have the self-renewal capacity in vitro, they are able to form three primitive germ layers (ectoderm, mesoderm, and endoderm). Yamanaka and Takahashi first discovered iPSCs by cellular reprogramming method (14). Recently, Boddy et al. has developed non-integrating mRNA reprogramming technology on iPSCs to produce otic cell lineages. This technology facilitates the limitation of genetic variability imposed by other cell reprogramming methods (viral reprogramming and DNA-based reprogramming) and are suggested as a novel tool in the field of regenerative medicine (15). However, tumor formation was observed after transplantation of iPSCs into the mouse cochlea, and this might be caused by the undifferentiated iPSCs (16).
Mesenchymal Stem Cells. Mesenchymal stem cells are adult stromal cells, characterized by non-hematopoietic, self-renewing, multipotent, highly proliferative, adherent growing nature, paracrine activity and migration ability to the injury sites. The presence of MSCs in tissues is identified by the expression of surface antigens CD105, CD90 and CD73 (17). Bone marrow, umbilical cord, adipose tissue and placenta are rich sources of MSCs and used in variety of tissue regeneration studies (18). The risk of isolation of MSCs depends on different sources. For example, MSCs isolation from cord tissue and placenta is ethically unproblematic and non-invasive than other sources. Originally, MSCs were differentiated into bone cells, fat cells and cartilage cells. But recent studies have shown that MSCs can induce to differentiate auditory hair cells, neuronal cells and cochlear fibrocytes, which made a key milestone in hearing regeneration (19-21) (Tables I and II).
In vitro studies of mesenchymal stem cells (MSCs) in hearing regeneration.
Studies of mesenchymal stem cells (MSCs) in animal models for hearing regeneration.
Mesenchymal Stem Cells in Inner Hair Cell Regeneration. In the cochlea, regeneration of auditory neurons and hair cells through the application of MSCs is not a simple process. It requires certain neurotrophic factors especially glial cell-derived neurotrophic factor, brain-derived neurotrophic factor and neurotrophin-3 (GDNF, BDNF, NT-3) and growth factors for the differentiation of MSCs into auditory hair-like and neuronal cells (22-24). Evidence showed that mesenchymal stem cells could be able to differentiate auditory hair-like cells that were confirmed by the expression of hair cell markers Atoh1, Sox2, Jagged2, p27kip, Brn3c, Myosin VIIA and, Espin which are essential for inner ear development and hearing function (20). Administration of MSCs can cause diverse beneficial effects in in vivo models. In noise or drug-induced hearing loss model, the systemic administration of MSCs induces abundant neurotrophin expression in the cochlear injured sites, thereby promote the regeneration of auditory hair cells and neurons (25). In Sensorineural hearing loss patients, transplantation of autologous BM-MSCs showed no significant improvement in their hearing but no other complications and side-effects were found in their three year follow-up (26). However, when considering clinical trial aspects, therapeutic feasibility and safety measures must be assured. This study may give additional evidence for MSCs as the safest method in hearing loss. MSCs are considered as potent immunomodulators in various autoimmune inner ear diseases (27). In an autoimmune hearing loss murine model, human adipose-derived mesenchymal stem cells (h-ADSCs), h-ADSCs down-regulate Th1-mediated autoreactive response that recruits antigen-specific Treg cells to secrete interleukin-10 and suppresses the self-reactive T-cells and protects cochlear hair cell loss from degeneration (28). Some studies showed that MSCs have a greater migration effect to the injured sites of the cochlea. The delivery of umbilical cord-MSCs to the cerebrospinal fluid of congenital deaf albino pigs, facilitated enhanced migration of MSCs to different regions of inner ear cochlea, central nervous system and peripheral organs and also clinical adverse effects were not observed until eight weeks of transplantation (29). Another study by M.Y. Choi et al. reported that administration of UC blood-derived MSCs into the brachial vein of sensorineural hearing loss guinea pigs could enhance the number of missing or damaged neural cells in the spiral ganglion, replace damaged cochlear outer hair cells and significantly improve the auditory brainstem responses (ABRs) (30).
Mesenchymal Stem Cells in Spiral Ganglion Neurons (SGNs) Regeneration. In the central axis of the cochlea (modiolus), a group of neuron cell bodies are present, and are called spiral ganglion neurons (SGNs). They transmit the sound signals from the organ of Corti to auditory brainstem and stimulate the production of nerve impulses in the brain. In the auditory neuronal portion, two types (type I and type II) of ganglion cells are classified by their morphological structure, cell body, myelin sheath and biological function. Type I spiral ganglion cells are myelinated, large, bipolar cells and occupy 95% of the cochlear nerve cells and primarily innervate the inner ear hair cells, whereas the remaining nerve cells are composed of small, unmyelinated type II ganglion cells and innervate the outer hair cells (31). These ganglion cells perform different functions in auditory processing along with the sensory hair cells and the presence of a number of ganglion neuronal cells may vary among different species (32). Moreover, SGNs do not have the capacity of postembryonic cellular division, and cannot produce new sensory neurons when damage occurs (33). Generally, inner ear neuronal cells are regulated by predominant neurotrophic factors such as brain-derived neurotrophic factor (BDNF), neurotrophin-3 (NT-3) and glial cell-derived neurotrophic factor (GDNF) (34). BDNF is one of the most abundant neurotrophins, present in the brain that facilitates neuronal growth and controls the production, absorption and elimination of neurotransmitters. NT-3 is another neurotrophin that provides support for the neuronal growth and differentiation (35). GDNF is involved in promoting cochlear neuronal cell survival. These neurotrophins are supplied either as a neuronal medium for the complete differentiation of BM-MSCs to neuronal cells in vitro (36) or as genetically modified MSCs in the deafness animal model (37). A recent study established that genetically modified BDNF-producing MSCs in alginate-coated matrix protect the survival of SGNs from degeneration. In the drug delivery system, this encapsulation technique provides a good support for the survival of MSCs and their migratory control (38). Moreover, the higher proliferative potential of MSCs from Wharton’s jelly was able to differentiate auditory neuronal cells in a culture medium containing neurotrophic factors GDNF, BDNF and NT-3 (39).
Mesenchymal Stem Cells in Spiral Ligament Fibrocytes (SLFs) Repair. In mammals, cochlear fibrocytes arise from non-sensory regions, contribute to normal hearing function and play a potential role in transporting potassium ions to generate endolymphatic potential in the scala media. These fibrocytes are majorly found in the lateral wall of the cochlear spiral ligament and stria vascularis. Fibrocytes expressing various proteins for homeostasis mechanism, ionic transportation, collagen metabolism, potassium recycling, and gap junction communication of inner ear cell types (40). Compared to other sensory cells, spiral ligament fibrocytes are able to renew themselves in the mammalian inner ear after drug exposure (41). Within the cochlear lateral wall, mature fibrocytes are classified into five types I-V based on the structural characteristics, location and immunostaining patterns (40, 42). Fibrocytes originated from mesodermal germ layer that form part of connective tissue. These cells are able to proliferate throughout the human lifespan. However, less proliferation was detected in the lateral wall of adult cochlea (43). SLFs degeneration or dysfunction may arise from excessive noise, aging or genetic mutations. Sun et al. investigated two mechanisms for the functional communication between MSCs and SLFs. The first is that transplanted MSCs in the inner ear could transdifferentiate into SLF-like cells which compensate for the missing SLFs. The other is that transplanted MSCs boost the proliferation and regeneration of damaged SLFs (44). In the sensory hearing loss model, the functional recovery of hearing achieved by transplantation of MSCs that could repair injured SLFs and damaged gap junction network through invasion, migration, and proliferation of MSCs in the lateral wall of the cochlea (45). In young mice cochlea, transplanted MSCs were able to migrate and differentiate into fibrocyte-like cells with no adverse effects on hearing function. In contrast, there were no migration or differentiation of MSCs observed after transplantation in adult mice. This study may suggest that MSCs transplantation could be a better treatment to delay or stop early progression of sensorineural hearing loss (46).
MSCs and Gene Therapy in Hearing Regeneration. Gene therapy is a modern treatment approach that is being used to deliver genes of interests for reversing or preventing disease conditions. Most gene therapeutic approaches rely on the viral vectors such as adeno-associated virus (AAV), adenovirus (AV), lentivirus (LV) and herpes virus (HV). These viral vectors are not pathogenic to the host cells, they do not have viral genes, they have high transduction efficiency and non-toxic to the host cells (47). One of the major challenges of gene therapy is achieving local delivery of viral vectors without any damage to sensitive inner ear structures (48). There are many genes, ATOH1, SOX2, OCT4, Myosin7A, GJB2 (connexin 26), Espin, and USH1C necessary for cochlear hair cells and supporting cell development. ATOH1 (also known as Math1) gene encoding the basic helix-loop-helix transcription factor that is vital for inner ear hair cell differentiation (49). In a hearing loss animal model, adenoviral-mediated ATOH1 gene therapy effectively improved the regeneration of auditory hair cells (50). Another study evidenced that, adeno-associated virus (AAV)-mediated ATOH1 gene delivery could transfect supporting cells to induce the formation of new hair cells (51). In the last few years, MSCs are used as a therapeutic vehicle for gene therapy methods in various diseases. Different approaches (viral vector-based gene delivery, non-viral gene delivery) have been employed to introduce regenerative genes into MSCs. The advantage of MSCs in gene therapy is that they can be modified with a broad range of viral and non-viral vector systems. However, the transduction efficiency may differ with each vector (52). Genetically modified MSCs can be used to treat heart diseases, bone diseases, cancer, central nervous system diseases and autoimmune diseases (53). In hearing research, Devarajan et al. reported the delivery of the ATOH1 gene through adenovector mediated transduction into human umbilical cord mesenchymal stem cells induced to differentiate inner ear hair cells phenotype in vitro. These differentiated hair cells were confirmed by the expression of hair cell markers (54). This study provided a new foundation for hearing loss treatment. But there exists no further clinical evidence found for the combination of gene and stem cell-based therapies in hearing loss studies.
MSCs and siRNA in Hearing Regeneration. Small interfering RNAs (siRNAs) are short, non-coding double-stranded RNA molecules, specifically targeting disease-causing genes and silencing them. In an siRNA transfection study, different viral vectors, nucleic acid constructs, polyethylenimine vectors, recombinant proteins, nanoparticles, cationic liposomes have been used as delivery vehicles (55). In the inner ear, Notch signaling pathway is the main target for regeneration of hair cells. Modulation of notch downstream molecule Hes1 with siRNA is enough for the ATOH1 gene up-regulation and promotes an increase in hair cell number. Significant recovery of hearing function attained by delivery of siHes1 encapsulated nanoparticles in a hearing loss animal model (56). To enhance the therapeutic applicability of siRNA in ototoxicity, siMAPK1 nanoparticle treatment was used to reduce the systemic administration of cisplatin-ototoxic effects in hair cell lines (57). However, delivery efficiency, inflammatory reaction and, target gene selection limit the success of siRNA molecules (47). For the first time, Mellott et al. assessed the functional role of ATOH1 gene homologues (HATH1 and MATH1) in human Wharton’s jelly-derived stem cells by the non-viral reprogramming approach. The study hypothesized that, both the ATOH1 gene homologues were not functionally similar in human tissues and the knockdown of Hes1 and Hes5 (negative regulators of inner ear hair cell differentiation) in conjunction with ATOH1 homologues overexpression increases the atonal function could induce the hair cell development (58). However, further clinical evidence is required to show the therapeutic effect of MSCs with siRNA in hearing regeneration.
MSCs and miRNA in Hearing Regeneration. MicroRNAs (miRNAs) are small, non-coding RNA molecules, highly conserved in many species, that regulate physiological, biological and pathological processes in inner ear development (59). Apart from other essential genes, these small molecules also participate in hearing regeneration. In SNHL, some of these miRNAs are identified as biomarkers for diagnosing age-related and noise-induced hearing loss. Several miRNAs play a major role in the inner ear, and their targets play a role in hearing regulation (60). Wang et al. performed a study on mouse otocyst-derived cells, where mir-182 promoted the differentiation of otocyst cell fate into hair-like cells and as the transcription factor Tbx1 was functionally influenced by miR-182, and was found to be the target of miRNA-182, thereby providing a crucial gene in development of the inner ear (61). MiR-183 family has three homologues (miR-183, miR-182 and miR-96) that are abundantly expressed in vertebrates of auditory hair cells and sensory neurons (62). Activation of this microRNA family homologues is essential for the development of inner ear stereociliary hair bundle formation and cochlear hair cell function (63). Transdifferentiation is a cellular process of conversion of one cell type into another type without self-renewal of the original cell. In the organ of Corti, miRNA-210 promote the transdifferentiation of epithelial cells to sensory hair cells (64). Apart from that, a transfection agent was used to study the expression of hair cell-specific markers in mesenchymal stem cells. This study established that, transfection of microRNA (mir-182, mir-183 and mir-96) mimics into human BM-MSCs facilitated hair cell markers up-regulation. Among three microRNAs, miR-182 could enhance the differentiation of MSCs, therefore microRNA function could serve a precise role in hair cell differentiation (65).
Clinical Challenges of MSCs Administration in the Cochlea. Stem cell administration to the inner ear cochlea is not a simple procedure. It is associated with various risks and challenges. Some of the clinical issues, the proper efficient distribution, migration, immunocompatibility and retaining the cells alive at the target sites must be resolved when using MSC therapy. Inside the cochlea, a specific microenvironment is required to facilitate the survival of exogenously transplanted stem cells (66). Stem cells can be delivered through tympanic or vestibular duct, which contain perilymph fluid, but need to cross the membrane barriers (Reissner’s or basilar membranes) to reach the organ of Corti. This will be the biggest challenge for transplanted MSCs. To overcome this, stem cells might be directly delivered to the cochlear duct that could make some beneficial effect. However, the higher concentration of potassium ions in the endolymph can lead to endolymphatic fluid toxicity that will disrupt the function of neighboring hair cells and supporting cells and decrease the viability of transplanted cells. Furosemide injection may be helpful to reduce the endocochlear potential toxicity in scala media (67). Furthermore, transplantation of MSCs into different sites of the cochlea may show better results and also cause damage to the inner ear structure, infection or other complications, further weakening of hearing by affecting organ of Corti cells. Intravenous or local administration requires more volume of MSCs and rarely crosses the blood brain barrier, therefore causing a reduction in the cell migration to the target sites (26). For example, Choi et al. demonstrated that intravenously injected MSCs to noise or drug-induced hearing loss rats were greatly trapped in the lungs than other injured sites (25). Overall, various physiological and cytotoxic barriers in the mammalian inner ear cochlea may have a significant impact on the transplanted stem cell distribution, migration and survival.
Conclusion
Different approaches (stem cell therapy, gene therapy, small interference RNA and microRNA) are being developed for the treatment of hearing loss. Among them, mesenchymal stem cell therapy provides a new hope for otolaryngologists. The reason is mesenchymal stem cells own significant properties such as self-renewal, multipotency, higher proliferation potential, migration, and paracrine activity. The MSCs isolation procedure may vary by sources (bone marrow, adipose tissue, umbilical cord and placenta), but the functional features are almost similar. For example, the isolation of MSCs from bone marrow is an invasive and painful procedure compared to using the umbilical cord. But both MSCs can exhibit similar morphology, surface marker expression, colony formation, doubling time, migration, differentiation potential and immunomodulation. Though many experimental studies show possible outcome of MSC-based therapy in regenerative medicine, some of the challenges are encountered by it. The main challenge is to achieve successful delivery of MSCs to the target sites. Sometimes, transplanted MSCs may cause incompatibility, inflammation and tumor formation to the experimental animals. Besides, a suitable microenvironment is necessary for the MSCs survival and migration. Still, many in vitro studies provide deep insight for the therapeutic application of MSCs. Continuous research in this area is required to establish the complete mesenchymal stem cell approach in pre-clinical and clinical evaluation.
Acknowledgements
This work was supported by grants from the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (NRF-2018-R1D-1A1B07048074) and National Research Foundation of Korea (NRF) funded by the Ministry of Science and ICT for Bioinspired Innovation Technology Development Project (NRF-2018M3C1B7021997).
Footnotes
Authors’ Contributions
Maharajan N and Cho GW wrote the article, Jang CH designed and supervised the study.
Conflicts of Interest
The Authors declare no conflicts of interest with regard to the present study.
This article is freely accessible online.
- Received September 13, 2020.
- Revision received September 27, 2020.
- Accepted September 30, 2020.
- Copyright© 2021, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}