


Abstract
Background: It is unclear whether the de-escalated therapy that omits anthracycline-based chemotherapy is as beneficial as standard therapy for patients with stage I human epidermal growth factor receptor 2-positive (HER2+) early breast cancer. Patients and Methods: We retrospectively investigated 95 patients with pathological stage I HER2+ early breast cancer who underwent adjuvant treatment from April 2009 to December 2018. Results: We assessed 45 patients who underwent standard therapy containing anthracyclines, 35 patients who underwent paclitaxel plus trastuzumab (P+TRA group), and 15 patients who underwent trastuzumab monotherapy or no adjuvant therapy; the 5-year invasive disease-free survival rates were 97.8%, 92.9%, and 93.3%, respectively (p=0.255). Adverse events were significantly less frequent in the P+TRA group than that in the standard therapy group. Conclusion: In a real-world setting, de-escalated therapy without anthracyclines demonstrated excellent outcomes similar to the standard therapy containing anthracyclines as well as lower adverse events.
- Early breast cancer
- HER2-positive
- invasive disease-free survival
- de-escalated therapy
- real-world experience
Approximately 20% of patients with early breast cancer (EBC) have human epidermal growth factor receptor 2 (HER2) overexpression (1). Trastuzumab combined with chemotherapy for patients with HER2+ EBC reduces the risk of recurrence and mortality compared with chemotherapy alone, and the addition of trastuzumab to adjuvant chemotherapy is a standard therapy for these patients (1-6). Trastuzumab has been approved in the European Society for Medical Oncology guidelines for node-positive disease, node-negative disease with tumors larger than 1 cm, and node-negative disease with tumors smaller than 1 cm tumor but with a somewhat higher relapse risk (7). Given that most patients with stage I HER2+ EBC were ineligible for the adjuvant trastuzumab trials documented in the guidelines (1-5), the standard adjuvant therapy for these patients is unclear. The Adjuvant Paclitaxel and Trastuzumab (APT) trial recently showed that adjuvant paclitaxel and trastuzumab (P+TRA) was a therapeutic option for stage I HER2+ EBC and mentioned that P+TRA represents an important step toward de-escalated chemotherapy (8, 9). Given that the APT trial had no control arm, the exact efficacy of P+TRA compared with standard therapy including anthracycline-based regimens is unknown. We therefore retrospectively investigated the efficacy of P+TRA as de-escalated therapy omitting anthracyclines compared with standard therapy in a real-world setting.
Patients and Methods
Patients. We retrospectively reviewed the data for patients with stage I HER2+ EBC who underwent adjuvant therapy at Fukuyama City Hospital (Japan) from April 2009 to December 2018. We obtained the patients' medical data from the original hospital records and investigated the patients' characteristics and outcomes. The hormone receptor and HER2 status were defined according to the American Society of Clinical Oncology/College of American Pathologists guidelines (10, 11). Assessing the pathological reports of surgical specimens, ‘hormone receptor-positive’ defined those with estrogen receptor-positive and/or progesterone receptor-positive, and ‘HER2+’ was defined as a score of 3 in the immunohistochemistry or the presence of HER2 gene amplification by fluorescence in situ hybridization. The physicians decided the adjuvant chemotherapy regimens, including dose modifications, interruptions, and discontinuations, and the patients were divided into three groups according to adjuvant chemotherapy regimen. The standard therapy group (standard group) underwent anthracycline-based regimens (epirubicin/cyclophosphamide or fluorouracil/epirubicin/cyclophosphamide) and P+TRA (including three cases without paclitaxel and one case without trastuzumab). The de-escalated therapy groups underwent P+TRA, or trastuzumab monotherapy or no adjuvant therapy (Other group). Lastly, we identified 95 patients with pathological stage I HER2+ EBC who underwent treatment, and we investigated the invasive disease-free survival (IDFS) of these three groups. This retrospective study was approved by Fukuyama City Hospital's review board (approval number: 524). All procedures that involved human participants were performed in accordance with the ethical standards of the institutional and national research committees and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants in the form of an opt-out on the website included for the study. We assessed adverse events according to Common Terminology Criteria for Adverse Events v5.0 (12).
Patient characteristics at the time of adjuvant treatment.
Statistical analysis. We employed the Kruskal–Wallis test to compare median ages and chi-square test or Fisher's exact test to compare the proportions of characteristics between the groups. Survival analyses were estimated using the Kaplan–Meier method, and differences between the groups were calculated using the log-rank test. A value of p<0.05 was considered statistically significant. All statistical analyses were performed with EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria) (13).
We defined IDFS as the time from the diagnosis to the first event, according to the standardized definitions for efficacy endpoints (STEEP) system (14): Following ipsilateral invasive breast tumor recurrence, regional invasive breast cancer recurrence, distant recurrence, death from any cause, contralateral invasive breast cancer, and second primary non-breast invasive cancer. Overall survival (OS) was defined as the time from diagnosis to death from any cause.
Results
Patient characteristics. We identified 95 patients with HER2+ EBC at our institution, with 45 patients assigned to the standard therapy group, 35 to the P+TRA group, and 15 to the Other group. Table I shows the patients' baseline characteristics. Overall, the median age was 61 years (range=29-90 years), and 58 patients (61.1%) had a T1c tumor, whilst 53 (55.8%) had hormone receptor-positive disease. The median follow-up duration was 61.7 (range=18.9-123.4) months; 82.4 (range=33.9-123.4) months in the standard therapy group, 38.8 (range=18.9-91.0) months in the P+TRA group and 70.4 (range=19.9-119.9) months in the Other group.
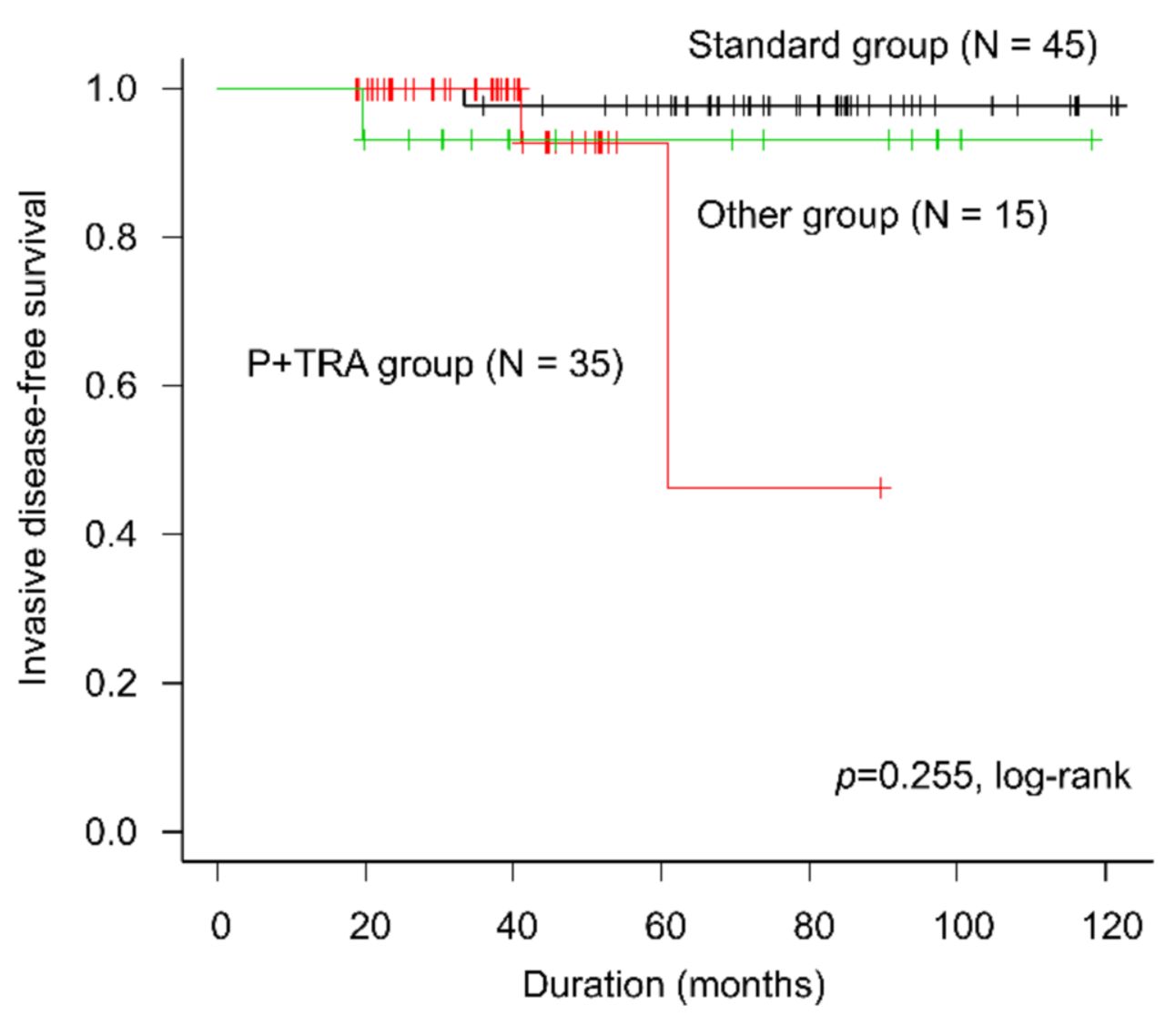
Efficacy. There were four IDFS events in total: one was a distant recurrence (1.1%), and three were deaths without breast cancer recurrence (3.2%). The 5-year IDFS was 97.8% [95% confidence interval (CI)=85.3-99.7%] for the standard group, 92.9% (95% CI=59.1-99.0%) for the P+TRA group, and 93.3% (95% CI=61.3-99.0%) for the Other group (p=0.255) (Figure 1). The 5-year OS was 97.8% (95% CI=85.3-99.7%) for the standard group, 100.0% (95% CI=not reached) for the P+TRA group, and 93.3% (95% CI=61.3-99.0%) for the Other group (p=0.551) (Figure 2).

Invasive disease-free survival according to treatment group. Other group: Trastuzumab monotherapy or no adjuvant therapy; P+TRA group: paclitaxel plus trastuzumab; Standard group: standard therapy including anthracycline-based regimens.
Adverse events. During the adjuvant therapy, there were significantly fewer adverse events (AEs) in the P+TRA group compared with the standard group. Forty-two patients (93.3%) in the standard group and 14 patients (40.0%) in the P+TRA group experienced grade 3 or 4 neutropenia (p<0.001), and 33 patients (73.3%) in the standard group and 14 patients (40.0%) in the P+TRA group experienced nausea or vomiting (p=0.003). Seven patients (15.6%) in the standard group and none of the patients in the P+TRA group experienced grade 3 left ventricular systolic dysfunction (p=0.016). Other AEs are shown in Table II.
Discussion
A number of clinical trials and the Cochrane library review demonstrated that the addition of trastuzumab to adjuvant chemotherapy including anthracyclines and taxanes significantly reduced recurrence and mortality (1-6). A meta-analysis that included randomized trastuzumab trials showed that patients with HER2+ tumors measuring 2 cm or smaller derived substantial disease-free survival (DFS) and OS benefit from the addition of trastuzumab to adjuvant chemotherapy (15). A review that included randomized trastuzumab trials showed that patients with small HER2+ tumors also derived a similar benefit in terms of DFS from the addition of trastuzumab to chemotherapy when compared with the overall study (16). Furthermore, retrospective studies have shown a recurrence rate of 5-30% for patients with small node-negative HER2+ EBC and have suggested that these patients might derive a clinically relevant benefit from adjuvant trastuzumab-based therapy (7, 16, 17). However, trastuzumab significantly increases the risk of congestive heart failure (risk ratio= 5.11, 90% CI=3.00-8.72; p<0.00001), and decreased left ventricular ejection fraction (risk ratio=1.83, 90% CI=1.36-2.47; p=0.0008) (6). Physicians therefore need to be vigilant for cardiac toxicity, especially in patients with HER2+ EBC and a low risk of recurrence such as stage I. There is a natural expectation that de-escalated therapy should be prescribed for these patients given the desire to prevent cardiac toxicity. However, the efficacy of de-escalated therapy is unknown because previous clinical trials compared the addition of trastuzumab to adjuvant chemotherapy with adjuvant chemotherapy alone. The APT trial recently demonstrated that the combination of paclitaxel and trastuzumab provided excellent outcomes for patients with small HER2+ EBC, with a 3-year DFS of 98.5%, a 5-year DFS of 96.3% and a 7-year DFS of 93.3% (8, 9). However, the APT trial did not have a control arm because no standard of treatment existed at that time for this population. In addition, because of the low incidence of DFS events, it is difficult to conduct a randomized trial. Therefore, we investigated the efficacy of P+TRA compared with standard therapy containing anthracyclines in a real-world setting. Although there were very few IDFS events of distant recurrence (1.1%), our study demonstrated excellent outcomes of P+TRA compared with those of standard anthracycline-containing therapy, and the results were similar to those of the APT trial (9). There are no results from clinical trials or real-world data comparing the efficacy of adjuvant standard therapy containing anthracycline with those omitting anthracyclines for patients with stage I HER2+ EBC. Our results suggested that de-escalated therapy omitting anthracyclines for HER2+ EBC is one of standard regimens not only for patients in Western country but also for Japanese patients.

Overall survival according to treatment group. Other group: Trastuzumab monotherapy or no adjuvant therapy; P+TRA group: paclitaxel plus trastuzumab; Standard group: standard therapy including anthracycline-based regimens.
Adverse events according to treatment.
The frequency of AEs in the P+TRA group was lower than that of the standard group, and the trend was similar to the results of the APT trial. Therefore, considering the balance between efficacy and AEs, P+TRA might be preferable to standard therapy including anthracyclines for patients with stage I HER2+ EBC.
A number of prospective studies have reported the less toxic therapy for patients with HER2+ EBC and small node-negative tumors. The ATEMPT trial was an investigator-initiated, randomized, multicenter, phase II adjuvant study that compared P+TRA with trastuzumab emtansine. The regimen was associated with very few recurrences, and trastuzumab emtansine was associated with significantly lower toxicity than P+TRA (18). The RESPECT trial investigated the benefit of trastuzumab monotherapy compared with the combination of trastuzumab and chemotherapy in women over 70 years of age with HER2+ EBC in Japan. The trial suggested that trastuzumab monotherapy might be an option as an adjuvant therapy for elderly patients with HER2+ EBC. Our results for the group treated with trastuzumab monotherapy or no adjuvant therapy showed good outcomes, similar to standard therapy containing anthracyclines, and the results support the results of the RESPECT trial (19, 20).
Our study has a number of limitations due to its retrospective nature and being a single-institution study. However, since this was a single-institution study, patients were carefully followed-up and only two (2.1%) were untraceable. In addition, our study allowed us to compare P+TRA therapy omitting anthracyclines with standard anthracycline-containing therapy. As far as we are aware, our report is the first to compare these two groups and to mention the management of HER2+ EBC. We must point out the difference in the follow-up periods between the groups because we had selected the P+TRA regimen in daily practice after the APT study result was published (8). Although our study's observation period was similar to that reported by many investigators, very few IDFS events occurred, suggesting that the risk of recurrence might be reduced by the de-escalated therapy omitting anthracyclines, which might be an appropriate treatment.
The de-escalated therapy omitting anthracyclines demonstrated excellent outcomes similar to the standard therapy containing anthracyclines in a real-world setting. Cardiac events were significantly less frequent in the P+TRA group. Considering the balance between efficacy and AEs, the de-escalated therapy omitting anthracyclines might be a therapeutic option for stage I HER2+ EBC.
Acknowledgements
The Authors would like to thank Enago (www.enago.jp) for English language review.
Footnotes
Authors' Contributions
All Authors contributed to the study conception and design. Shogo Nakamoto prepared the materials and performed the data collection and analysis. Shogo Nakamoto wrote the first draft of the article, and all Authors commented on the previous versions of the article. All Authors read and approved the final article.
This article is freely accessible online.
Conflicts of Interest
Dr. Nakamoto reports having received personal fees from Chugai Pharmaceuticals, Eisai, and Taiho Pharmaceuticals outside the submitted work; Dr. Ikeda reports having received personal fees from AstraZeneca, Chugai Pharmaceuticals, Daiichi-Sankyo, Eisai, Eli-Lilly, Kyowa Kirin, Pfizer, Nippon Kayaku, Novartis, Mundipharma, Celltrion Healthcare, and Sawai Pharmaceuticals outside the submitted work; Dr. Kubo reports having received personal fees from Eli-Lilly outside the submitted work; Dr. Yamamoto reports having received personal fees from Bayer outside the submitted work. The other authors have no conflicts of interest.
- Received September 25, 2020.
- Revision received October 5, 2020.
- Accepted October 6, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.