


Abstract
Background/Aim: The impact of diverting ileostomy on the feasibility of adjuvant chemotherapy (ACT) remains unclear. We retrospectively investigated the tolerability and adverse events of ACT for rectal cancer in patients with diverting ileostomy. Patients and Methods: Thirty-three patients who received ACT after curative resection with ileostomy construction for rectal cancer were analyzed. We assessed completion rate, the mean relative dose intensities, and the factors affecting the tolerability of ACT. Results: The completion rate of each chemotherapy regimen was 10 out of 16 patients in oral uracil-tegafur plus leucovorin (UFT/LV), 1 out of 3 patients in oral capecitabine (Capecitabine) and 2 out of 14 patients in capecitabine plus oxaliplatin (CAPOX). The mean relative dose intensities were 77% in UFT/LV, 48% in Capecitabine, and 57% of capecitabine and 42% of oxaliplatin in CAPOX. In multivariate analysis, laparoscopic surgery (Odds ratio=11.6, p=0.021) and receiving preoperative chemoradiotherapy (Odds ratio=32.4, p=0.021) were associated with treatment completion. Conclusion: Completion rate of ACT in patients with diverting ileostomy was lower than that of colorectal cancer patients in the previous studies. UFT/LV may be a more tolerable regimen than Capecitabine or CAPOX in colorectal cancer patients with diverting ileostomy.
Anastomotic leakage is one of the severe complications of the surgical treatment for rectal cancer, causing morbidity and mortality. Diverting ileostomy is constructed in lower rectal surgery with high risk of anastomotic leakage. Previous reports have demonstrated that constructing a diverting stoma reduces clinically relevant anastomotic leakage (1-3).
Several studies have proven that adjuvant chemotherapy (ACT) improves postoperative survival in patients with stage III colorectal cancer (4-6). In case of advanced lower rectal cancer, ACT is indicated in patients with ileostomy. However, there is scarce data regarding the tolerability of ACT for rectal cancer in patients with diverting ileostomy.
This retrospective cohort study aimed to investigate the tolerability and adverse events of ACT for rectal cancer in patients with diverting ileostomy.
Patients and Methods
Patients. Between April 2011 and March 2018, 33 patients with rectal cancer received ACT after curative resection with ileostomy construction in a single center, Saitama Medical center, Jichi Medical University. We retrospectively reviewed the medical charts of these patients.
ACT is indicated in patients with histologically confirmed stage III (any T, N1–3, M0; according to UICC TNM classification) (7) or high–risk stage II (T4, inadequately sampled lymph node, poorly differentiated tumor, lymphovascular invasion) rectal cancer (8). In the present study, patients who received preoperative chemoradiotherapy were also included.
Bioethics Committee for Clinical Research, Saitama Medical Center, Jichi Medical University approved this study (#S19-164).
Regimens. Chemotherapy regimens were oral uracil-tegafur plus leucovorin (UFT/LV), oral capecitabine (Capecitabine) or capecitabine plus oxaliplatin (CAPOX). Treatment regimen was determined by the attending physicians. CAPOX regimen was initially recommended, and other regimens were alternatively chosen in consideration with comorbidities, performance status and preferences of the patients.
UFT/LV regimen comprised oral uracil-tegafur 300 mg/m2 daily plus leucovorin 75 mg daily on days 1-28 of a 5-week cycle for a total of five cycles. Capecitabine regimen comprised oral capecitabine 2,500 mg/m2 daily on days 1-14 of a 3-week cycle for a total of eight cycles. CAPOX regimen comprised oral capecitabine 2,000 mg/m2 daily on days 1-14 plus intravenous oxaliplatin 130 mg/m2 on day 1 of a 3-week cycle for a total of eight cycles.
Dose adjustment was performed in case of drug toxicity. Adverse events were assessed according to the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE) version 4.0 (9).
Endpoints. The endpoints of this study were the treatment completion rate, the average relative dose intensities, the reasons for the discontinuation of ACT, and the rate of adverse events of each chemotherapy regimen. We also assessed the clinical factors affecting the discontinuation of ACT. The patient characteristics [age, sex, body mass index (BMI), and American Society of Anesthesiologists Physical Status Classification (ASA-PS)], the preoperative chemoradiotherapy, the surgical approach (open, laparoscopic), the postoperative high output stoma, the pathology stage, and the interval from surgery to ACT were retrieved from medical records. The postoperative high output stoma was defined as an output ≥2,000 ml per day or an output ≥1500 ml for two consecutive days (10, 11).
Statistical analysis. The statistical analyses were performed using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for the R software program (The R Foundation for Statistical Computing, Vienna, Austria) (12). Fisher's exact test was used for qualitative data and the Student-t test or the Mann-Whitney U-test was used for quantitative data. A multivariate analysis was performed by logistic regression model. Statistical significance was established at p<0.05.
Results
Patient demographics and clinical characteristics. The characteristics of patients are listed in Table I. The median age of the patients was 64 years (range=34-79). There were 23 men and 10 women. Treatment regimens of ACT were UFT/LV in 16 patients, Capecitabine in 3 patients and CAPOX in 14 patients. Eight patients received preoperative chemoradiotherapy. The surgical approach included open surgery in 18 patients and laparoscopic surgery in 15 patients.
Tolerability and adverse events of ACT (all regimens). The overall completion rate of ACT was 13 out of 33. The percentages of actually received dose (90-100%, 70-90%, 0-70% and 0% of the intended dose) in each cycle of each regimens are shown in Figures 1, 2 and 3. The mean relative dose intensity was the highest in UFT/LV regimen (76.6%) and the lowest in oxaliplatin in CAPOX regimen (42.0%). Grade 3 adverse events occurred in 11 out of 33 patients. The reasons for discontinuation of ACT included adverse events in 16, patient's refusal in 3, and cancer recurrence in 1. The details of tolerability and adverse events of each regimen are described as follows.
Tolerability of UFT/LV. Ten out of 16 patients completed the UFT/LV. The mean of relative dose intensity was 76.6% (Table II). Six patients discontinued the treatment without dose reduction (Figure 1). The reasons for non-completion were related to adverse events in 5 patients and patient refusal in one. A total of 10 patients experienced adverse events of any grade, and 3 patients experienced grade 3 adverse events. The adverse events causing treatment discontinuation were anorexia (4/16) and creatinine increase (1/16) (Table III). Grade 3 adverse events are diarrhea (2/16), dehydration (1/16), creatinine increase (1/16), small intestinal obstruction (1/16) (Table IV).
Clinical and demographic characteristics of patients (n=33).
Tolerability of Capecitabine. One out of 3 patients completed the Capecitabine. The mean of relative dose intensity was 47.6% (Table II). Two patients required dose reduction and 1 could complete the planned treatment (Figure 2). Two patients did not complete the treatment, due to adverse events and patient refusal. A total of 2 patients experienced adverse events of any grade, and 1 patient experienced grade 3 adverse events. The adverse events causing treatment discontinuation were neutropenia (1/3) (Table III). Grade 3 adverse event was hand foot syndrome (1/3) (Table IV).
Tolerability of CAPOX. Two out of 14 patients completed the Capecitabine. The mean relative dose intensity of capecitabine and oxaliplatin were 57.1% and 42.0%, respectively (Table II). Because of the adverse events, 4 patients changed from CAPOX regimen to oral capecitabine alone. The treatment changes were performed from the second cycle in 2 patients, from the fourth cycle in 1 patient, and from the seventh cycle in 1 patient. After changing treatment, 2 patients received a total of seven cycles and 2 patients could complete eight cycles. The reasons for non-completion were related to adverse events in 10 patients, patient refusal in 1, and recurrence of rectal cancer in 1 patient. All patients (n=14) experienced adverse events of any grade, and 3 patients experienced grade 3 adverse events. The adverse events causing treatment discontinuation were stomatitis (3/14), diarrhea (2/14), anorexia (1/14), vomiting (1/14), peripheral neuropathy (1/14), neutropenia (1/14), and allergy (1/14) (Table III). Grade 3 adverse events were anorexia (1/14), vomiting (1/14), diarrhea (1/14), dehydration (1/14), and thrombocytopenia (1/14) (Table IV).
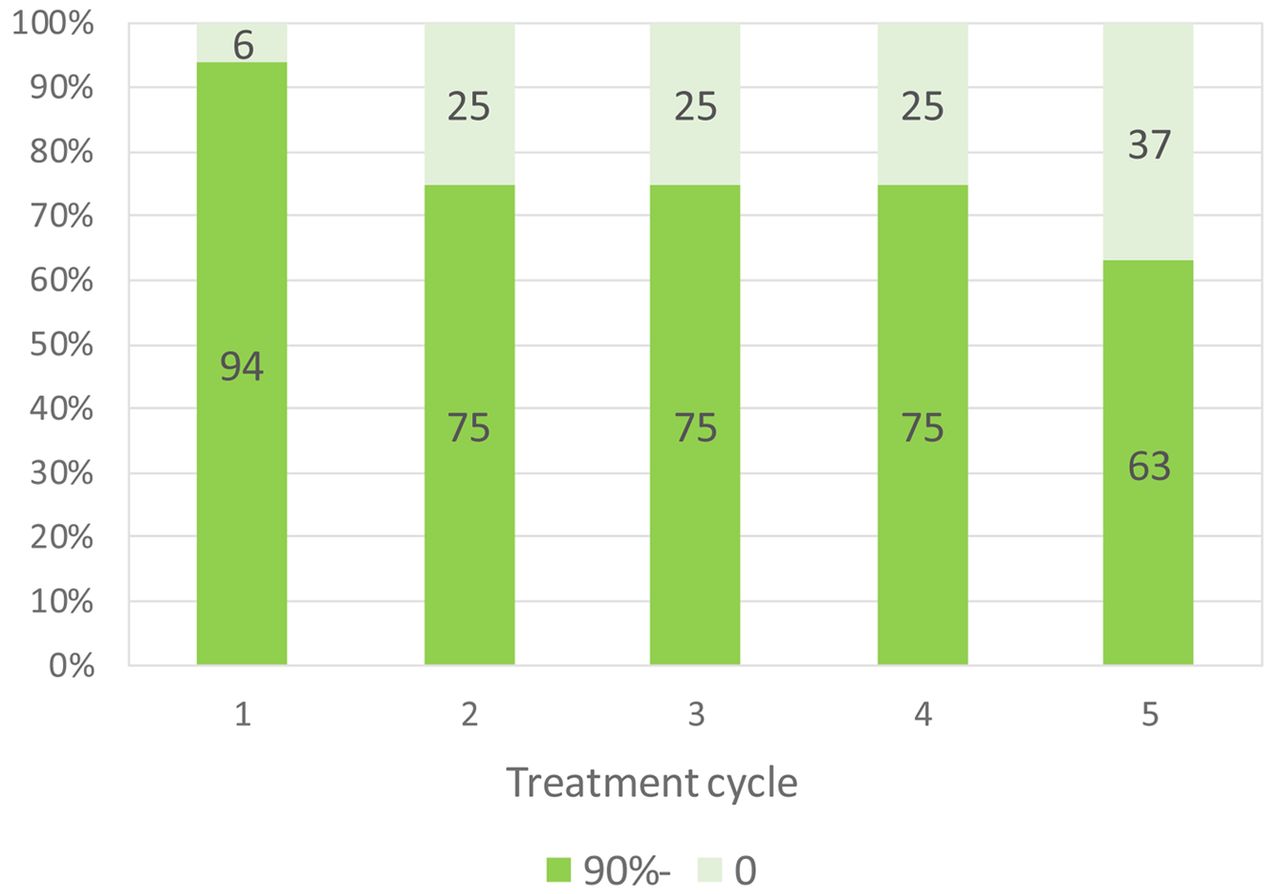
Percentage of received dose of UFT in each cycle of uracil-tegafur plus leucovorin (UFT/LV) regimen.

Percentages of received dose of Capecitabine in each cycle of Capecitabine regimen.
Clinical factors affecting the tolerability of ACT. The clinical characteristics of the treatment completion and non-completion groups are shown in Table V. One patient who discontinued ACT because of recurrence was excluded and a total of 32 patients were analyzed. There were 15 patients in the completion group (including the 2 patients who completed the treatment after changing from CAPOX to Capecitabine) and 17 patients in the non-completion group. Univariate analysis revealed that laparoscopic surgery (p=0.031) and preoperative chemoradiotherapy (p=0.033) were significantly more frequent in the completion group than in the non-completion group. The incidence of postoperative high output stoma was higher in the non-completion group (p=0.041). There were no significant differences in age, gender, regimen, BMI, ASA-PS, pathology stage and interval from operation to start of ACT. Laparoscopic surgery [odds ratio (OR)=11.6; 95% confidence interval (CI)=1.44-92.8; p=0.021 and preoperative chemoradiotherapy (OR=32.4; 95% CI=1.70-619; p=0.021)] were independently associated with the completion of ACT in the multivariate analysis. There was no statistically significant relationship between the incidence of the high output stoma and the preoperative chemoradiotherapy or the surgical approach.

(A) Percentages of received dose of Capecitabine in each cycle of capecitabine plus oxaliplatin (CAPOX) regimen. (B) Percentages of received dose of Oxaliplatin in each cycle of capecitabine plus oxaliplatin (CAPOX) regimen.
Discussion
In this study, we evaluated the tolerability of ACT for rectal cancer in patients with diverting ileostomy. The completion rate of ACT was relatively lower than that reported in the literature for colorectal cancer. In our study, the completion rates of UFT/LV, Capecitabine and CAPOX were 10 out of 16 patients, 1 out of 3 patients and 2 out of 14 patients respectively, although previous studies in Japanese patients with colorectal cancer have reported 73-77%, 66% and 73.7%, respectively (5, 13-15). In addition, previous studies have shown that low completion rate and low relative dose intensity of ACT had negative impact on overall survival rate (16, 17).
Completion rate and relative dose intensity (RDI) of each regimen.
To discuss about the association between lower completion rate of ACT and ileostomy, it is necessary to consider the increased incidence of adverse events in CAPOX regimen (Tables III and IV) and the decreased sustainability in Capecitabine or CAPOX regimens (Figures 2 and 3) when indicating ACT to patients with diverting ileostomy. The completion rate of CAPOX was only 2 out of 14 patients, and 2 patients completed the treatment after switching to Capecitabine alone. A previous study with a larger number of Japanese patients regarding safety and efficacy of CAPOX as adjuvant chemotherapy (MCSCO-1024) reported a completion rate of 73.7%, which included switching to capecitabine alone (13). In that study, reasons for discontinuation of ACT were patient refusal of 16.8%, disease recurrence of 5.8%, and adverse event of 3.7%. On the other hand, most of the reasons for the discontinuation in present study were the adverse events. Similar to the previous study by Danno et al. (13), the most frequent adverse event in our study was peripheral neuropathy. However, the adverse events causing the discontinuation of ACT were gastroenterological events such as stomatitis, diarrhea, anorexia, and vomiting. In our study, discontinuation of ACT was mostly observed within the fourth cycle. These results suggest that adequate monitoring of the gastroenterological symptoms and changing the dose early may contribute to a higher treatment completion rate.
Reasons for discontinuation of each regimen.
In the present study, the UFT/LV regimen showed a trend for higher tolerability than Capecitabine or CAPOX. Although the difference in completion rate of each ACT regimen did not reach statistical significance in present study, this result must be carefully interpreted considering the small number of studied patients and the decision bias in the selection of ACT. The completion rate for UFT/LV (10/16) was lower than in the ACTS-CC trial (73.4%), but the mean relative dose intensity of UFT/LV in our study (76.6%) was similar to the one reported in the ACTS-CC trial (76.5%) (15). The overall incidences of any grade and grade 3 adverse events were 63.5% and 18.8% respectively, in this study, while the ACTS-CC trial reported 73.7% and 14.4% (15). These results suggest that the feasibility of ACT with UFT/LV in patients with ileostomy is acceptable.
The analysis of clinical factors affecting the tolerability of ACT showed that patients with laparoscopic surgery and preoperative chemoradiotherapy were significantly more frequent in the completion than in the non-completion group. Increased tolerability of ACT after laparoscopic surgery might be associated with better postoperative recovery after minimal invasive surgery. Previous studies have demonstrated that laparoscopic colectomy improved short-term surgical outcome (18, 19). Kim et al. have shown that laparoscopic colectomy contributed to greater compliance and earlier initiation of ACT (20).
There is scarce data regarding the relationship between preoperative chemoradiotherapy and tolerability of ACT. In present study, the patients receiving preoperative chemoradiotherapy had already been exposed to chemotherapy before ACT. Therefore, this experience may contribute to improved management for adverse events and dose reduction compared to those without preoperative chemoradiotherapy. Postoperative high output stoma was associated with non-completion, although stoma output and dehydration were well controlled by medication before ACT started. Three patients who suffered from chemotherapy-induced diarrhea also experienced postoperative high output stoma before ACT. The incidence of postoperative high output stoma may be indicator of high risk for adverse events.
Adverse events for each regimen.
Analysis of clinical factors completion group versus non-completion group.
Ileostomy occasionally causes dehydration and acute kidney disease due to the high output stoma and some patients need readmission because of stoma associated complications (21, 22). Robertson et al. (23) reported that the ileostomy was associated with severe chemotherapy-induced diarrhea and that it required chemotherapy regimen changes. In our study, 4 out of 33 patients experienced chemotherapy-induced diarrhea, and in 3 of the 4 it was of grade 3. One patient experienced grade 3 acute kidney disease and needed rehospitalization. The incidence of the chemotherapy-induced diarrhea was not higher than in previous studies, whereas the percentage of grade 3 was higher (13, 15, 23). These results indicated that once diarrhea is induced by ACT, presence of ileostomy might be a prognostic factor for severe adverse events.
Certain reports have addressed the timing of stoma closure in the context of ACT, but the appropriate timing of ileostomy closure is still controversial. Hajibandeh et al. (24), in a meta-analysis regarding ileostomy closure during versus after ACT, showed that there was no significant difference in surgical complication and length of postoperative hospital stay after stoma closure. Zhen et al. (25) demonstrated that patients who underwent stoma closure 6 months after surgery received more cycles of ACT than patients who underwent stoma closure 3 months after surgery. Brown et al. (26) reported that overall survival was similar in patients who underwent ileostomy closure before and after ACT for rectal cancer. There is no report about the relationship between the completion rate of ACT and the diverting ileostomy. Currently, a randomized clinical trial (27) studying the completion of ACT early versus late stoma closure (CoCStom trial) is ongoing.
Our study has potential limitations. It is a retrospective study, with a small sample size. Another limitation is that dose reduction criteria and discontinuation criteria were not strictly defined and were determined by the attending physicians. In this study, we focused specifically on tolerability and adverse event of ACT in patients with ileostomy. We will continue to follow up our patients, and investigate relationship between lower completion rate of ACT, interval from resection of cancer to stoma closure and long-term survival in our future research.
In conclusion, the completion rate of ACT in patients with diverting ileostomy was lower than that of colorectal cancer patients in the previous studies. UFT/LV was reasonably tolerated, while Capecitabine or CAPOX were difficult to continue due to adverse events. Dose reduction or modification of regimens may be considered for sustainable ACT. Larger randomized control studies are warranted to evaluate the tolerability of ACT regimens in patients with diverting ileostomy, to identify the optimal regimen.
Acknowledgements
The Authors would like to thank Editage (www.editage.com) for English language editing.
Footnotes
Authors' Contributions
JT and ST proposed study conception and design. RM, RF, RS and EM performed data collection and acquisition. JT and ST interpreted the data. JT drafted the manuscript. ST, RM, RF, RS and EM edited the manuscript. YM, KS and TR had a role in critical revision of the manuscript. All Authors have read and approved the final version of the manuscript.
This article is freely accessible online.
Conflicts of Interest
The Authors declare no conflicts of interest for this article.
- Received June 8, 2020.
- Revision received July 25, 2020.
- Accepted July 31, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.