


Abstract
Background/Aim: Prophylactic splenectomy has shown no inferiority for tumors not invading the greater curvature side. Despite this, the clinical impact of prophylactic splenectomy for proximal advanced gastric cancer is not clear. This review aimed to clarify the impact of splenectomy for advanced gastric cancer in the upper third of the stomach. Materials and Methods: A systematic review and meta-analysis were conducted based on PubMed and EMBASE databases. The following search terms were used: “gastric cancer” OR “splenectomy” OR upper third of the stomach” OR preservation of the spleen. Results: Out of 765 articles, 18 studies (combined n=6,341) were included in the analysis. Four randomized controlled trials (RCT) and eight retrospective studies suggested the benefits of spleen-preserving gastrectomy. Six retrospective studies showed no significant benefit of spleen-preserving gastrectomy. Prophylactic splenectomy showed a close association with a higher incidence of postoperative morbidity (pancreatic fistula and anastomotic leakage) with no concomitant improvement in overall survival. Prophylactic splenectomy should not be routinely performed and RCTs are necessary to confirm the impact of splenectomy for cN(+) at the splenic hilum tumors and tumors invading the greater curvature.
Despite the recent decrease in the incidence of gastric cancer globally, it is still the third leading cause of cancer-associated mortality (1, 2). Recent years have witnessed a gradual increase in the incidence of proximal gastric cancer in Western and Asian countries (3). Total or proximal gastrectomy combined with adequate lymph node dissection is the standard surgical procedure for proximal gastric cancer. The Japanese Gastric Cancer Treatment Guidelines (ver.4) (4) recommend splenectomy to facilitate complete dissection of No.10 lymph node (D2) for patients with advanced gastric cancer in the upper third of the stomach. Therefore, prophylactic splenectomy is routinely performed even for cN0 status at No.10 lymph node in these patients, and pancreaticosplenectomy or splenectomy are employed in patients with advanced proximal gastric cancer with direct invasion of the pancreas or spleen for R0 resection in Japan (5). On the other hand, in Western countries, therapeutic splenectomy has been limitedly performed for clinical lymph node (cN)-positive at No.10 lymph node and for a tumor invading the spleen or the pancreas in patients with advanced gastric cancer (6). Taken together, it appears that there is a vast difference in the therapeutic strategy between Japan and Western countries.
The clinical significance of prophylactic and therapeutic splenectomy for advanced gastric cancer in the upper third of the stomach remains unclear. Previous studies reported a high incidence of postoperative complications closely related with mortality following gastrectomy combined with splenectomy (7). Some studies have reported a high incidence of lymph node metastasis in the splenic hilum and underlined the need for prophylactic splenectomy in patients with tumors involving the upper third of the stomach and the gastroesophageal junction (8). On the contrary, some other studies have reported poor long-term survival of patients with lymph node metastasis in the splenic hilum (9). Therefore, the relative merits of spleen preservation vis-a-vis those of splenectomy need to be carefully evaluated in this population.
A previous study reported the survival benefits of prophylactic splenectomy in a subset of patients with advanced gastric cancer in the upper third of the stomach (10). However, another study yielded contradicting results (11). Both of these studies as well as others are retrospective ones with a small sample size and had several limitations, including poor reliability and statistical bias.
In a recent randomized controlled trial, prophylactic splenectomy showed no clinical impact in patients with tumors not invading the greater curvature in the upper third of the stomach (12). However, no randomized controlled trial has focused on the surgical benefits of prophylactic splenectomy on tumors invading the greater curvature in the upper third of the stomach, although some retrospective studies were reported (13).
We conducted this systemic review to clarify the surgical impact of prophylactic splenectomy for a tumor cN0 at No.10 lymph node. Of note, we paid particular attention to the surgical results of splenectomy based on the primary tumor location (the lesser curvature and the greater curvature)
Materials and Methods
Literature search. A systematic literature search was performed using the PubMed and EMBASE databases (reference period: January 1997 to March 2019). The language of publication was restricted to English, irrespective of the country of research. The following search terms were used: “gastric cancer” OR “splenectomy” OR upper third of the stomach” OR preservation of the spleen. Moreover, the reference lists of retrieved articles were manually screened to identify additional relevant studies.
The reference lists of relevant meta-analyses and primary studies were also searched to identify any studies that were potentially missed. The literature search was independently performed by multiple authors to improve the reliability of the literature search. We only selected comparative studies that focused on the significance of splenectomy for advanced gastric cancer in the upper third of the stomach. Studies that evaluated the general surgical outcomes of overall gastric cancer were excluded. A total of 816 articles were retrieved from the database search and screening of reference lists. After screening of titles/abstracts, 767 articles were excluded while 49 articles were selected for full-text review. Finally, 18 studies with a combined study population of 6,341 patients were selected for the current review (studies with poor quality and those with inadequate number of patients were excluded) (Figure 1). Out of the 18 studies, 4 studies were prospective randomized controlled trials (pRCT) and 14 were retrospective studies. Eight retrospective studies showed a positive effect of spleen-preserving gastrectomy, while 6 retrospective studies showed no benefit of spleen-preserving gastrectomy.
This work has been reported in line with preferred reporting items for systematic reviews and meta-analyses (PRISMA) (14) and assessing the methodological quality of systematic reviews (AMSTAR) (15) guidelines.
Study-selection criteria. The inclusion and exclusion criteria were defined a priori by applying the problem/population, intervention, comparison and outcome (PICO) framework. We selected randomized controlled trials and non-randomized retrospective trials that compared the outcomes between the splenectomy group and the non-splenectomy group for adenocarcinoma mainly in the upper third of the stomach. Patient characteristics, intraoperative findings, short-term outcomes (postoperative morbidity, such as pneumonia, anastomotic leakage, pancreatic fistula, intra-abdominal abscess, and wound infection), and long-term outcomes [overall survival (OS)] were compared between the two groups. Exclusion criteria were as follows: review articles, comments, letters, case reports, cohort studies with fewer than 100 cases, and studies that included patients with other concomitant cancers.
Data were extracted by two authors and confirmed by a 3rd author. In this review, OS was defined as the primary outcome. Postoperative morbidity and mortality were secondary outcomes.
Statistical analysis. Data were analyzed using the SPSS statistical software program (SPSS Inc., Chicago, IL). Patient characteristics were compared using the two-tailed Fisher exact test or the Chi-squared test with Yates correction. Quantitative variables are expressed as mean±standard deviation and between-group differences were assessed using the Student's t-test. The Kaplan-Meier method was used for survival analysis and between-group differences were assessed using the log-rank test. A random effects model was used for the pooled estimates to account for potential heterogeneity between studies and to adopt a more moderate approach. The pooled effect was considered significant if p<0.05. Heterogeneity was assessed using I2 statistic and results were displayed graphically using forest plots. Odds ratios (OR) and 95% confidence intervals (CI) were calculated using the random-effects Mantel-Haenzel method.
Publication bias of the meta-analysis was assessed by the funnel plot of standard error by log odds ratio. Probability (p)-Values<0.05 were considered indicative of statistical significance.
Results
Prospective randomized controlled trials. We found four pRCTs that compared the surgical outcomes between gastrectomy with and without splenectomy (Table I). Of these, two studies were conducted in Japan (12, 16), one in Korea (17) and one in Chile (18). These studies had a combined study population of 1,009 patients. OS was not significantly different between the two groups in any of these studies. Sano et al. have conducted a noninferiority trial to identify the impact of spleen preservation (12). They have successfully shown the noninferiority of spleen preservation with respect to OS in a cohort of 505 patients with gastric cancer not invading the greater curvature in the upper third of the stomach. Among these four trials, there was considerable variability with respect to patient characteristics, therapeutic strategies, and postoperative treatments; therefore, surgical outcomes, such as operation time, postoperative morbidity, hospital stay, mortality, and OS, differed between the trials. In each of these trials, there was no significant difference between the splenectomy and the non-splenectomy groups with respect to intraoperative factors or mortality. However, the postoperative morbidity was discernibly higher in the splenectomy compared to the non-splenectomy group. Moreover, the incidence of pancreatic fistula and intra-abdominal abscess were significantly higher in the splenectomy compared to the non-splenectomy group in two studies. In these four pRCTs, OS was not improved by splenectomy in spite of the high incidence of postoperative morbidity; therefore, they suggest that prophylactic splenectomy should be avoided.

Preferred reporting items for systematic reviews and meta-analysis (PRISMA), 2015 diagram of study selection.
Retrospective studies that showed the benefits of spleen preservation. A total of eight retrospective studies (combined n=3,676) showed the beneficial effect of spleen-preserving gastrectomy. Of these, four articles were published from Korea (19-22), three were from China (23-25) and one was from Germany (26). In four studies, the incidence of postoperative morbidity was significantly higher in the splenectomy compared to the non-splenectomy groups (19, 21, 22, 25). Two studies showed no significant between-group difference in the incidence of postoperative morbidity (23, 26), while two studies did not report on this topic (20, 24). A total of five studies reported the comparative outcomes of mortality. There was no significant difference in mortality in four studies (20, 22, 23, 26); however, one study showed barely significant difference in mortality between gastrectomy with and without splenectomy (2.7% vs. 0.4%, respectively, p=0.048) (19). The remaining three studies did not report the outcomes of mortality (22, 24, 25). All studies showed the superiority of spleen preservation for OS by univariate analysis; however, three studies showed no significant between-group difference in OS on sub-group analysis disaggregated by disease stage (19-21). Moreover, spleen preservation was not identified as an independent favorable prognostic factor for OS. Apparently, these retrospective studies had some limitations. Particularly, patient characteristics were significantly different between the splenectomy and the non-splenectomy groups. The splenectomy group comprised of patients with more advanced stage tumors and postoperative complications were more frequently observed. All studies concluded that splenectomy should be avoided unless a tumor has directly invaded the spleen and stressed the need for a well-designed pRCT (Table II).
Outcomes of prospective randomized trials.
Retrospective studies that showed no effect of spleen preservation. A total of six studies (combined n=1,656) were included in this category. Of these, two articles were published from Japan (27, 28), two were from Taiwan (29, 30), one was from China (31), and one was from Korea (32). All these comparative studies found no significant difference in OS or mortality between the splenectomy and non-splenectomy groups. Of these six studies, two studies showed a significantly higher incidence of overall postoperative complications (28, 31). These studies concluded that spleen-preserving gastrectomy is feasible for gastric cancer in the upper third of the stomach (Table III).
Meta-analysis. Postoperative complications were obtained from 14 studies. We could extract the data from 2 studies in pRCTs, 6 studies in positively supporting the effect of spleen-preserving gastrectomy, and 6 studies without difference in the effect of the preservation of the spleen. The analysis showed that the preservation of the spleen had a lower postoperative complication rate compared to splenectomy (OR=0.567, 95%CI=0.489-0.658, p<0.000) (Figure 2a), with low heterogeneity between studies (p=0.281, I2=15.8%).
Retrospective studies positively supporting the effect of spleen-preserving gastrectomy.
Retrospective studies without difference in the effect of the preservation of the spleen.
Mortality was obtained from 12 studies involving 3,693 patients reported data of mortality. The data from 4 studies in pRCTs, 5 studies in positively supporting the effect of spleen-preserving gastrectomy, and 3 studies without a difference in the effect of the preservation of the spleen were extracted. We could not find significant difference in mortality between the two groups (OR=0.776, 95%CI=0.445-1.351, p=0.370) (Figure 2b), with a low heterogeneity between studies (p=0.914, I2=0.0%).
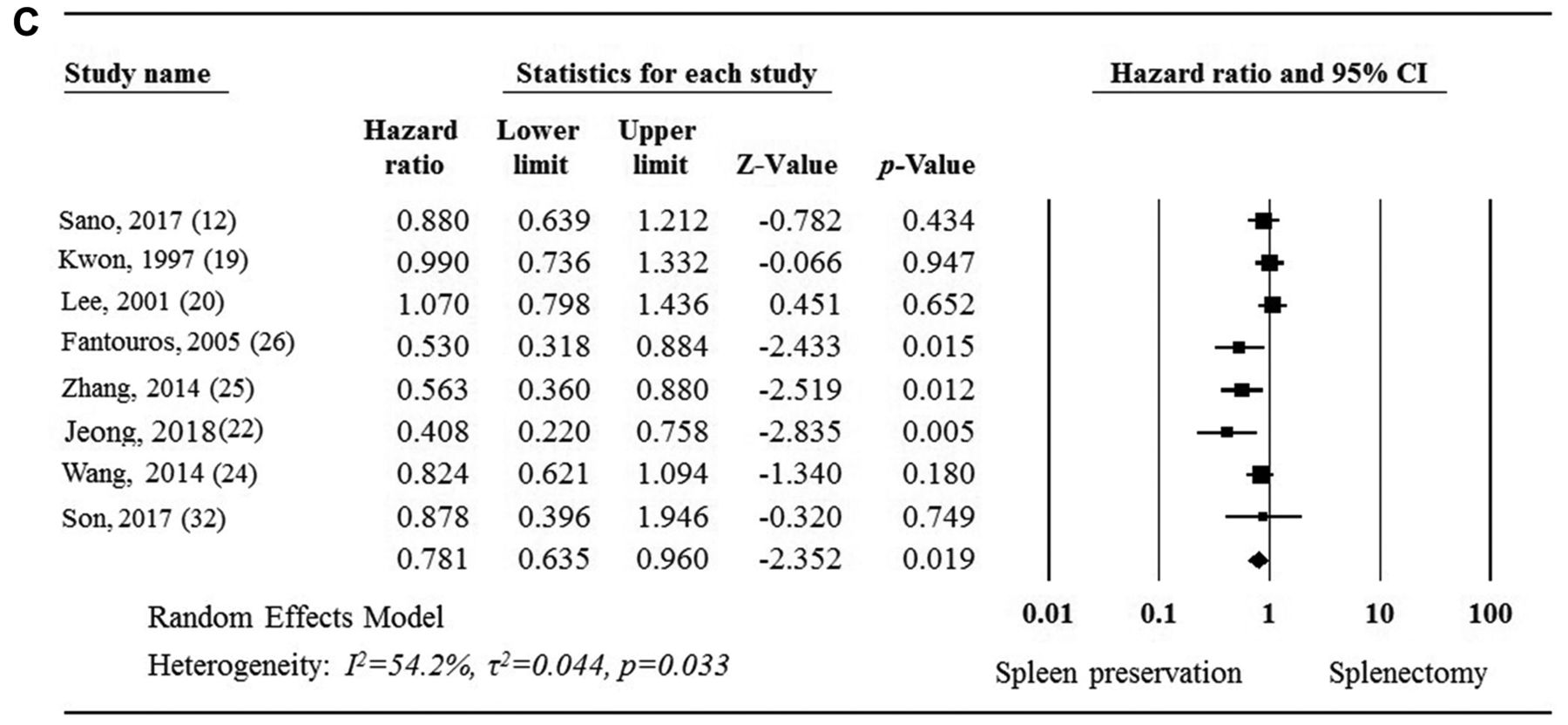
Hazard ratio (HR) for OS was acquired from 8 studies. We could extract the data of HR from one study in pRCTs, 5 studies in positively supporting the effect of spleen-preserving gastrectomy, and 2 studies without difference in the effect of the preservation of the spleen. This analysis showed that HR was favorable by the preservation of the spleen (HR=0.781, 95%CI=0.635-0.960, p=0.019) (Figure 2c), with a moderate heterogeneity between studies (p=0.033, I2=54.2%).


Forest plot of pooled odds ratio. a) Postoperative complications, b) mortality, c) hazard ratio for overall survival.
Publication bias. Publication bias of the meta-analysis was assessed using the funnel plot of standard error by log odds ratio. We could recognize that there was no publication bias in the analysis of postoperative complications (Figure 3a) although bias existed in the analyses of mortality (Figure 3b) and HR for OS (Figure 3c).
Discussion
The present systemic review showed that prophylactic splenectomy does not confer a survival benefit but is associated with a high incidence of postoperative morbidity. Therefore, a well-designed, prospective randomized controlled trial is required to identify cases for which prophylactic splenic hilar lymph node dissection with or without splenectomy can be justified.
The main goal of prophylactic splenectomy is oncological sufficiency. In Japan, prophylactic splenectomy is widely performed to facilitate complete dissection of lymph node at the splenic hilum for gastric cancer clinically without metastasis at No. 10 lymph node in the upper third of the stomach to complete D2 lymph node dissection according to the guidelines (4). As shown in this review, most studies focusing on the significance of prophylactic splenectomy have shown no favorable long-term survival outcomes in the splenectomy group. On survival analysis disaggregated by disease stage, several retrospective studies suggested no significant between-group difference in the 5-year OS according to stage; however, the 5-year OS in the non-splenectomy group was longer compared to the splenectomy group (17-21). Only a few studies have shown the feasibility of prophylactic splenectomy for advanced proximal gastric cancer irrespective of tumor stage.
In Western countries, therapeutic splenectomy has been employed for tumors invading the spleen and in cases with clinical suspicion of lymph node metastasis at the splenic hilum. One study has demonstrated the prognostic impact of splenectomy in patients with advanced proximal gastric cancer with lymph node metastasis at the splenic hilum (10). Splenectomy showed a benefit in patients with T3 tumors and was found to be an independent prognostic factor for OS; however, this was a retrospective study with some limitations. Moreover, other studies have reported no survival benefit of splenectomy for patients with metastasis at the splenic hilum (9).
No pRCTs have identified the impact of therapeutic splenectomy in patients with advanced proximal gastric cancer who have lymph node metastasis at the splenic hilum; therefore, a randomized study is required to validate the need for therapeutic splenectomy in patients with advanced gastric cancer in the upper third of the stomach.
Many RCTs and retrospective studies have shown significantly high incidence of postoperative complications following splenectomy (12, 16-19, 21, 22, 25). Pancreatic fistula, intra-abdominal abscess, and anastomotic leakage are typical complications of splenectomy. The incidence of postoperative complications differed between the studies owing to variable definitions of postoperative complications. Moreover, the sample size, surgeons' skill set, and the quality of treatment influence the outcome. These complications may sometimes lead to mortality and result in poor prognosis. Therefore, there is a need to accurately determine the indications for splenectomy. Other studies have evaluated the predictive factors for lymph node metastasis at the splenic hilum (33). No.4sa lymph node metastasis, cross-sectional location (multi-wall involvement), tumor diameter, pNstage, and pTNMstage have shown a significant correlation with lymph node metastasis at the splenic hilum. At least, it may be better to perform splenectomy for patients with suspected lymph node metastasis.
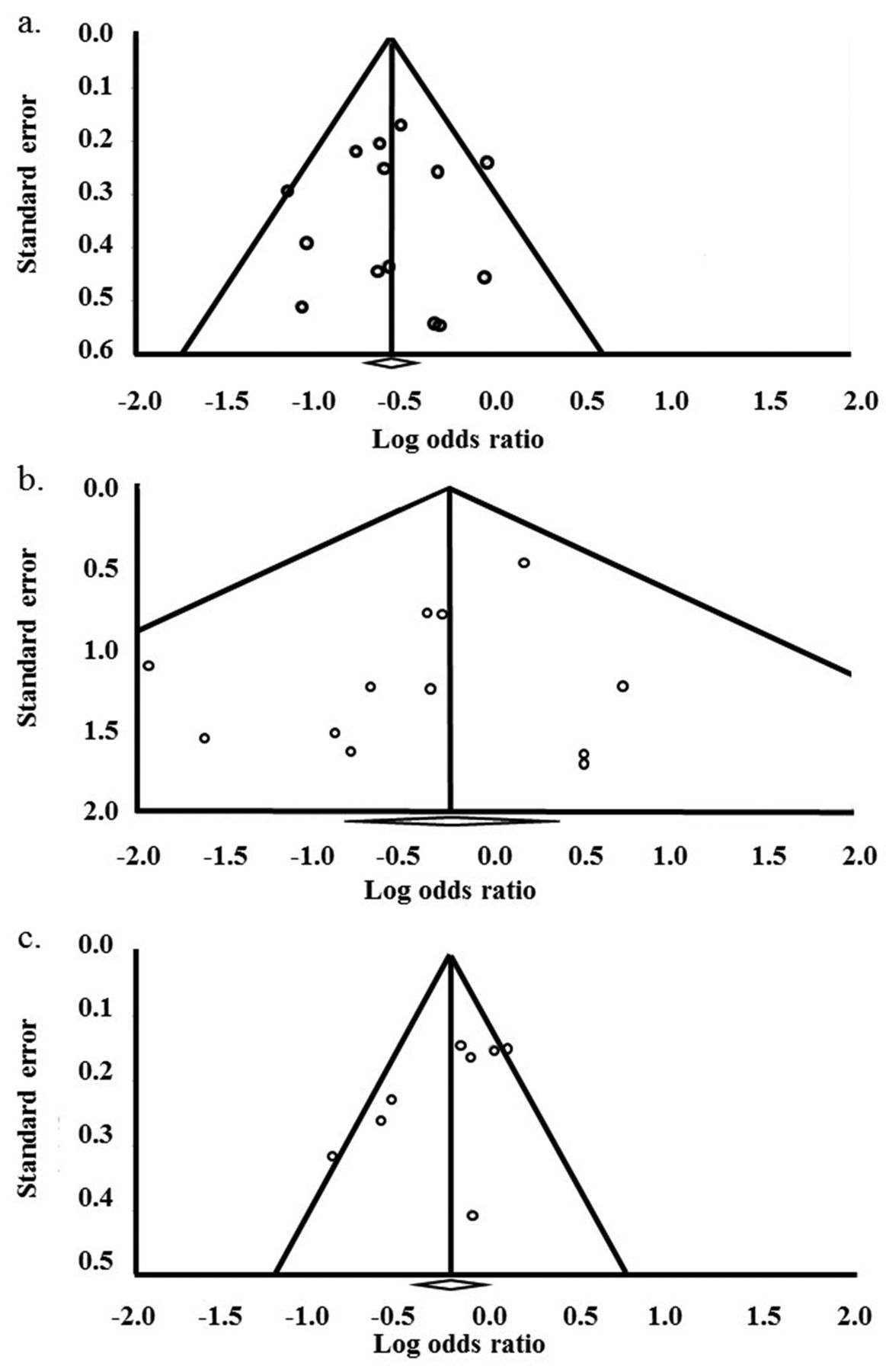
Funnel plot. Publication bias of the meta-analysis was assessed using the funnel plot of standard error by log odds ratio. a) Postoperative complications, b) mortality, c) hazard ratio for overall survival.
A recent RCT suggested the need to avoid splenectomy in patients with proximal gastric cancer and no invasion of the greater curvature; this was because splenectomy increased operative morbidity with no concomitant survival benefit (12). This study is the first study that focused on the therapeutic effect of splenectomy based on the location of the gastric tumor. No RCT has evaluated the survival benefit of splenectomy for tumors involving the greater curvature. However, a retrospective study has shown no prognostic impact of prophylactic splenectomy in spite of the higher incidence of morbidity in patients with gastric cancer invading the greater curvature (34). Conversely, two other studies have shown the necessity of lymph node dissection at the splenic hilum by evaluating the favorable therapeutic value index, as defined by the metastatic rate multiplied by the 5-year survival rate (13). The authors argued that complete splenic hilar lymph node dissection with and without splenectomy is recommended because the therapeutic value index of No. 10 lymph node was favorable. A most recent study reported the therapeutic value index in each lymph node station by the macroscopic type (type 4 vs. non-type 4) in tumors involving the greater curvature (35). The indexes in No.10 lymph node ranked seventh in type 4 and second in non-type 4 tumor. Therefore, they concluded that No.10 lymph node may be the target for dissection in tumors invading the greater curvature. However, these were retrospective studies that are liable to be affected by selection bias. Therefore, a well-designed RCT is required to confirm the validity of hilar lymph node dissection based on the ubiquity of the tumor.
Owing to recent technological advances, laparoscopic and robotic surgery has been widely employed in the field of gastroenterological surgery. One study has reported low rates of postoperative morbidity and favorable long-term survival after laparoscopic total gastrectomy with splenectomy (36). Another study has compared the short-term outcomes of spleen preservation vs. splenectomy in a small sample of patients undergoing laparoscopic total gastrectomy (37). This revealed acceptable short-term outcomes in the spleen preservation group. The debate on the subject of splenectomy has gradually moved to the next stage. Recent studies dealt with the operative approach (laparoscopic and robotic) for splenic hilar lymph node dissection but did not discuss the pros and cons of splenectomy itself. Several studies report acceptable morbidity and mortality rates after laparoscopic or robotic hilar lymph node dissection for proximal gastric cancer (38). Clear delineation of the indications for splenic hilar lymph node dissection for tumors invading the greater curvature would facilitate application of these advanced techniques in this population.
In this study there are some limitations. First, retrospective studies comparing short and long-term outcomes between the spleen preservation and the splenectomy groups with many patients are limited. Moreover, some important data were lacking in some studies. Therefore, publication bias was found in this study. Second, the number of patients was relatively small and so the reliability of obtained outcomes might be low in the prospective comparing studies used in this study. It is necessary to conduct a pRCT to clarify whether splenectomy or splenic hilar lymph node dissection would be effective and for what kind of advanced gastric cancer in the upper third of the stomach.
In conclusion, available evidence suggests that prophylactic splenectomy should not be routinely performed in patients with advanced proximal gastric cancer. pRCTs are required to determine the appropriate indications for therapeutic splenectomy or spleen-preserving hilar lymph node dissection in patients with advanced proximal gastric cancer and with cN(+) at the splenic hilum. A pRCT would help devise optimal therapeutic strategies for tumors invading the greater curvature side of the stomach.
Footnotes
Authors' Contributions
KC, EI conceived the study; KC designed the study; SS, TN, KH, KK, and KT acquired the data; AH and WJ analyzed and interpreted the data; ST and TK performed quality control of data and algorithms; KC and MT performed statistical analysis; KC and SS prepared the manuscript; KC and EI edited the manuscript; KC, SS, TN, KH, WJ, ST, TK, KK, KT, AH, EI and MT reviewed the manuscript.
This article is freely accessible online.
Conflicts of Interest
The Authors declare no conflicts of interest.
- Received September 16, 2020.
- Revision received October 2, 2020.
- Accepted October 7, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}
{kind=link}
{kind=link}
{kind=link}