


Abstract
Background/Aim: To investigate the clinicopathological characteristics of high-grade squamous intraepithelial lesions (HSILs) and squamous cell carcinomas (SCCs) involving endocervical polyps (ECPs). Patients and Methods: We collected the endocervical polypectomy cases and performed pathological examination and cytohistological correlation. Results: During a period of 12 years, 21 (1.1%) HSILs and two (0.1%) SCCs involving ECPs were identified in 1,905 cases. Twelve (63.1%) of the 19 cases were cytohistologically concordant. In five HSILs and one SCC with polypectomy margin involvement, residual HSIL was identified in conization or hysterectomy specimens. Furthermore, in two HSIL patients and one SCC patient with negative polypectomy margins, residual HSILs were found in the conization specimens. Conclusion: The prevalence of HSIL and SCC involving ECP in our cohort was similar to the rates found in previous studies. The presence of residual HSIL in nonpolypoid cervical tissue regardless of the polypectomy margin involvement suggests that conization or hysterectomy is needed for diagnostic or treatment purposes.
Endocervical polyps (ECPs) are the most common benign neoplasms of the uterine cervix that characteristically arise in the endocervical canal (1). They can occur over a wide age range, but about 90% of patients are aged >40 years (2). The reported prevalence of ECP is 1.5-10%, and its pathogenesis remains unknown. Focal reactive epithelial and stromal hyperplasia associated with repeated episodes of inflammation, an abnormal local response to increased estrogen levels, or local congestion of cervical stromal blood vessels might be involved in the development of ECP (1, 3). Approximately 60% of ECP patients is asymptomatic and discovered incidentally during routine gynecologic examinations, whereas symptomatic ECPs manifest as menorrhagia, metrorrhagia, postcoital bleeding, postmenopausal bleeding, vaginal discharge, or leukorrhea (2, 4).
Even though the reported prevalence of malignancies arising from ECP is 0.1-0.5%, a thorough literature review revealed no information about malignancies involving ECP in Asian women (2, 3). We recently experienced several patients with high-grade squamous intraepithelial lesions (HSIL) and squamous cell carcinoma (SCC) involving ECP, which initiated a comprehensive review of our archival records. In this study, we aimed to determine the prevalence of HSILs and SCCs involving ECP and to investigate their clinical characteristics and pathological features, as well as the relationship between cytology and human papillomavirus (HPV) results.
Clinical characteristics of high-grade squamous intraepithelial lesion (HSIL) and squamous cell carcinoma (SCC) involving endocervical polyp.
Patients and Methods
Patient selection. This retrospective study (4-2016-0549) was reviewed and approved by the Institutional Review Board at Severance Hospital (Republic of Korea). Cases were collected by searching the pathology database for ECP between 1996 and 2018. The search included all reports with the terms “cervical”, “endocervical”, “polypoid”, and “polyp”. We identified 1,976 patients with ECP. Multiple polyps in an individual single patient discovered less than six months apart were taken as being the same polyp. When data from an individual patient remained unchanged for six months, only the most recent data were collected. Consequently, 71 cases were excluded. Among 1,905 cases of ECP, we extracted cases with HSIL or SCC involving ECP using the histological criteria recommended by the World Health Organization (WHO) Classification of Tumours of Female Reproductive Organs (5) and the Lower Anogenital Squamous Terminology (LAST) Standardization Project (6). The clinical features were determined from reviews of the electronic medical records, or by communicating with referring gynecologists. Images were reviewed where available. The primary lesions of all 1,905 patients were histologically assessed by two board-certified pathologists specialized in gynecological oncology. They examined all available hematoxylin and eosin-stained slides, concluded pathological diagnoses, and selected representative slides for immunostaining and HPV genotyping.
Immunohistochemical staining and interpretation. Sections (4-μm thick) cut from formalin-fixed, paraffin-embedded tissue blocks were placed onto Superfrost Plus glass slides (Thermo Fisher Scientific, Waltham, MA, USA). Thereafter, the sections were deparaffinized in xylene, rehydrated through a series of graded alcohols and immunohistochemically stained using an automated Ventana Benchmark XT (Ventana Medical Systems Inc.) as described by the manufacturer (7-13). Antigen was retrieved using CC1 Cell Conditioning Solution (Ventana Medical Systems Inc.). The sections were incubated with primary antibody for p16 using prediluted clone E6H4 (Ventana Medical Systems Inc.). After chromogenic visualization using an ultraView Universal DAB Detection Kit (Ventana Medical Systems Inc.), the slices were counterstained with hematoxylin, dehydrated in graded alcohols and xylene, and then embedded in mounting solution. Appropriate positive and negative controls were concurrently stained to validate the staining method. Cervical invasive squamous cell carcinoma and endometrial serous carcinoma tissue samples obtained by radical hysterectomy were used as positive controls. According to the recommendation of the LAST Standardization Project (6), the immunostaining profile of p16 was interpreted as block positive when p16 expression was horizontally continuous and strong, with nuclear or nuclear plus cytoplasmic staining. All other p16 immunostaining profiles, described as focal nuclear, wispy, blob-like, puddled, or scattered cytoplasmic staining were interpreted as patchy positive (9, 14-19).

Colposcopy features of endocervical polyps. (A and B) Case 10. (A) Head of pedunculated polyp projects beyond external os. (B) Long stalk is apparently attached to endocervix. (C and D) Case 7. (C) Polyp protrudes from external os. (D) Small, deep red polyp resembles early granulation tissue formation. (E and F) Case 11. (E) Cylindrical polypoid mass protrudes from endocervical canal and widens external os. (F) Polyp surface has irregular-shaped superficial erosions and patchy hemorrhagic spots. (G and H) Case 13. (G) Small polyp has similar shape to that in case 7. (H) Close-up view reveals gray-to-pink, slightly nodular appearance at surface.
HPV genotyping assay. We used a commercially available polymerase chain reaction (PCR)-based microarray with a HPV 9G DNA chip (BMT HPV 9G DNA Chip; Biometrix Technology) (20-22). The 9G test detects 14 high-risk (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68) and five low-risk (6, 11, 34, 40, and 42) HPV types as described by the manufacturer. Briefly, the PCR mixture contained 10 μL of extracted target DNA, 10 μl of BMT Primer set (Biometrix Technology), and PCR premix (Biometrix Technology) contained dNTP and Taq DNA polymerase in amplification buffer. Fragments of DNA were amplified using the following cycling program: pre-denaturation at 94°C for 5 min, 40 denaturation cycles at 94°C for 30 s, 40 annealing cycles at 45°C for 30 s, 40 elongation cycles at 72°C for 30 s, and final elongation at 72°C for 5 min. The PCR products were resolved by electrophoresis in 2% agarose gels to confirm amplification. Each hybridization chamber of the 9G was covered with a mixture of the hybridization solution (35 μl) and PCR products (15 μl) and incubated at 23°C-26°C for 30 min. The array was washed, then images were acquired using a fluorescent ScanArray GX Microarray scanner (PerkinElmer Life and Analytical Sciences Inc., Waltham, MA, USA).
Results
Prevalence of HSIL and SCC involving ECP. During a study period of 12 years, we identified 1,905 patients with ECP, and most of the them were diagnosed with ECP without additional descriptors. According to the histological criteria for HSIL and SCC (5, 6), 21 and two patients each had HSIL and SCC involving ECP. The prevalence of HSIL and SCC involving ECP was 1.1% (21/1,905) and 0.1% (2/1,905), respectively.
Clinical characteristics. Table I summarizes the clinicopathological characteristics of the patients with HSIL and SCC involving ECP. The two patients with SCC were aged 53 and 63 (mean: 58) years and were postmenopausal. The mean age of the 21 patients with HSIL was 49.9 (range=30-84) years and eight (38.1%) of these patients were aged <45 years and premenopausal.
All except one patient underwent polypectomy under hysteroscopic or colposcopic guidance, which revealed ECP with various gross morphologies (Figure 1). The remaining one patient underwent hysterectomy without polypectomy. Nine (42.8%) HSIL patients were treated by cervical conization after polypectomy, and three of those also underwent total hysterectomy following conization. Four (19.0%) HSIL patients underwent only hysterectomy. One of the two patients with SCC was treated by radical hysterectomy with bilateral external iliac lymph node sampling, whereas the other patient underwent conization with no further treatment after. None of the patients received postoperative adjuvant chemotherapy or radiation therapy. Recurrent disease and metastasis did not arise in the two patients with SCC during postoperative follow-up for 11 and 21 months, respectively. The patients with HSIL were followed up for a mean of 44.3 months (range=7-173 months). All 17 (81.0%) patients with HSIL who had complete follow-up information have remained alive without evidence of recurrent disease.
Pathological characteristics of high-grade squamous intraepithelial lesion (HSIL) and squamous cell carcinoma (SCC) involving endocervical polyp (ECP).
HPV status. Information about HPV genotypes was available for 18 (78.3%) patients: 17 patients with HSIL and one patient with SCC. High-risk HPV was detected in 15 patients with HSIL and in one with SCC (type 16). The most prevalent genotype in the patients with HSIL was type 16 (7/15; 46.7%), followed by types 31 (2/15; 13.3%) and 52 (2/15; 13.3%). Types 18, 33, 39, and 68 were also detected. High-risk HPV was not detected in the remaining two patients with HSIL.
Cytohistological correlation. Cervicovaginal cytology results were available for 19 (82.6%) patients. The findings for two SCC patients were SCC and atypical squamous cells of undetermined significance (ASC-US), respectively. Seventeen patients with HSIL were diagnosed with atypical squamous cells, cannot exclude HSIL (ASC-H; 6/17; 35.3%), HSIL (5/17; 29.4%), ASC-US (4/17; 23.5%), low-grade squamous intraepithelial lesion (LSIL; 1/17; 5.9%), and negative for intraepithelial lesion or malignancy (NILM; 1/17; 5.9%). Taken together, ASC-H, HSIL, or SCC was diagnosed in 12 (63.1%) of the 19 patients with cytological results.
Pathological characteristics. Table II summarizes pathological characteristics. The mean size of ECP was 13.9 mm (range=2-40 mm). The mean size of two ECP with SCC was 15.5 (15-16) mm. Three and 18 patients with HSIL were classified as cervical intraepithelial neoplasia (CIN) 2 and CIN 3, respectively. The mean sizes of the largest ECP classified as CIN 2 and CIN 3 were 5 and 15.2 mm, respectively. Endocervical glandular extension by HSIL was identified in 19 (90.5%) patients with HSIL and two (100.0%) with SCC. Bizarre nuclear atypia, including marked nuclear enlargement (4-5-fold larger than basal cell nuclei) and severe pleomorphism, were found in six (28.6%) patients with HSIL and one (50.0%) with SCC. Mitotic activity was increased in all patients examined. Atypical mitotic figures, including tripolar, tetrapolar, and asymmetric mitoses, were detected in five (23.8%) and two (100.0%) patients with HSIL and SCC, respectively. The greatest size and invasion depth of invasive carcinoma were <1 mm in both patients with SCC (International Federation of Gynecology and Obstetrics stage IA1). In three representative cases, detailed histopathological features of HSIL and SCC involving ECP are as follows.
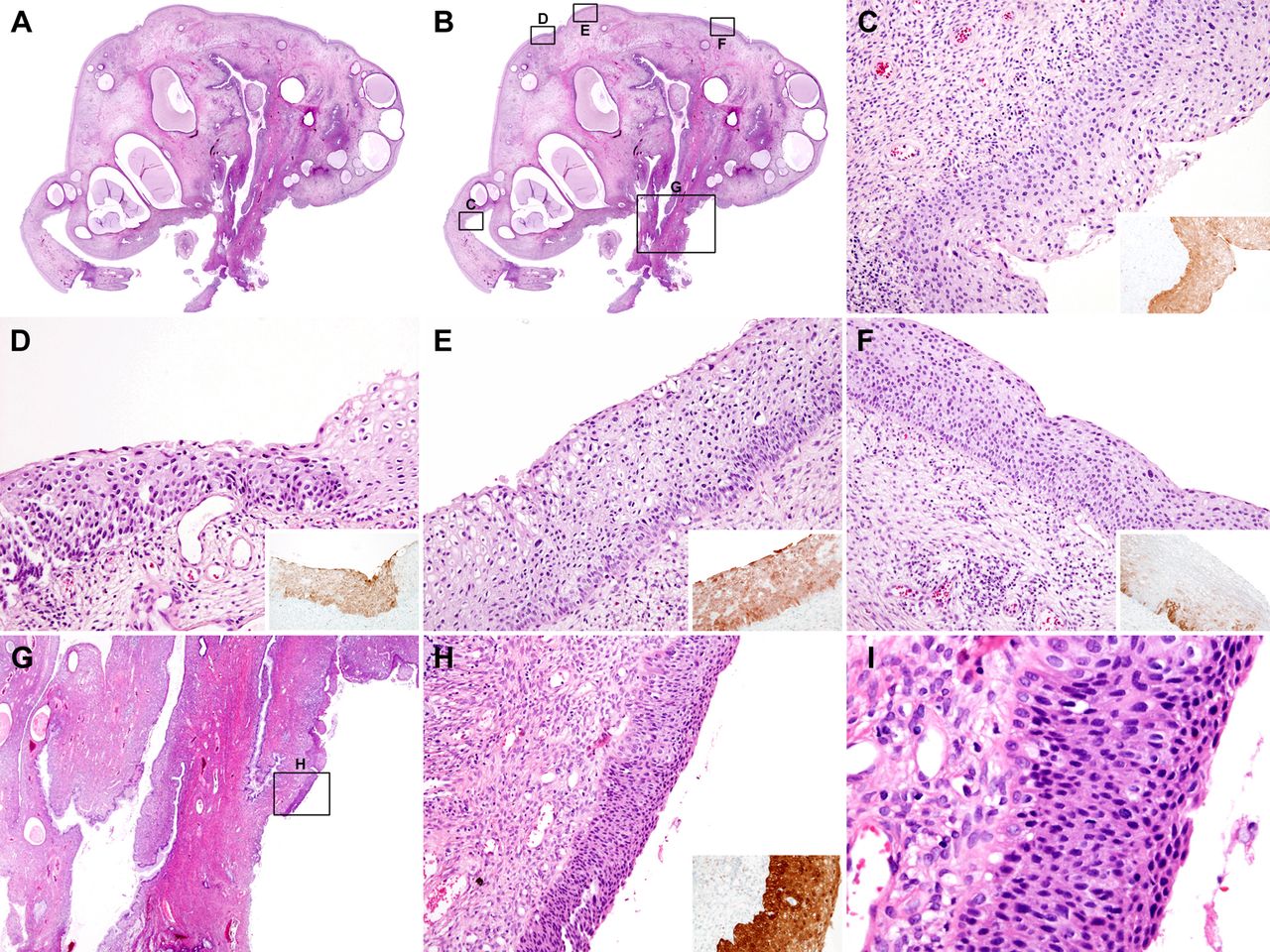
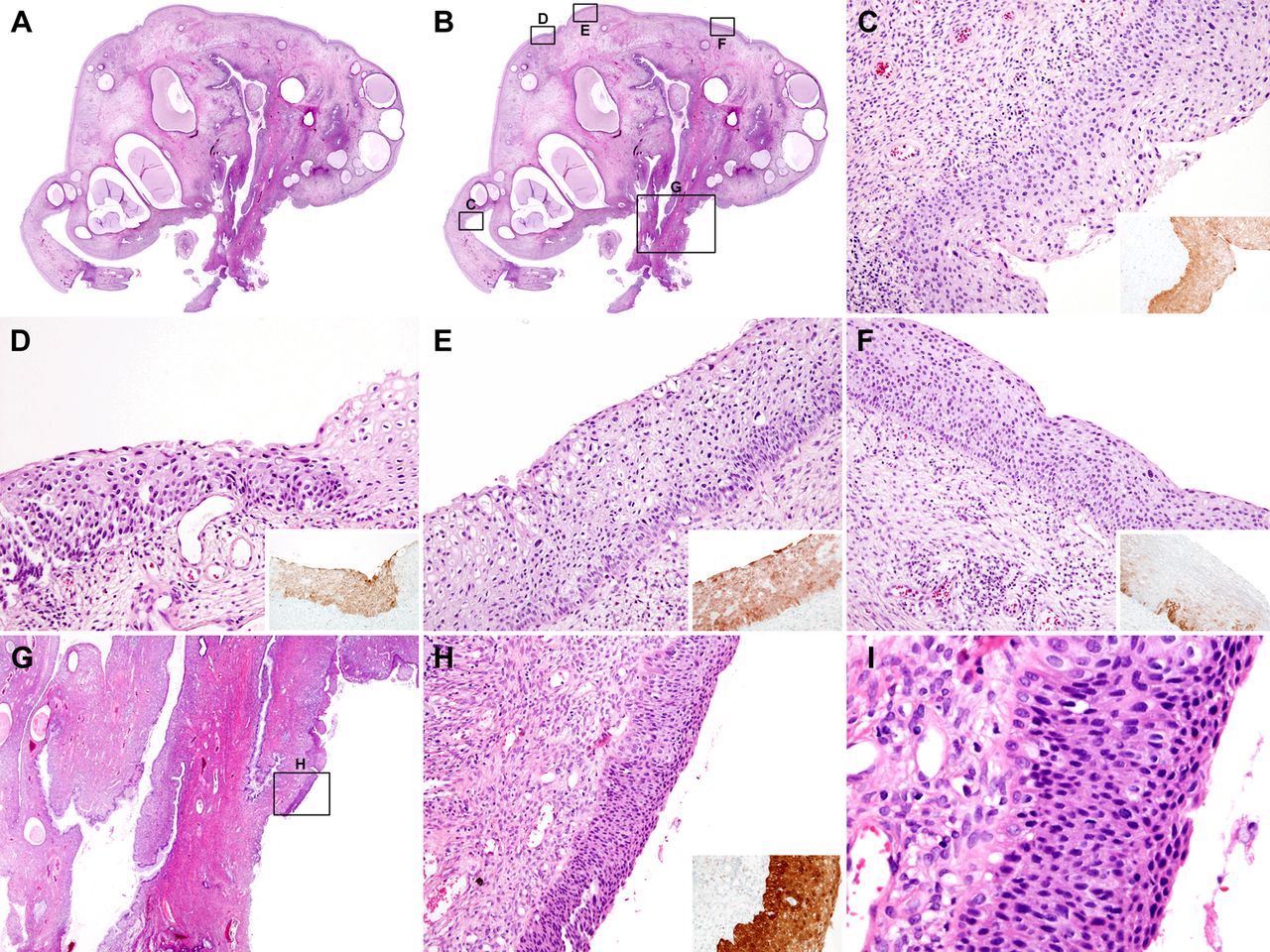
Histopathological features of endocervical polyp (ECP) in case 10. (A) Scan view. (B) Boxes indicate location of subsequent medium-power views. (C to F) Several areas show atypical squamous lesions along ECP surface and morphologically low- to high-grade squamous intraepithelial lesions, namely suspected cervical intraepithelial neoplasia (CIN) 2. Box (right lower corner) in each image shows p16 patchy positivity, indicating low-grade squamous intraepithelial lesion. (G) Another atypical squamous lesion is located at mid-portion of stalk. (H) Medium-power view reveals full-thickness proliferation of homogeneous squamous epithelium, consistent with high-grade squamous intraepithelial lesion (HSIL; CIN 3). Box (right lower corner) shows p16 block positivity. (I). High-power view shows nuclear hyperchromasia and pleomorphism occupying entire epithelial thickness.
Case 10: An umbrella-shaped, pedunculated polyp included several, round-to-ovoid, dilated endocervical glands (Figures 2A, B) and randomly scattered glandular lumina filled with mucin. A few centrally located glands also stretched along the long axis of the polyp. Fibrotic stroma contained some thick-walled blood vessels and ectatic veins. Areas of atypical squamous epithelium were patchily distributed along the surface of the polyp, with variable degrees of nuclear enlargement, hyperchromasia, and pleomorphism. Several foci showing suspected CIN 2 were observed (Figures 2C-F), but p16 immunostaining was patchy positive, which does not support the diagnosis of HSIL. A few microscopic areas of definite HSIL were p16 block positive (Figures 2G-H). The homogeneous proliferation of atypical squamous epithelial cells with severe nuclear pleomorphism at the basal and parabasal layers extending throughout the entire epithelial thickness were characteristic of HSIL (Figure 2I).
Case 11: An ovoid polyp with a short stalk had a central, ovoid, dilated glandular lumen containing clear mucinous material (Figures 3A-B). The surface of the head was almost totally consumed by HSIL, with p16 block positivity throughout the surface (Figure 3C), and HSIL extensively involved the endocervical glands embedded within the stroma. Nuclear hyperchromasia, pleomorphism (Figure 3D), frequent mitotic figures and a few atypical mitoses were features of tumor cells (Figure 3E). A small microscopic nest of tumor cells in a single focus in the stromal-epithelial junction penetrated the stroma (Figure 3F). The maximum size and invasion depth of SCC were <1 mm.
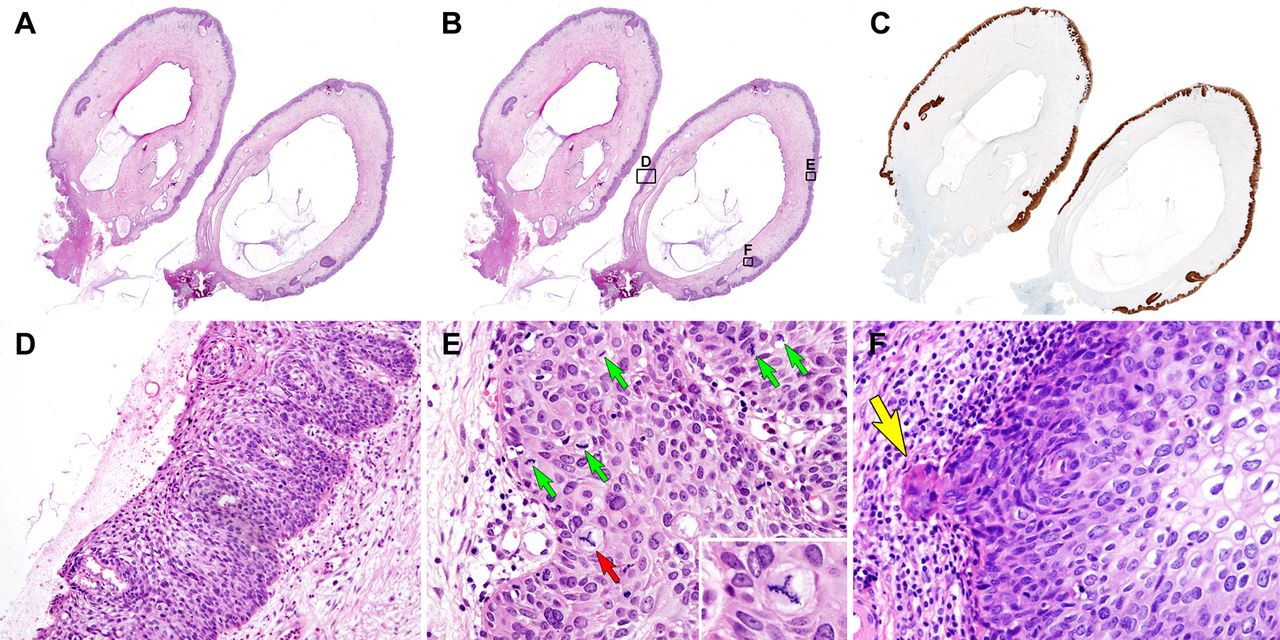
Histopathological features of endocervical polyp: case 11. (A) Scan view. (B) Boxes indicate location of subsequent medium-power views. (C) Immunostaining highlights high-grade squamous intraepithelial lesion (HSIL) with p16 block positivity. Most of polyp surface involves HSIL but not stalk or resection margin. (D) Medium-power view shows HSIL. Mild lymphocytic infiltration is evident in subepithelial stroma. (E) High-power view shows frequent mitotic figures (small green arrows). Small red arrow shows typical mitotic figure. Box (right lower corner) shows tripolar mitosis. (F) Large yellow arrow indicates microscopic stromal invasion, characterized by protrusion of tumor cells from stromal-epithelial junction into stroma. Invasive focus measures <1 mm.
Case 12: A leaf-shaped polyp featured a few centrally located, elongated, dilated glandular lumina and a broad base without a stalk (Figures 4A, B). Focal inflammatory infiltrates with granulation tissue at the tip of the polyp were probably due to chronic irritation. The HSIL extensively involved the endocervical glands with expansile growth (Figures 4C-E), and some had a keratinized surface (keratinizing HSIL). Immunostaining revealed p16 block positivity.
The resection margin was involved in polypectomy specimens of five patients with HSIL (23.8%) and in one with SCC. One patient with SCC underwent radical hysterectomy. Four HSIL patients received further treatment, and one did not. Two of the four patients with HSIL were treated only by total hysterectomy, and the other two were treated by conization and subsequent total hysterectomy. All the five hysterectomy or conization specimens except from the one patient who was not further treated had residual HSIL. Furthermore, conization specimens revealed residual HSIL in two HSIL patients and in one SCC patient, whose polypectomy resection margins were negative for HSIL or SCC. Chronic cervicitis with reactive epithelial atypia and squamous and tubal metaplasia, hemorrhage, and focal fibrosis were identified in the previous conization bed of conization specimens with no apparent residual lesions. The conization resection margin was not involved in any of these patients.
Discussion
Berzolla et al. (3) reported that the prevalence of dysplasia and malignancy arising in ECP is 0.5% (12/2,246) and 0.09% (2/2,246), respectively. Similarly, Chin et al. (23) reported that the prevalence rate of SIL involving ECP is 0.4% (7/1,900). In a larger cohort study by Long et al. (24), the overall risk of dysplasia arising in ECP was 0.3% (9/3,256). Here, we analyzed the prevalence of HSIL and SCC in a cohort of Korean patients with ECP. The prevalence of HSIL (1.1%; 21/1,905) and SCC (0.1%; 2/1,905) involving ECP in our cohort was similar to the rates found in these studies.
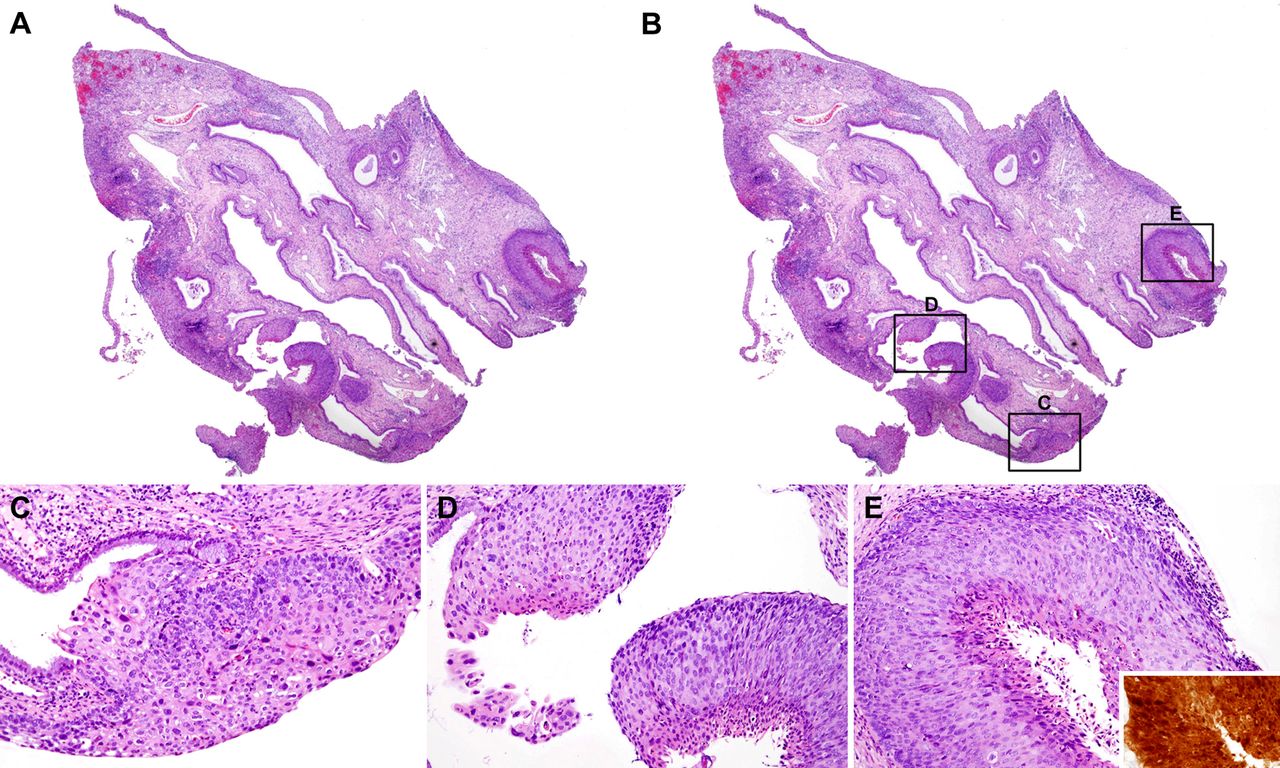
Histopathological features of endocervical polyp: case 12. (A) Scan view. (B) Boxes indicate location of subsequent medium-power views. (C to E) Extensive, multifocal glandular extension of high-grade squamous intraepithelial lesion (HSIL). Box in right lower corner of image E shows block p16 positivity.
Although eight (38.1%) of 21 patients with HSIL were aged <45 years, the average age of two patients with SCC was 58 years. The younger patients tended to have HSIL than SCC involving ECP, reflecting the fact that HSIL occurs in younger persons and progresses to SCC. Moreover, the number of patients with SCC in the present study was too small to detect a significant difference.
Histological features of invasive carcinoma in two patients with SCC comprised HSIL with protruding microscopic tumor cell nests <1 mm that extended from the stromal-epithelial junction to the subepithelial stroma, which was unlikely to be visualized by the naked eye. Moreover, the HSIL distribution on polyp surfaces was random and in various sizes; thus, identifying uninvolved regions with the naked eye was difficult. The gross appearance of the polyp surface varied regardless of HSIL as a result of erosion, inflammation, granulation tissue formation, and fibrosis from chronic irritation.
The rate of concordance between the presence of HSIL or SCC and high-risk HPV detection in the present study was 88.2% (16/18). Furthermore, when considering ASC-H and worse as a standard for cytological interpretation, the cytohistological concordance rate was 63.1% (12/19). The reason for this was most likely sampling error due to ECP being located within the endocervix and not being found during routine speculum or colposcopic examination. We also found that patients with discordant results had noncontinuous, randomly distributed HSIL areas admixed with squamous metaplasia and multifocal LSIL. In contrast, most patients with concordant results had continuous HSIL that involved most of the polyp surface and many had exposure outside the external os due to large polyps. Taken together, our results suggest that when HSIL or SCC involves ECP, the diagnostic value derived from HPV tests or cytological examinations would be limited.
Our results indicate that there are limitations in terms of predicting concurrent HSIL or SCC from colposcopic appearance, HPV status, or cytological results prior to polypectomy. Therefore, a thorough pathological examination after polypectomy is warranted so that clinicians can be informed about resection margin involvement. Five of 23 of our patients had HSIL involving the polypectomy resection margin. One patient with SCC underwent radical hysterectomy, and two patients each with HSIL underwent total hysterectomy and conization. Tissues removed from all five patients showed residual HSIL. In the absence of clear guidelines for the method of polypectomy or changing its regions, these results suggest that involvement of the polypectomy resection margin is an important factor in predicting residual HSIL even when HSIL or SCC involving ECP is not clinically suspected. Hysterectomy will be needed for patients with polypectomy resection margin involvement to remove possible residual lesions, and therapeutic conization will be necessary for those whose fertility should be maintained. However, polypectomy resection margin involvement cannot be concluded as an absolute predictor marker for residual HSIL. This is because residual HSIL was found in two patients with HSIL who did not have polypectomy resection margin involvement and in conization specimens from one patient with SCC. These findings suggest that a separate HSIL can exist in nonpolypoid cervical mucosa, and that additional treatment will be necessary regardless of polypectomy resection margin involvement.
When HSIL was accompanied by ECP, the mean size of the largest polyp with histological grade CIN 2 was smaller than that of CIN 3 (5 vs. 15.2 mm). However, the significance remains indeterminate, as only three patients had CIN 2. Differences in the mean largest size of ECP (13.9 vs. 15.5 mm) in HSIL and SCC could not be statistically compared, because only two patients had SCC. The rate and extent of the unusual histological features of HSIL, such as marked nuclear enlargement, severe nuclear pleomorphism, and atypical mitotic figures, did not significantly differ between patients with HSIL and SCC. This finding is in agreement with that of a study by Stewart (25) who reported that pleomorphic epithelial changes (marked nuclear atypia often associated with multinucleation) in HSIL do not necessarily indicate more aggressive biological behavior.
None of the patients, including the eight who did not undergo further treatment, had evidence of recurrence or metastasis during follow-up after polypectomy. Of those who did not undergo further treatment, two patients were lost to follow-up and four were followed up for less than 3 years. Therefore, observation after polypectomy should not be mistaken as a treatment option. Patients diagnosed with HSIL and SCC involving ECP should undergo treatment according to the management guidelines for HSIL and SCC without ECP until more clinical data are collected to determine the behavior. Patients in the present study were followed up for a relatively short period. Therefore, future studies should analyze the clinical course and outcomes of HSIL and SCC involving ECP in a larger patient cohort over a longer follow-up period.
In conclusion, the prevalence of HSIL (1.1%) and SCC (0.1%) involving ECP in our cohort was similar to that is previous studies. The presence of residual HSIL in nonpolypoid cervical tissues in cases with polypectomy resection margin involvement suggest that conization or hysterectomy is needed for diagnostic or treatment purposes. Since cervicovaginal cytology or HPV tests have insufficient diagnostic value as a screening tool for HSIL and SCC involving ECP, a thorough pathological examination of polypectomy specimens is required to provide sufficient clinicopathological information to clinicians for appropriate management.
Acknowledgements
This research was supported by the Chungnam National University Hospital Research Fund (2019), by the National Research Foundation of Korea (NRF) grant funded by the Korea government (Ministry of Science and ICT) (2019R1G1A1100578), and by a Grant of Translational R&D Project through Institute for Bio-Medical Convergence (Incheon St. Mary's Hospital, College of Medicine, The Catholic University of Korea).
Footnotes
Authors' Contributions
All Authors made substantial contributions to the conception and design of the study; the acquisition, analysis, and interpretation of the data; drafting of the article; critical revision of the article for important intellectual content; and the final approval of the version to be published.
This article is freely accessible online.
Conflicts of Interest
The Authors declare that they have no conflicts of interest.
- Received June 2, 2020.
- Revision received June 22, 2020.
- Accepted June 24, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Ovarian Mesonephric-like Adenocarcinoma With Multifocal Microscopic Involvement of the Fimbrial Surface: Potential for Misdiagnosis of Tubal Intraepithelial Metastasis as Serous Tubal Intraepithelial Carcinoma Associated With Ovarian High-grade Serous Carcinoma
- Invasive Stratified Mucin-producing Carcinoma (ISMC) of the Uterine Cervix: Clinicopathological and Molecular Characteristics With Special Emphasis on the First Description of Consistent Programmed Death-ligand 1 (PD-L1) Over-expression
- Mesonephric-like Differentiation of Ovarian Endometrioid and High-grade Serous Carcinomas: Clinicopathological and Molecular Characteristics Distinct from Those of Mesonephric-like Adenocarcinoma
- Clinicopathological Characteristics of Microscopic Tubal Intraepithelial Metastases from Adenocarcinoma and Small Cell Neuroendocrine Carcinoma of the Uterine Cervix
- Dedifferentiated Mesonephric-like Adenocarcinoma of the Uterine Corpus
- Diagnostic Utility of Oncomine Comprehensive Assay v3 in Differentiating Between Isocitrate Dehydrogenase (IDH)-mutated Grade II-III Astrocytoma and Oligodendroglioma