


Abstract
Background/Aim: Despite the large amount of clinical data available of Coronavirus-19 (COVID-19), not many studies have been conducted about the psychological toll on Health Care Workers (HCWs). Patients and Methods: In this multicentric descriptive study, surveys were distributed among 4 different Breast Cancer Centers (BCC). BCCs were distinguished according to COVID-19 tertiary care hospital (COVID/No-COVID) and district prevalence (DP) (High vs. Low). DASS-21 score, PSS score and demographic data (age, sex, work) were evaluated. Results: A total of 51 HCWs were analyzed in the study. Age, work and sex did not demonstrate statistically significant values. Statistically significant distribution was found between DASS-21-stress score and COVID/No-COVID (p=0.043). No difference was found in the remaining DASS-21 and PSS scores, dividing the HCWs according to COVID-19-hospital and DP. Conclusion: Working in a COVID-19-hospital represents a factor that negatively affects psychosocial well-being. However, DP seems not to affect the psychosocial well-being of BCC HCWs. During the outbreak, psychological support for low risk HCWs should be provided regardless DP.
- COVID-19
- breast cancer
- SARS-SOV-2
- DASS-21
- PSS
- score
- anxiety
- heath care workers
- psychological well-being
- multicentric study
The first case of atypical pneumonia previously named as Severe Acute Respiratory Syndrome Corona Virus 2 (COVID-19) was recorded in December 2019 in China. Italy has been the first European country to be involved in this outbreak. The national health care system (NHS) is currently reallocating resources from elective and semi-elective patients toward severe COVID-19 patients (1, 2). Italy has exceeded the cases recorded in China and unfortunately, up to now (May, 17th), 225,435 cases and 31908 deaths have been registered with still over 700 admitted to intensive care units (3). The Italian outbreak is mainly located in clusters along the north of Italy (Lombardia, Veneto and Emilia Romagna) and a low incidence in central and southern regions (1, 3, 4).
In order to control COVID-19, resource reallocation eventually led to the creation of hospitals partially or totally dedicated to COVID-19 patients (COVID-hospital), therefore increasing numbers of health care workers (HCWs) have been facing a new highly contagious infectious disease (5). In spite of having a separate route and applying infection control (IC) measures during this period, patients could refuse surgery or diagnostic procedures due to COVID-19 infection risk, reducing the number of admitted patients in the hospital (2, 6-8). Moreover, IC measures include instructions to HCWs to maintain a physical distance from other colleagues, patients and families which could eventually lead to psychological distress (9-11). Previous studies that took place during the Toronto SARS outbreak have shown that many HCWs presented high levels of psychological distress who were mostly concerned about infecting family and friends as well as about the disease consequences on their own health. Worries about their functional ability and fear of stigmatization along with social isolation and higher job stress have been described (9-11). Many studies showed HCWs who are in the front line of the diagnosis, treatment and care of patients with an emerging disease like COVID-19, are more frequently at risk of developing psychological distress and mental health disorders (12-15). Other causes of HCWs' psychological distress were strenuous workload, depletion of personal protective equipment, lack of specific drugs and the uncertainty of dealing with an illness whose transmissibility is partially understood (15).
Distribution of Breast Centre according to COVID-19 prevalence and COVID-hospital designation.
Despite the great deal of existing literature regarding psychological distress in the high-risk area, little is known about the psychological distress among HCWs at low risk and the impact of the outbreak on HCWs who aren't directly involved in COVID-19 treatment. The present study aimed to assess differences in the degree of depression, anxiety and distress among different Italian Breast Cancer Centers (BCCs) HCWs according to COVID hospital/No-COVID hospital and prevalence of the disease in the hospital district (high prevalence vs. low prevalence).
Patients and Methods
Study design. The study was designed as multicentric and descriptive. The institutional review board of Policlinico Tor Vergata waived the need for a formal approval. Due to the difference in COVID-19 prevalence (4) and national breast screening programs across Italy (13, 14), we included 4 different BCCs across Italy: Azienda Ospedaliero-Universitaria Policlinico Hospital of Modena, Campus Bio-Medico University Hospital of Rome, “Guglielmo da Saliceto” Hospital Piacenza and Policlinico Tor Vergata University Hospital. BCCs and Hospital were divided as shown in Table I. COVID-19 hospital was defined as the hospital that was totally or partially designated by the NHS as tertiary care institutions for COVID-19 disease.
Population. All HCWs from 4 Italian BCCs were invited to complete written questionnaires between April 1st and April 30th; 51 forms were collected. The main inclusion criteria were work in tertiary BCCs and no involvement with COVID-19 patients. All participants were allowed to terminate the survey at any time they wished. The population was subdivided for analysis according to demographic data, prevalence (high prevalence vs. low prevalence) and COVID hospital (COVID vs. No-COVID hospital). HCWs' roles were recorded and divided between physician, surgeon, nurse.
Questionnaires and score. An e-mail was sent to each breast cancer unit manager, informing about the study and asking for their permission to distribute the questionnaires among their employees. Blank anonymous questionnaires were placed at various designated work areas in each participating unit during the study period. All questionnaires were collected by personnel not involved in the study analysis from each BCC and were sent to Tor Vergata for analysis. To assess HCW's worries and concerns over the pandemic, their behavior during the outbreak and whether these factors were related to psychological distress and other mental health symptoms like depression, anxiety and stress, the following two self-reported questionnaires were administered: the depression, anxiety and stress scale (DASS-21) and the perceived stress scale (PSS) by Sheldon Cohen. The first part of both questionnaires' inquiries about basic demographic data (age, sex, occupation and workplace).
The depression, anxiety and stress scale – 21 items (DASS-21) is a set of three self-report scales designated to measure the emotional states of depression, anxiety and stress. Each of the three DASS-21 scales contains 7 items, divided into subscales with similar content. Participants were asked to respond according to how closely the item applied to them in the period of the outbreak. The scale uses the Likert four-level scoring system, with 0 to 3 points representing non-conformity (0) to very consistent (3). Higher scores are linked with higher level of negative emotions (14).
The total scores of these measurement tools were interpreted as follows: Depression, normal [0-9], mild [10-13], moderate [14-20], severe [21-27], extremely severe (28+); Anxiety, normal [0-7], mild [8-9], moderate [10-14], severe [15-19], extremely severe [20+]; Stress, normal [0-14], mild [15-18], moderate [19-25], severe [26-33], extremely severe [34+].
The 10-item Perceived Stress Scale (PSS) by Sheldon Cohen (16) is the most widely used psychological instrument for measuring global perceived stress and is a robust predictor of health and disease (13, 17). The scale measures global perceived stress experienced across the past 30 days on a 5-point scale: never [0], almost never [1], once in a while [2], often [3], very often [4]. Total scores range from 0 to 40. Total PSS score is classified as: 0-13 low perceived stress, 14-26 medium perceived stress, 27-40 high perceived stress.
Demographic characteristics, Mean DASS-21 and PSS score, Subdivision according DASS-21 and PSS score subdivision. Categorical variables are expressed as numbers and percentages, continuous variables are expressed as a median and an IQR (interquartile range).
Statistical analysis. All data were submitted into the EXCEL datasheet (Microsoft, Washington, DC, USA). DASS-21 and PSS-10 scores were analyzed as continuous variables and ordinal variables according to the respective classification. Due to the small sample size, all continues variables are expressed as a median and an interquartile range (IQR). t-test and ANOVA were used to determine the p-value for continuous variables. When DASS-21 score was treated as dummy variable, independent-samples Kruskal-Wallis test or Independent-Samples Mann-Whitney U-test were used to determine the p-value for nominal data or dichotomous variables, respectively. Pearson's coefficient was used to assess any correlation between continuous variables and PSS-10 and DASS-21 scores. Categorical data were recoded as numbers and percentages. Analysis was performed using the Fisher's exact test for dichotomous variable. All the statistical analyses were performed in SPSS statistical package version 23.0 (SPSS Inc., Chicago, IL, USA).
Linear correlation and DASS-21 and PSS scores. All Values are reported as a median and an IQR in the brackets. IQR: Interquartile range; R: Pearson coefficient.
Results
Demographic data. A total of 51 HCWs answered to the survey, 5 HCWs were excluded from the study as they didn't complete the demographic data or both tests (PSS-10 or DASS-21). Thus, the population consisted of 46 HCWs from the 4 different hospitals. 65.22% of the HCWs who answered the survey were females. 78.26% were medical doctors and the remaining nurses (21.74%). HCWs' population was subsequently divided according to COVID/NO-COVD and prevalence. Twenty-nine (63%) of the surveyed population worked in COVID hospital and 17 (37%) in No-COVID hospital. Grouping by districts, 27 HCWs (58.70%) worked in low prevalence areas and 19 (41.30%) in high prevalence districts (Table II).
In the general population, DASS-21 score revealed a median value of 16, 5, and 6 regarding stress, anxiety and depression, respectively. 71.74% of HCWs experienced mild to extremely severe stress level according to DASS-21 score. 32.6% HCWs experienced anxiousness and 36.95% depression symptoms. Median PSS score was 16.5. Table III summarizes calculations of linear regression between DASS-21 and PSS-10 scores with age, showing no correlations (R: 0.0217, -0.033, 0.2424, 0.1853 for DASS-21 Stress, DASS-21 Anxiety, DASS-21 depression and PSS-10, respectively).
Subdivision of the population according to sex exhibited no difference in terms of median DASS-21 stress, anxiety and depression values. Moreover, PSS scores demonstrated casual distribution between ages (Table IV).
Analyzing data regarding Profession and DASS-21 or PSS score value showed no statistical significance. Population grouping according to the level of symptoms (normal, mild, moderate, severe, extremely severe for DAS-21 score and low, medium and high perceived stress) didn't show any statistical difference in stress, anxiety and depression or perceived stress level among nurses, physicians and surgeons (Table V).
DAS-21 score and PSS score according to Sex. All values are express as medians and IQRs (interquartile ranges). All categorical data are expressed as numbers and percentages. p-Values are obtained with T-test for continuous variable and with Independent-Samples Mann-Whitney U-Test for ordinal data.
COVID No-COVID analysis. HCWs population was subsequently divided according to COVID/No-COVID hospital. As mentioned before in Table I, Piacenza-Parma Hospital and Roma Tor Vergata Breast Cancer Center were designated as COVID hospitals by the National Health system in low prevalence and high prevalence areas, respectively. Campus Bio-Medico University Hospital and Modena University Hospital were used as control for this analysis in low and high prevalence areas, respectively.
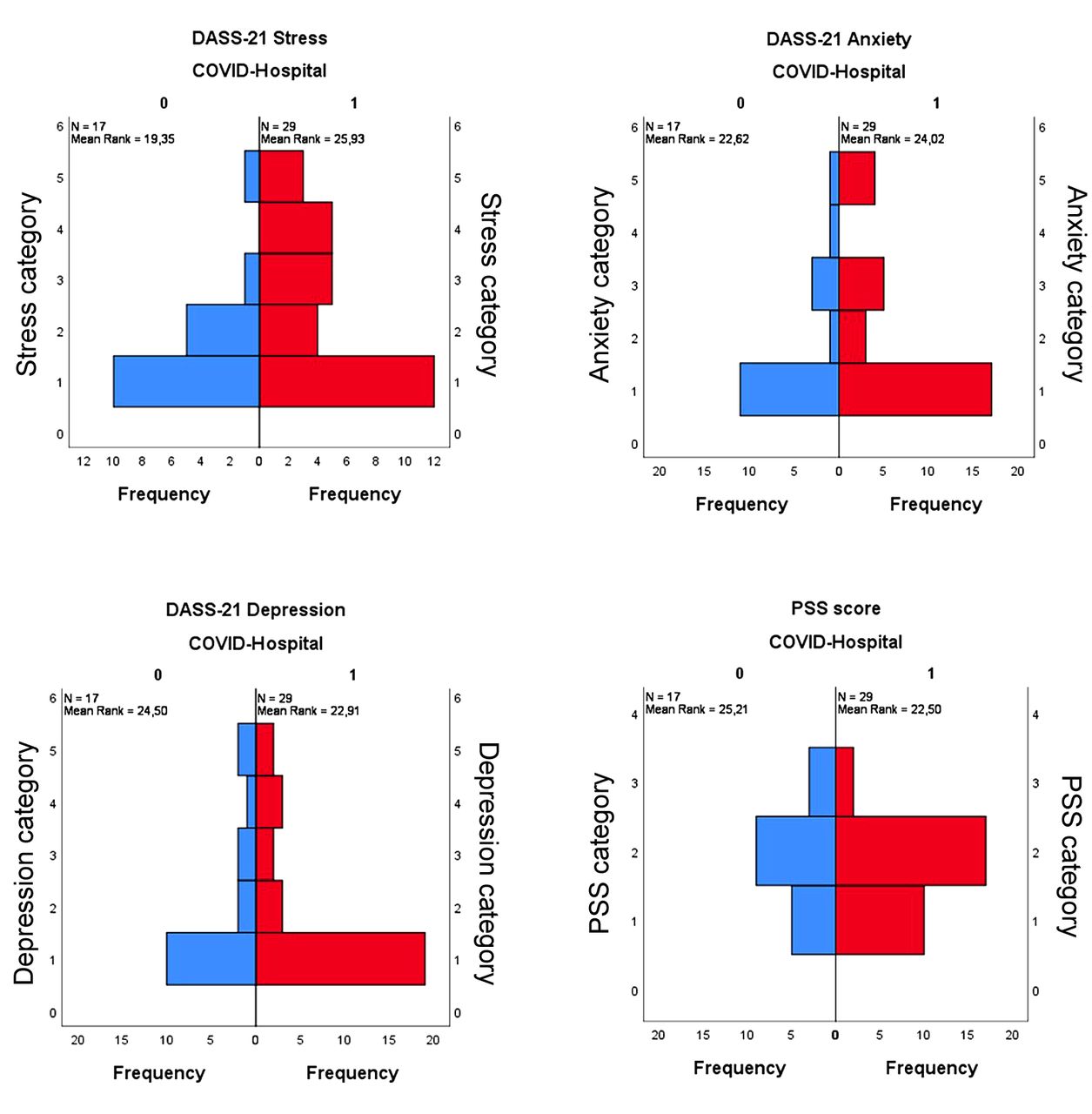
Consequently, 29 (63%) questionnaires were collected from COVID hospital and 17 (23%) were submitted from No-COVID hospital. As displayed in Table VI, the analysis did not identify any significant differences in the distribution of DASS-21 subset of anxiety and depression and PSS score in the COVID hospital compared to No-COVID hospital (p>0.05). Conversely, statistically significant distribution was found in the median DASS-21 score (p=0.043). However, independent-samples Mann-Whitney U-test failed to find statistically significant distribution between the two cohorts (p>0.05) in regard to the DASS-21 stress score according to groups (normal, mild, moderate, severe, extremely severe).
COVID Hospital HCWs exhibited lower mean value of reported stress when compared with No-COVID hospital HCWs (22.03 vs. 26.00). This result was confirmed when the PSS scores were classified as ordinal values. Greater rate of high perceived stress was observed in the No-COVID sample (No-COVID: 17.65% vs. COVID: 6.90%). Despite these data, DASS-21 stress score (COVID: 17.24% vs. No-COVID 5.88%) was found to be as expected from the distribution of the values, as mentioned before. The same result was reported for DASS-21 anxiety (COVID: 13.79% vs. No-COVID 11.76%) and DASS-21 depression score showed similar results (COVID: 17.24% vs. No-COVID 17.65%). All Distributions of DASS-21 stress, anxiety, depression and PSS scores are reported in Figure 1.
District prevalence. Due to the characteristic pattern of COVID outbreak in Italy, we divided the HCWs according to COVID-19 DP. Following the first 2 imported cases in Rome, the first Italian COVID-19 transmission was reported in Lombardy and higher prevalence was reported in the North of Italy (Lombardy, Veneto and Emilia Romagna) (3). Accordingly, Campus Bio-Medico University Hospital and Tor Vergata University Hospital were classified as low prevalence (low prevalence district) and Modena University Hospital together with Piacenza Parma Hospital as high prevalence (high prevalence district). Distribution of HCWs according to DP resulted in 19 (43.30%) HCWs in the high prevalence district while 17 (56.70%) questionnaires were collected from the control group (low prevalence group). Table VII displays the median scores and category distribution for DASS-21 stress, anxiety and PSS scores according to DP. According to our data, DASS-21 stress, anxiety and depression score distribution wasn't influenced by COVID-19 prevalence in the Hospital district (p>0.05). Although the median value of the PSS score was higher in the high prevalence district, a statistically significant difference in terms of distribution was not found between the groups. However, a high rate of severe and extremely severe scores was found in DASS-21 subsets (DASS-21 stress 21.05% vs. 7.4%; DASS-21 anxiety 26.32% vs. 3.7%; DASS-21 depression 26.32% vs. 11.11%). The same disposition was found for PSS scores of medium and high perceived stress (73.86% vs. 62.96%). Figure 2 summarizes DSS-21 and PSS-10 distributions according to district prevalence (High vs. Low).
Discussion
Breast Cancer guidelines determined a shift in the clinical and health organization in the last 20 years, resulting in better clinical outcomes for patients (18-20). In order to provide the best clinical outcome, all surgeons and physicians involved in breast cancer care spent more than 50% of their working hours with minimum caseload (20, 21). Breast Cancer treatment requires a profound knowledge of cancer behavior in order to reduce the risk of tumors progression (22-24). On the other hand, a surgical plan should be seen as an opportunity for breast remodeling that may enhance the woman's appearance (25-30). For these reasons, BCC HCWs' workload may be assumed as homogenous in terms of effect by perceived stress, anxiety and depression.
DAS-21 score, PSS score and work. All values are express as medians and IQRs (interquartile ranges). All categorical data are expressed as numbers, p-Values are obtained with One-way ANOVA for continuous variable and with Independent-Samples Kruskal-Wallis test for ordinal data.
Resource reallocation and risk of cross infection are two of the many issues that BCC HCWs are facing during the COVID-19 outbreak. Today, having no reliable data regarding the end of the epidemic, the idea of postponing all treatments until the end of the outbreak is not feasible for cancer patients. Therefore, several guidelines have been published in order reduce the detrimental effect of COVID-19 outbreak (2, 7, 8, 31-33). Triage of urgent clinical cases, awake and fast track surgery could increase the number of treated patients, reducing hospitalizations as well as the risk of cross-infection during the COVID-19 era (8, 34-38). Breast oncological treatment was only partially impaired by the COVID-19 outbreak and breast specialists try to provide the best cancer treatment for a higher number of patients (2, 7, 8, 35, 39). Hence, breast cancer specialists could provide a good model for understanding how the COVID-19 outbreak could influence health well-being among the low risk HCWs population.
In our study, age did not show any correlation with DASS-21 stress, anxiety, depression and PSS scores (R: 0.0217, - 0.033, 0.2424, 0.1853, respectively), as already demonstrated by Styra et al. in SARS outbreak (10).
In contrast to earlier findings determining that nurses are at higher risk of emotional distress in tertiary care hospital during outbreak (10, 12), our data demonstrated no difference in terms of DASS-21 and PSS scores between the different HCWs (physician, surgeon and nurse) in low risk environment. Although our results seem to contradict the data from Lai et al. and Styra et al., we underline that both works included HCWs directly exposed to index outbreak (10, 12). As stated before, our population consisted of Breast Cancer Center workers yet no one in the cohort assisted in any circumstances COVID-19 symptomatic patients. Thus, were considered at lower risk for COVID exposure.
DAS-21 score and PSS score according to COVID Hospital/No-COVID Hospital. All values are expressed as medians and IQRs (interquartile ranges). All categorical data are expressed as numbers and percentages. p-Values were obtained with t-test for continuous variable and with Independent-Samples Mann-Whitney U-test for ordinal data.
Neither sex among our population seemed to have an impact on the distribution of DAS-21 and PSS scores' higher values. In our cohort, women experienced median lower value of DASS-21 and higher value of PSS-10, without reaching statistical significance. These data are also in contrast with previous evidence which included partially or totally exposed COVID-19 or SARS HCWs (10, 12), but are in line with data from Goulia et al. during the A/H1N1 pandemic in a general hospital (9).
During the COVID-19 outbreak, the NHS reallocation of resources toward COVID-19 patients resulted in reduced availability of facilities, and even operatory theatres were transformed into Intensive Care Units (1, 2, 8). Moreover, the Health system planned the creation of COVID hospitals, totally or partially dedicated to treatment of COVID-19 patients (40). Due to the scarcity of facilities and the fear of cross-infection, we hypothesized that low risk HCWs could suffer in terms of psychosocial well-being when compared to no-COVID HCWs. Despite higher value of DASS-21 anxiety, no statistically significant distribution was found between the two populations and higher values of DASS-21 depression and PSS score were found in No-COVID HCWs. Interestingly, DASS-21 stress score values demonstrated a statistically significant distribution (p=0.043) between COVID and No-COVID hospital, yet no difference was found when populations were grouped according to ordinal variables (normal, mild, moderate, severe, extremely severe).
DAS-21 score and PSS score according to District Prevalence. All values are express as medians and IQRs (interquartile ranges). All categorical data are expressed as numbers and percentages. p-Values were obtained with t-test for continuous variable and with independent-samples Mann-Whitney U-test for ordinal data.
Similar results were obtained when the population was divided according to DP. Following two imported cases in Rome, the COVID-19 Italian outbreak emerged mainly in the northern region, determining a relevant difference in terms of cases and fatality rate across the country (3). In order to assess the impact of prevalence differences on psychosocial well-being, we divided our cohort according to the number of cases in the hospital district. High prevalence district HCWs experienced higher median value of DAS-21 stress, anxiety, depression and PSS scores. Despite these results, no statistically significant difference was found between the groups (high vs. low prevalence). Furthermore, the same result was confirmed when both cohorts were divided according to score level: despite greater rate of higher level of stress, anxiety and depression in the high prevalence population, our study failed to demonstrate a statistically significant difference between HCWs among the different districts of prevalence in terms of psychosocial well-being.

DASS-21 stress, anxiety, depression and PSS score Categories. COVID-Hospital 0: No; 1: Yes. For DASS-21 score 1: Normal, 2: Mild, 3: Moderate, 4: Severe, 5: Extremely Severe. PSS Score 1: Low Perceived Stress, 2: Medium Perceived Stress, 3: High Perceived Stress.
In line with these data, careful measures of addressing psychosocial well-being during an outbreak should be taken by the hospital despite its role during a future outbreak or the incidence of future epidemic in the hospital district. In our opinion, these data obtained from BCC HCWs should be considered, especially for HCWs who are at low risk of infection.
Our study has the limitation of the small cohort, yet population baseline data were well matched when the population was grouped according to COVID-hospital/not-COVID-hospital and COVID-19 prevalence. Moreover, the Study was designed to have 4 different certified Breast Units. The choice of BCC was made in order to obtain data from different facilities in terms of COVID-19 treatment (COVID-hospital) and COVID-19 prevalence. However, further vaster studies with a larger cohort are required for the validation of these preliminary data. Furthermore, no data were available for the period before the COVID-19 outbreak and no comparison was made with this baseline period. This limitation was mainly due to the unexpected event of the COVID-19 outbreak. We decided not to collect retrospective data of pre-COVID-19 era. If confirmed in larger series, our data show that district prevalence differences do not affect psychological well-being of low risk HCWs during the COVID-19 pandemic. Conversely, COVID hospital HCWs seem to obtain a higher value of DASS-21 score when compared with No-COVID HCWs, regardless of the COVID-19 district prevalence. Further studies are needed in order to address the long-term effect of COVID-19 pandemic on HCWs, particularly among low risk HCWs. These topics are deferred to future work.

DASS-21 stress, anxiety, depression and PSS score categories divided according to prevalence district. Low prevalence district:0; high prevalence district:1. For DASS-21 score 1: Normal, 2: Mild, 3: Moderate, 4: Severe, 5: Extremely Severe. PSS Score 1: Low perceived stress, 2: Medium perceived stress, 3: High perceived stress.
Our multicentric descriptive study demonstrated that working in a COVID-19 tertiary care institution did not affect the risk of perceived anxiety and depression symptoms among low risk HCWs during the COVID-19 pandemic and according to the COVID-19 prevalence.
Despite the absence of differences in the abovementioned data, COVID hospital HCWs experienced a statistically significant higher value of DASS-21 anxiety score, underlining the influence of hospital organization on HCWs' anxiety. In our Opinion, NHS and hospital administration should promote and provide psychological support to HCWs despite the COVID-19 prevalence in order to reduce the epidemic impact on all HCWs. Moreover, hospital administrations should take into special consideration the psychological support for HCWs in COVID Hospitals, regardless of their role in COVID management.
Acknowledgements
This study was funded with the non-conditional contribution of the Italian Ministry of Health.
Footnotes
Authors' Contributions
Study conception and design: Vanni Gianluca, Santori Francesca, Pellicciaro Marco, Buonomo Oreste Claudio; Collection of data-Tor Vergata Hospital: Cotesta Maria, De Majo Adriano; Collection of data-Campus Biomedico Hospital: Orsaria Paolo; Collection of data-Piacenza Parma Hospital: Cattadori Francesca; Collection of data-Modena University Hospital: Tazzioli Giovanni; Collection of data-project coordinator: Meucci Rosaria, Lamacchia Feliciana, Assogna Massimo; Analysis of data: Vanni Gianluca, Altomare Vittorio, Buonomo Oreste Claudio, Tazzioli Giovanni; Interpretation of data: Vanni Gianluca, Materazzo Marco, Chiaravalloti Agostistino; Article draft: Marco Materazzo, Gianluca Vanni, Caspi Jonathan; Critical revision: D'Angelillo Rolando Maria, Barbarino Rosaria, Pistolese Chiara Adriana, Perretta Tommaso, Chiocchi Marcello, Granai Alessandra Vittoria; Critical revision of literature: Ingallinella Sara, Morando Ljuba, Dalli Stefania, Portarena Ilaria.
This article is freely accessible online.
Conflicts of Interest
The Authors declare no conflicts of interest regarding this study.
- Received May 21, 2020.
- Revision received May 25, 2020.
- Accepted May 26, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Contrast-enhanced Ultrasound Using Intradermal Microbubble Sulfur Hexafluoride for Identification of Sentinel Lymph Nodes During Breast Cancer Surgery: A Clinical Trial
- Awake Breast Conservative Surgery: A Strategy to Shorten Surgical Waiting Lists During and Post COVID-19 Emergency
- Acute Appendicitis During Coronavirus Disease 2019 (COVID-19): Increasing Incidence of Complicate Appendicitis, Severity and Length of Hospitalization
- Background Parenchymal Enhancement in Contrast-enhanced Spectral Mammography: A Retrospective Analysis and a Pictorial Review of Clinical Cases
- Erector Spinae Plane Block Versus Serratus Plane Block in Breast Conserving Surgery: A Randomized Controlled Trial
- Pre-pectoral Breast Reconstruction Does Not Affect Early Immunological Response: A BIAL 2.20 Study Subanalysis
- Impact of COVID-19 Pandemic on Surgical Breast Cancer Patients Undergoing Neoadjuvant Therapy: A Multicentric Study
- Unusual Presentation of a Post-procedural Breast Hematoma: A Case Report
- Feasibility and Oncological Safety of Axillary Reverse Mapping in Patients With Locally Advanced Breast Cancer and Partial Response After Neoadjuvant Chemotherapy
- Advanced Stages and Increased Need for Adjuvant Treatments in Breast Cancer Patients: The Effect of the One-year COVID-19 Pandemic
- Lymphocytes, Interleukin 6 and D-dimer Cannot Predict Clinical Outcome in Coronavirus Cancer Patients: LyNC1.20 Study
- Delay in Breast Cancer Treatments During the First COVID-19 Lockdown. A Multicentric Analysis of 432 Patients
- Effect of Lockdown in Surgical Emergency Accesses: Experience of a COVID-19 Hospital