


Abstract
Background/Aim: Primary hepatic angiosarcoma (PHA) is a rare disease entity with variable morphologic features. Recent findings regarding ROS1 gene rearrangements in PHA may lead to new targeted therapies. Patients and Methods: Thirteen cases (4 resected specimens and 9 biopsy samples) underwent histologic review and morphologic patterns were classified according to a previous study as 1) sinusoidal, 2) peliotic, 3) vasoformative, and 4) solid (epithelioid/spindled). ROS1 immunohistochemistry and investigation of the presence of a ROS1 fusion gene by reverse transcription-polymerase chain reaction were performed in available cases. Results: Eight of 13 cases (62%) showed vasoformative patterns. Three cases (23%) were classified as sinusoidal and two (15%) as solid patterns. Mortality rate was 90% (9/10) except for three patients lost in follow up. Only one patient is still alive and has survived for 8 months with the disease. All cases tested did not have ROS1 expression (0/9) or a ROS1 fusion gene (0/4). Conclusion: We report 13 cases of PHA with 90% mortality. Vasoformative PHA is the most common histologic type. New findings on ROS1 fusion gene rearrangements could lead to the development of novel targeted therapeutics for PHA patients with dismal prognosis.
Angiosarcoma is a malignant vascular tumor arising from vessel endothelial cells. The liver is the second most common angiosarcoma site (1). However, primary hepatic angiosarcoma (PHA) is quite rare, comprising less than 2% of all primary hepatic tumors (2). A previous multi-institutional study of about 44 hepatic angiosarcoma cases revealed a poor prognosis with 5.8 months median overall survival and only two patients achieving 5-year survival (3).
Although no standard treatment has been established, surgical resection is the only treatment option that can provide long-term survival (4). According to a previous review article, partial hepatectomy in small size tumors (particularly, <10 cm) is a favorable factor (5). Chemotherapy can be an option for unresectable cases but liver transplantation is not recommended (5). Therefore, if possible, molecular therapy can be an alternative for the treatment of advanced tumors or those larger than 10 cm. Little is known about the genetic abnormalities in hepatic angiosarcoma, but a recent study by Marks et al. reported the first case of a ROS1 fusion gene rearrangement with GOPC/FIG (6). Crizotinib has now been used for pulmonary non-small cell carcinoma with a ROS1 rearrangement. In hepatic angiosarcoma with ROS1 rearrangement, ROS1 tyrosine kinase inhibitors including crizotinib can be an optional treatment. A CEP85L-ROS1 fusion was also identified in another study (7). Therefore, the presence of a ROS1 gene fusion in this disease should be further investigated.
Variations in hepatic angiosarcoma have been found at the microscopic level in several studies. Yasir et al. from the Mayo clinic, classified the morphologic patterns of 21 hepatic angiosarcoma cases into two major groups that considered whether the tumor has mass formation or not (8). “Mass-forming” tumors are further subclassified as vasoformative or non-vasoformative by the recognition of vascular space on microscopic examination (8). Non-vasoformative solid tumors can have epithelioid/or spindled morphology (8). “Non-mass-forming” tumors can be divided into a “sinusoidal” or “peliotic” pattern (8). Overall four main histologic growth patterns have been suggested: 1) sinusoidal, 2) peliotic, 3) vasoformative, and 4) solid (epithelioid/spindled) (8).
Clinicopathologic data of 13 hepatic angiosarcomas.
In our study, we aimed to describe morphologic findings in 13 cases of PHA presented at a single institute over 19 years, accompanied by clinicopathological analysis. Additionally, our study investigated ROS1 gene rearrangements by immunohistochemical and molecular analyses.
Patients and Methods
Patient selection. From June 2000 to March 2019, the pathology database of Samsung Medical Center, Seoul, Korea, was searched for all biopsy and resected specimens identified as ‘angiosarcoma’ of the liver. In total, 13 cases were selected and hematoxylin and eosin stained slides were reviewed. After examining the residual formalin-fixed paraffin-embedded (FFPE) blocks, nine of them had sufficient tissue for further ROS1 immunohistochemical analysis and six for molecular analysis. Electronic medical records were reviewed for clinical information, including demographic features, radiologic findings, treatment history, and clinical outcomes. The Institutional Review Board of the Samsung Medical Center approved this study and waived the informed consent.
Histologic classification. Histologic review of 13 cases was performed, and cases were classified according to four main classifications: 1) sinusoidal, 2) peliotic, 3) vasoformative, and 4) solid (epithelioid/spindled), as suggested by Yasir et al. (8).
ROS1 immunohistochemistry. ROS1 immunohistochemical studies were performed on 4-μm thick representative sections of FFPE tissues. Appropriate samples were obtained from nine cases of hepatic angiosarcoma. A Bond 3 Automated Immunostainer (Leica Microsystems, IL, USA) was used to retrieve antigen with ER2 solution for 20 min, and the sections were incubated with anti-ROS1 antibody (clone: D4D6, 1:100; Cell Signaling Technology, Danvers, MA, USA).
Reverse transcription-polymerase chain reaction (RT-PCR) for ROS1 fusion gene detection. Total RNA was prepared using a RNeasy FFPE kit (Qiagen, MD, USA) according to the manufacturer's protocols. A total of 2 μg of RNA was reverse transcribed using random hexamer and SuperScript III Reverse Transcriptase (Invitrogen, ThermoFisher Scientific, Waltham, MA, USA). RT-PCR amplification reactions were performed using the following conditions: an initial denaturation for 10 min at 95°C and then 40 cycles for 30 sec at 95°C, 30 sec at 59°C, and 60 sec at 72°C, followed by 72°C for 10 min. The primers for the CEP85L-ROS1 fusion gene were 5’-GCCAACAAGATGAGATTGACAGA-3’ (forward) and 5’-TAAGCACTGTCACCCCTTCC-3’ (reverse). The primers for the FIG-ROS1(S) fusion gene were 5’-CCCTTCGTAGACATATAGCTGTT-3’ (forward) and 5’-CCACTGCTGTTCCTTCATACA-3’ (reverse). The primers for the FIG-ROS1(L) fusion gene were 5’-TGGACATCGTTACCGTTTGTA-3’ (forward) and 5’- GCATTAGCCAGGCCTACTC-3’ (reverse).

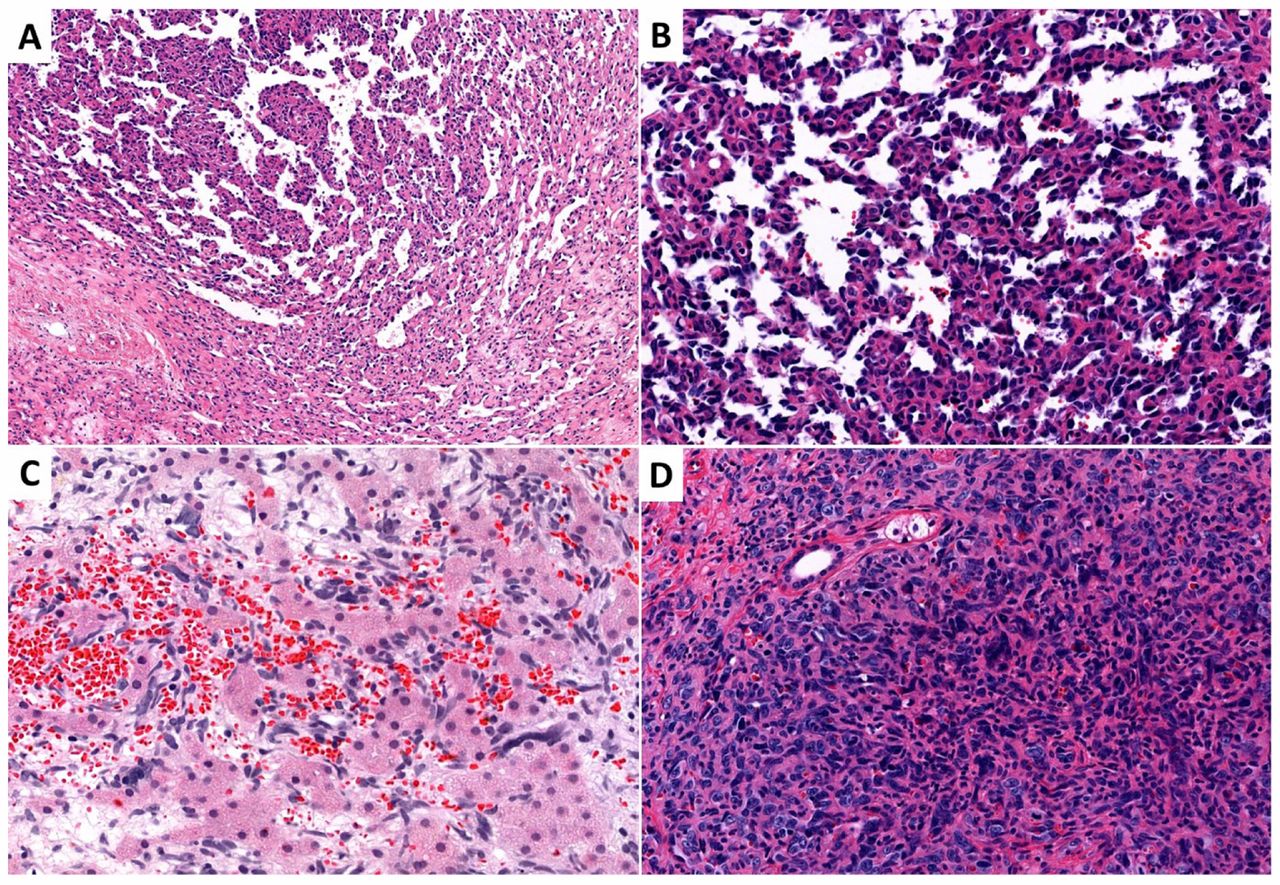
Histologic classification of primary hepatic angiosarcoma. (A, B) Vasoformative pattern, (C) sinusoidal pattern, and (D) solid pattern.
Results
Clinicopathological characteristics. The clinicopathological features of 13 angiosarcomas are summarized in Table I. Nine of the 13 patients were male and the median age at initial histologic diagnosis was 67 years old. Eleven patients had multiple masses at the initial radiologic examination. Nine patients had symptoms at the first visit, including abdominal pain and distension. Four of the 13 underwent surgical treatment, which included two liver transplantations, one lobectomy, and one trisegmentectomy. The patient who had the trisegmentectomy experienced local recurrence after the operation but refused further chemotherapy. Chemotherapy was received by four patients including one operated patient. Treatment was not possible in two patients due to the advanced stage of disease; one of these patients died 2 weeks and one at 1 month subsequent to their initial diagnoses. One patient refused treatment and died after 5 months. Initial work up findings revealed that two patients had metastatic lesions, one patient had adrenal metastasis and the other had multiple intrahepatic metastasis. After the diagnosis, multiple metastases were identified in two patients (after 2 months and 1 month). One patient who underwent transplantation and postoperative radiation therapy developed bone metastasis after 11 months. Nine died of disease progression, one patient is still alive with the disease (Case No. 11) after 8 months, and three (Case No. 10, 12, and 13) were lost to follow up.
Histological classification. Eight of the 13 cases (61.5%) showed a vasoformative pattern (Table I). They had vessel formation without parenchymal liver tissue (Figure 1A and B). Between the vascular forming area, fibrotic stroma was identified in most cases. One of the cases had a focal solid area with spindled morphology. There were three cases of sinusoidal pattern and two solid tumors with a spindled pattern. In our case series, the peliotic type was not found. The sinusoidal type showed dilated sinusoidal spaces with congestion of red blood cells (Figure 1E). Atypical cells with hyperchromasia were lined along the sinusoids and hepatic parenchyma was identified between the spaces. Two solid tumors had spindled morphology with mild whorling or storiform architecture (Figure 1F).

ROS1 immunohistochemistry (A) and reverse transcription-polymerase chain reaction for the ROS1 fusion gene (B). ROS1 expression or the ROS1-fusion gene was not detected in any of the samples tested.
ROS1 immunohistochemistry (IHC) and RT-PCR for ROS1 fusion gene detection. Nine cases had sufficient remnant tissue for further study. ROS1 IHC was used to assess them, and all cases were negative (Figure 2A). After immunohistochemistry, RT-PCR was used to investigate the presence of ROS1 fusion transcripts in six cases. Two failed due to inappropriate RNA quality that prevented cDNA synthesis, and the remaining four cases did not indicate the presence of a FIG-ROS1 or CEP85L-ROS1 fusion (Figure 2B).
Discussion
In this study, we reviewed histopathologic features of 13 PHAs over 19 years at our institute, and classified them into four categories, 1) sinusoidal, 2) peliotic, 3) vasoformative, and 4) solid (epithelioid/spindled), that were suggested by Yasir et al. (8). As a result, the most common histologic type was vasoformative (8 of 13 cases). Three of the PHAs were classified as sinusoidal, and the remaining two cases as solid. There was no typical peliotic type PHA in this study. PHA has morphologic diversity, thus pathologists should consider the variation of histologic features when facing vascular or mesenchymal tumors with suspicion of PHA. Clinical data were similar to previous studies of PHA. Males were predominant. Only one patient remains alive with the disease and nine of the 13 patients have died. The mortality rate was 90% (9 of 10), with the exception of three patients who were lost to follow up. The treatment of PHA has not been defined. In previous studies, complete surgical resection was shown to be the key to improving prognosis (9, 10). In the cases we studied, two patients went through surgical resection, but they died within 6 months with multiple metastases and local recurrence after surgery. Transplantation is now abandoned due to the high recurrence rate and poor survival (11) and PHA is now a contraindication to liver transplantation by the European Liver Transplant Registry (12). Two patients (Cases No. 2 and 4) in this study underwent transplantation in 2001 and 2008, before the recommendation. They died of the disease after postoperative chemotherapy with auto-peripheral blood stem cell transplantation and postoperative radiation therapy. Palliative chemotherapy was performed in three patients. One of the patients remains alive and has survived with the disease for 8 months so far, although intrahepatic multiple metastatic lesions were detected at the initial diagnosis. The median survival period was 5 months. The overall prognosis of PHA is dismal, compared to hepatic hemangioendothelioma with a mortality rate of 25% (13).
Recently, the ROS1 fusion genes with GOPC/FIG (6) and CEP85L (7) have been reported in angiosarcomas. We can anticipate the application of ROS1-targeted therapy in angiosarcomas with poor prognosis. Therefore, we tested ROS1 IHC in nine cases and RT-PCR for FIG-ROS1 or ROS1-CEP85L fusion transcripts in four cases, but could not find either ROS1 expression or the ROS1-fusion gene. The major limitation of this study is that we performed RT-PCR without a positive control sample. FIG-ROS1 or CEP85L-ROS1 is a very rare variant, that have been reported only in a few previous reports, and we could not find any positive control harboring such variants. Actually, the results of IHC and RT-PCR for ROS1 rearrangements have been reported to be highly concordant, and IHC is regarded as a reliable screening method for fusion gene detection (14-16). In our lab, we perform IHC, RT-PCR, and next generation sequencing in daily practice, and the results of these modalities are highly concordant. In our study, all tested samples were IHC-negative, so they could also be negative for a ROS1 rearrangement. Further studies regarding the ROS1 fusion gene are necessary in more PHAs.
Conclusion
We report 13 cases of PHAs with 90% mortality. Vasoformative PHA is the most common histologic type. Pathologists should consider variable morphological patterns including sinusoidal, solid (epithelioid/spindled), and peliotic type, in addition to vasoformative type. Although all cases tested did not express ROS1 or a ROS1 fusion gene, new findings on ROS1 fusion gene rearrangements could be key for the development of targeted therapy for PHA with dismal prognosis.
Acknowledgements
This study was funded by the Samsung Medical Center intramural grant (#SMO1161731) and the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education (NRF-2017R1C1B5017890).
Footnotes
Authors' Contributions
Conception and design: HJ, SYH; Acquisition of data: HJ, SS, CP, SYH; Analysis and interpretation of data: HJ, SYH; Drafting the article: HJ, SYH; Revising and final approval of the article to be published: HJ, HK, YJ, SS, CKP, SYH.
This article is freely accessible online.
Conflicts of Interest
None of the Authors has any conflicts of interest to declare regarding this study.
- Received February 7, 2020.
- Revision received March 2, 2020.
- Accepted March 3, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.