


Abstract
Background/Aim: Elderly patients with a single brain metastasis likely benefit from personalized treatment protocols. To add to treatment personalization, a survival score was generated for these patients. Patients and Methods: This retrospective study included 36 elderly patients, each with a single brain metastasis, who received surgery followed by whole-brain irradiation and a radiation boost. Six pre-treatment characteristics were evaluated regarding survival, namely age, gender, Karnofsky performance score (KPS), type of primary tumor, non-cerebral metastasis and interval from diagnosis of the neoplasm until surgery. Results: When applying the Cox regression model, KPS (p=0.005) and tumor type (p=0.018) were significant and incorporated in the score. Based on 12-month survival probabilities, three groups of 6-9 (n=5), 10-11 (n=15) and 14-19 points (n=16) were formed, with 12-month survival rates of 0%, 33% and 100%, respectively (p<0.0001). Conclusion: A survival score was generated specifically for elderly patients with a single brain metastasis that can improve personalization of their treatment.
- Elderly patients
- single brain metastasis
- surgery
- whole-brain irradiation
- radiation boost
- overall survival
Patients with a single brain metastasis are less common than patients with multiple lesions (1). If the brain lesion is surgically accessible and the patients are medically operable, they may be candidates for resection (1-4). Outcomes of patients with a single brain metastasis may be further improved with post-operative radiation therapy (5). A previous study of patients aged ≥65 years with one or two brain metastases compared four treatment protocols, namely whole-brain irradiation (WBI) alone, radiosurgery alone, surgery followed by WBI and surgery followed by WBI plus a radiation boost to the resection caves (6). The combined approach of surgery followed by WBI plus a boost achieved the best outcomes at 1 year in terms of significantly better survival, local control of the resected lesions and overall cerebral control. Thus, surgery followed by WBI plus a boost appeared preferable for elderly patients with one or two brain metastases. However, for many of these patients an invasive procedure such as brain surgery can be burdensome, particularly if they are impaired with underlying diseases. Moreover, in the previous study, the differences between the four treatments were less prominent at 6 months than at 1 year (6). Considering these results, an aggressive approach such as surgery followed by WBI plus a boost appeared more appropriate for longer-term survivors with comparably little co-morbidity. Therefore, it is important for the treating physicians to identify prior to the start of treatment a) patients who will likely live long enough to benefit from an aggressive multidisciplinary regimen and b) those patients who may not benefit. This study aimed to provide a score to support the estimation of a patient's survival prognosis and, thereby, contribute to the identification of patients who will likely live long enough to gain adequate benefit from such an aggressive regimen.
Patients and Methods
This retrospective study included 36 patients, each with a single brain metastasis, who were at least 65 years of age and had received surgery (resection of the metastasis) followed by WBI and a radiation boost to the metastatic site. The study was approved by the Ethics Committee of the University of Lubeck. The goal of this study was the development of a score that allowed the estimation of the 12-month survival. Six pre-treatment characteristics (Table I) were evaluated with respect to survival, including age (≤67 vs. ≥68 years, median: 67 years), gender, Karnofsky performance score (KPS 70-80 vs. 90-100, median: 80), type of primary tumor [breast cancer vs. non-small cell lung cancer (NSCLC) vs. renal-cell carcinoma (RCC)/melanoma vs. gastrointestinal cancers vs. other tumor types], non-cerebral metastasis (yes vs. no) and interval from first diagnosis of the neoplasm until surgery of brain metastasis (≤21 vs. ≥22 months, median: 21.5 months). Radiation therapy regimens included 10×3 Gy of WBI followed by a boost of 5×3 Gy (n=16), 20×2 Gy of WBI followed by a boost of 5×2 Gy (n=12), 10×3 Gy of WBI followed by a boost of 3×3 Gy (n=6), 10×3 Gy of WBI followed by a boost of 10×2 Gy (n=1) and 14×2.5 Gy plus a simultaneous integrated boost of 7 Gy (n=1).
Patient, tumor and treatment characteristics.
Time to death was referenced from the day of surgery. The characteristics that proved to be significantly (p<0.05) associated with survival or showed a trend (p<0.10) for such an association on univariate analysis (Kaplan-Meier method and log-rank test), were analyzed for independence using a Cox regression model. Characteristics achieving significance (p<0.05) in the Cox regression analysis were incorporated in the newly developed score. Initially, scoring points for each characteristic were devised by dividing the 12-month survival rates in percentage by 10. Afterwards, these scoring points were added for each individual patient.
Results
Median follow up was 13.5 months (range=1-66 months) in all 36 patients and 16.5 months (range=7-66 months) in those 10 patients alive at their last contact.
The median survival time of all 36 patients was 17 months, and the 6- and 12-month survival rates were 75% and 58%. When the univariate analyses were performed (Table II), a KPS of 90-100 (p=0.006) was significantly associated with a more favorable survival. In addition, a trend was found for comparably favorable types of primary tumor, namely breast cancer, NSCLC and RCC/melanoma, (p=0.061) and absence of non-cerebral metastasis (p=0.086). When applying the Cox regression model, KPS of 90-100 [risk ratio (RR)=3.44, 95% confidence interval (CI)=1.44-9.09, p=0.005] and favourable types of primary tumor (RR=1.22, 95%CI=1.04-1.43, p=0.018) were significant, whereas absence of non-cerebral metastasis (RR=2.39, 95%CI=0.65-7.26, p=0.176) did not achieve significance. Thus, KPS and type of primary tumor were incorporated in the score as described above.
Six- and 12-month survival rates of the evaluated characteristics.
Independent predictors of 12-month survival and related scoring points.

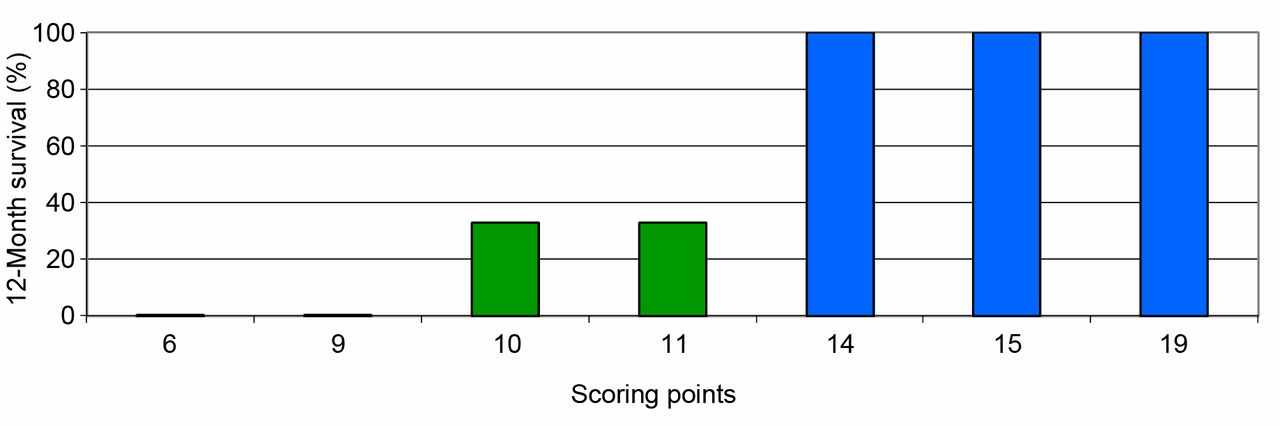
Survival rates of the different scoring points at 12 months following surgery.
The scoring points of these two characteristics are shown in Table III. When applying this methodology, individual patients received scores that ranged between 6 and 19 points (Figure 1). Based on 12-month survival probabilities, three survival groups were formed: 6-9 points (n=5), 10-11 points (n=15) and 14-19 points (n=16). The 12-month survival rates of these groups were 0%, 33% and 100%, respectively (Figure 2, p<0.0001).
Discussion
Several treatment options exist for elderly patients with a single brain metastasis including WBI alone, radiosurgery alone and surgery followed by WBI with or without a radiation boost to the resection cavity (1, 6). A retrospective study of 164 patients with one or two brain metastases compared these treatments according to the survival, intracerebral control and local control they achieved (6). At 12 months, the highest survival rate was observed after surgery plus WBI and a boost, i.e. 61% compared to 40% after radiosurgery alone, 27% after surgery plus WBI and 13% after WBI alone (p<0.001). Surgery plus WBI and a boost was also significantly superior to the other regimens with respect to 12-month intracerebral control (79% vs. 55%, 36% and 17%, respectively, p<0.001) and local control of the resected lesions (84% vs. 68%, 43% and 19%, respectively, p<0.001). At 6 months, the differences between the four regimens were less prominent (6). For example, the 6-month rates of survival, intracerebral control and local control were 78%, 82% and 86%, respectively, after surgery plus WBI and a boost compared to 56%, 48% and 53%, respectively, after WBI alone. Thus, patients surviving for ≥12 months had a greater benefit from the most aggressive approach (surgery followed by WBI and a radiation boost) than patients surviving for only 6 months. Since such an aggressive treatment program can be very stressful for elderly patients, the potential benefits should be carefully weighed against potential toxicities and complications. The benefit-risk assessment should also take into account a patient's survival prognosis, since benefit increases with lifetime. Therefore, it is important to accurately estimate a patient's remaining lifespan before considering an aggressive treatment protocol.

Kaplan-Meier curves of the patient-groups achieving 6-9 points (n=5), 10-11 points (n=15) and 14-19 points (n=16), respectively.
This study created a new survival score for elderly patients with a single brain metastasis, developed in a cohort treated with surgery plus WBI and a radiation boost. Based on the independent prognostic factors, KPS and type of primary tumor, we designed three groups with different 12-month survival probabilities. In the 6-9 points group, no patient survived as long as 12 months following surgery, and only 40% of these patients survived for 6 months. Therefore, these patients appeared less than ideal candidates for an aggressive treatment including neurosurgical resection (6). They may be better treated with radiosurgery alone that achieved the second-best results regarding survival, intracerebral control and local control in the previous study (6). Patients of the 10-11 points group had 6- and 12-month survival rates of 60% and 33%, respectively. Since the 12-month survival rate was, although better than in the 6-9 points group, also not convincingly long, surgery plus WBI and a boost may be limited to selected patients. The majority of these patients may be considered for radiosurgery alone. When wishing to combine radiosurgery with novel targeted therapies, which is becoming increasingly popular for younger patients, one should be aware that these new systemic drugs can lead to severe adverse events particularly in elderly patients (7, 8).
In contrast to these two groups (5-9 points and 10-11 points), patients of the 14-19 points group had an excellent long-term survival with 12-month and 24-month survival rates of 100% and 82%, respectively (Figure 2). These patients appear to benefit from surgery plus WBI and a radiation boost in terms of increased survival, intracerebral control and local control (6). They may also be considered for WBI plus radiosurgery, which provided similar 1-year outcomes as surgery plus WBI and a boost in a matched-pair study of 94 patients with one or two brain metastases and a matched-pair study of 92 patients of any age with a single lesion (2, 9). Studies comparing these two treatments in elderly patients alone are lacking.
The role of WBI in addition to a local therapy is currently under debate. Two older studies, a randomized trial (n=95) and a retrospective study (n=85) compared surgical resection alone to resection plus WBI for a single brain metastasis (3, 4). In the randomized trial, WBI led to increased 1-year local control (90% vs. 54%, p<0.001) and intracerebral control (82% vs. 30%, p<0.001) but not survival (median 11 months in both groups) (3). In the retrospective study, WBI resulted in increased 1-year local control (79% vs. 15%, p<0.05) and survival (median 23 vs. 11.5 months, p<0.05) (4). More recently, two randomized trials demonstrated that WBI when added to radiosurgery resulted in a significantly higher rate of cognitive decline after a few months (10, 11). However, in both trials, significantly more intracerebral recurrences were found after 12 months in the radiosurgery alone arm. One has to be aware that intracerebral progression can also be associated with impairment of cognitive function, as well as the need for further therapy (12). Patients who have a considerable risk of developing an intracerebral recurrence after radiosurgery alone should be considered for upfront WBI (13). If a patient is assigned to a local therapy plus WBI, the risk of cognitive decline can be significantly reduced with WBI-techniques sparing the hippocampal areas and with administration of memantine, which is normally used for dementia and Alzheimer's disease (14-16). These options should be considered particularly for patients achieving 14-19 points in our study, who are assigned to surgery plus WBI and a boost. When following the recommendations given in this article, the retrospective nature of the study with its risk of bias should be kept in mind.
In summary, a survival score was generated specifically for elderly patients with a single brain metastasis. This new score can improve personalization of their treatment by identifying patients who may be helped with an aggressive treatment protocol such as surgical resection followed by WBI and a radiation boost to the resection cavity.
Footnotes
Authors' Contributions
D.R., T.N. and S.E.S, designed the study. T.N. and D.R. collected or provided data that were analyzed by D.R. and S.E.S. The draft of the article was written by D.R. and S.E.S. and subsequently reviewed and approved by all Authors.
This article is freely accessible online.
Conflicts of Interest
On behalf of all Authors, the corresponding Author states that there are no conflicts of interest related to this study.
- Received February 19, 2020.
- Revision received March 25, 2020.
- Accepted March 26, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.