


Abstract
Background/Aim: Clinical management of testicular germ cell tumours (GCT) is based upon the measurement of serum tumour markers. Recent studies have shown that the microRNA-371a-3p is a sensitive and specific serum biomarker for all subgroups of GCT, except teratoma. To close the diagnostic gap relating to teratoma, serum levels of microRNA-375-3p have recently been suggested to represent a specific serum marker of this histological subgroup. In the present study, we tested this hypothesis. Materials and Methods: miRNA expression was analysed in serum of 21 GCT patients with teratoma, twelve patients with other GCT, and twelve male controls using the qPCR method. Results: The serum miR-375-3p levels of teratoma patients were not different from other GCT patients or controls. The ROC analysis revealed an AUC of 0.524 for the discrimination between teratoma and other pathologies. Conclusion: The miR-375-3p does probably not qualify for a useful serum biomarker to distinguish teratoma from other GCTs and from controls.
The clinical management of testicular germ cell tumours (GCTs) greatly rests on the measurement of the classical serum tumour markers beta human chorionic gonadotropin (bHCG), alpha fetoprotein (AFP) and lactate dehydro-genase (LDH) (1). A major limitation of these biomarkers is that they are differently expressed in the various histological subgroups of GCTs. In seminoma, the most frequent subgroup, bHCG and LDH are expressed in roughly 30% of cases, while AFP is not (2). In nonseminoma, the other main subgroup, all three markers are expressed in 30-60% of cases (3, 4). However, nonseminomas may comprise of four histologic subtypes each of which having its specific marker pattern. As several histological subtypes may occur simultaneously in one nonseminomatous tumour (5), a variety of marker patterns is possible in the entire group of nonseminomas (2). Yolk sac tumours usually express AFP, only. Choriocarcinoma specifically expresses bHCG. Embryonal carcinoma usually does not express any marker, but may show AFP elevations in isolated cases. Teratoma the most differentiated subtype does not express any of the markers (4). LDH is an unspecific marker that may be elevated in any of the subtypes of GCT except for teratoma. Recently, serum levels of microRNA-371a-3p (miR-371a-3p) have been shown to represent a novel serum biomarker of GCT with much higher sensitivity and specificity than the three classical markers (6). Importantly, this new marker is likewise informative for seminoma and nonseminoma. However, miR-371a-3p levels are not elevated in cases with teratoma (7). As the presence of teratoma in metastatic deposits is a challenge in clinical decision-making in many cases, it would clearly be beneficial to have one serum biomarker that is associated with the presence of this particular GCT subtype. In a recent publication on the role of miRs in GCTs, microRNA-375 was reported to be present in the tissue of teratoma. Although this miR had, so far, not been evaluated in serum it was considered a candidate biomarker for this particular subtype of GCTs (8). We, therefore, looked to the presence of this miR in the serum of patients with teratoma. Our aim was to test the hypothesis that serum levels of miR-375-3p might represent a valuable serum biomarker of teratoma.
Materials and Methods
Patients. Serum samples of 21 patients (median age: 34.5) with teratoma were examined for miR-375-3p (miR-375-3p) expression before treatment. Sixteen patients had testicular primary tumours consisting of pure teratoma without metastases [clinical stage (CS) 1]. Three patients had residual retroperitoneal masses after chemotherapy surgically proven to consist of teratoma only (CS2). Two other patients had both retroperitoneal and mediastinal metastases that were surgically resected and likewise proven to consist of pure teratoma (CS3). The patients were retrospectively recruited for the present study and serum samples for analysis were derived from a serum bank. All of the patients had participated in previous studies on miR-371a-3p (7, 9). Serum samples from twelve patients (median age: 36.0) with non-malignant scrotal diseases (hydrocele, epididymitis) served as controls. We also analysed twelve serum samples of patients with other GCT (median age: 34.5 years). Individual data regarding the patients and controls are given in Table I.
All patients gave informed consent. The study has been ethically approved by Ärztekammer Bremen (#301, decisions Jul 08 and Oct 08, 2015). All study activities had been conducted according to the Declaration of Helsinki of the World Medical Association (as amended by the 64th General Assembly, 2013).
Laboratory methods. Blood samples were collected in serum separations tubes (Sarstedt, Nümbrecht, Germany) and kept at room temperature for 1 h to allow for complete coagulation after blood aspiration. The blood samples were centrifuged for 10 min at 2,500 × g to separate serum, and aliquots were stored at −80°C until examination for study purposes. Serum levels of miR-375-3p were measured by quantitative real-time polymerase chain reaction (qPCR) as reported earlier for other miRs (10, 11). Briefly, total RNA was extracted from 200 μl serum using the miRNeasy Mini Kit (Qiagen, Hilden, Germany). Reverse transcription (RT) was performed using the TaqMan MicroRNA Reverse Transcription Kit (Applied Biosystems, Darmstadt, Germany). The RT product was preamplified, and levels of miR-375-3p (assay ID: 000564) and miR-30b-5p (assay ID: 000602) were measured by qPCR with TaqMan miRNA assays using the Applied Biosystems 7500 real-time PCR System (Applied Biosystems, Darmstadt, Germany). All PCR experiments were carried out in triplicate using the FastStart Universal Probe Master (Roche, Mannheim, Germany). Cycle threshold (Ct) values were normalised to miR-30b-5p as an internal control, and the relative quantity (RQ) was calculated using the 2-ΔΔCt method (12).
The miR-375-3p expression of the various groups is presented as median with interquartile ranges (IQR). The statistical evaluation was carried out with SPSS. Receiver operating characteristics (ROC) analysis was performed to assess the ability of miR-375-3p serum levels to differentiate between teratoma and other conditions. For the analysis of differences between two independent variables, the Mann-Whitney U-test was used. The null hypothesis was that there would be no differences between patient groups and controls and the alternative hypothesis was that miR-375-3p expression would be at variance among the groups. Significance was assumed at p<0.05.
Results
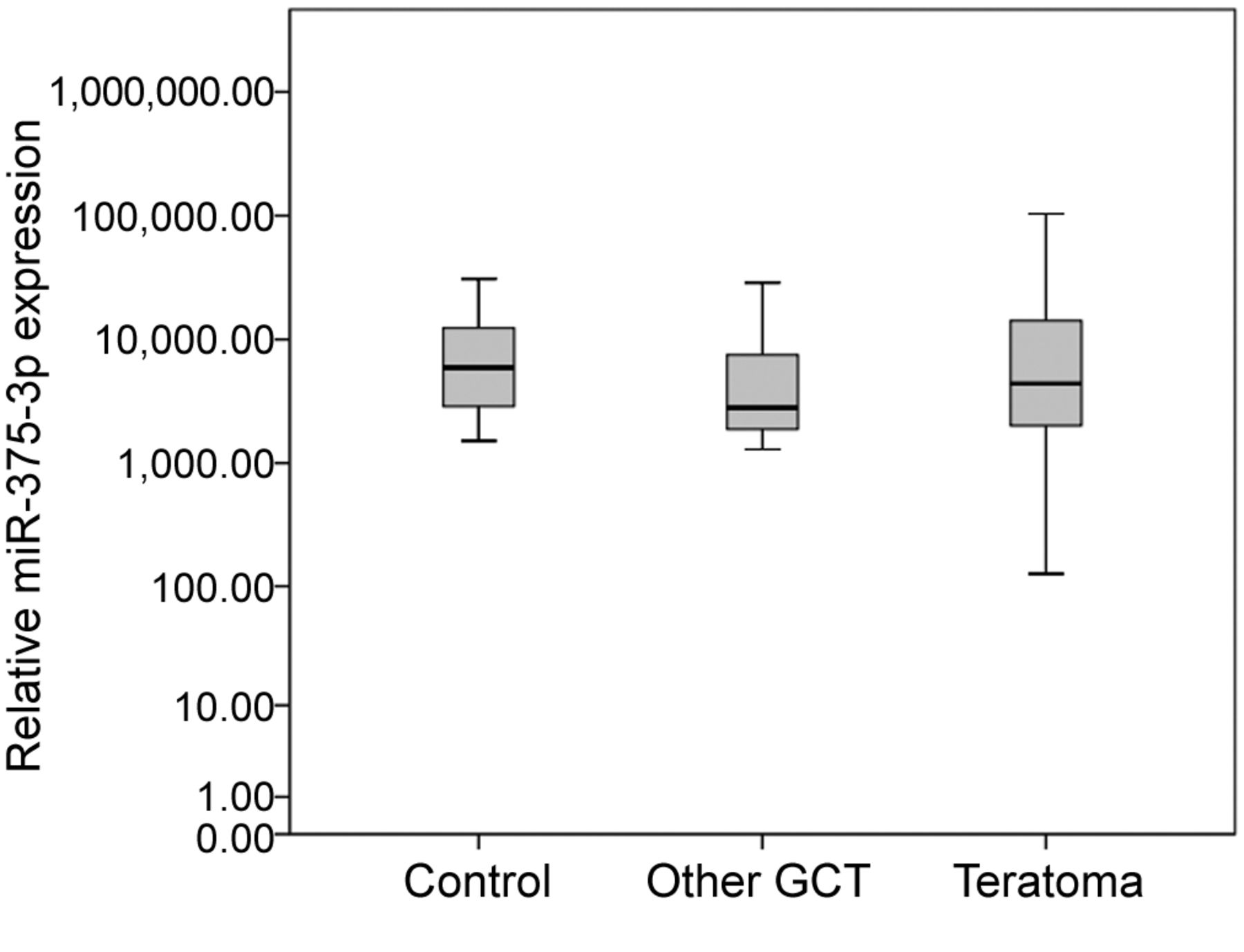
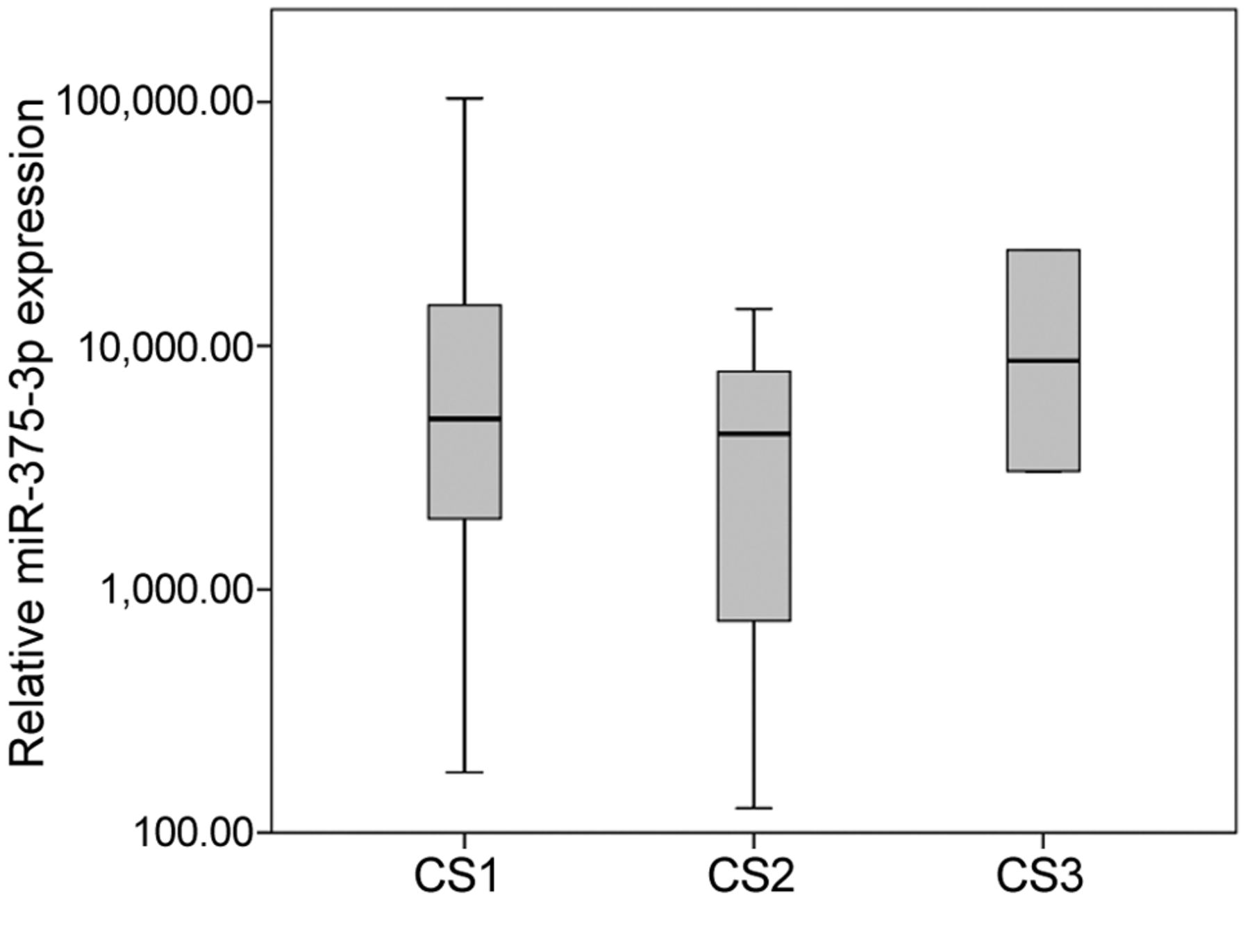
The median relative miR-375-3p expression in 21 patients with teratoma was 4,390.0 (IQR=15,284.2), compared to a median expression of 2,800.1 (IQR=6,513.5) in 12 patients with GCT, other than teratoma, and 6,163.8 (IQR=10,554.7) in 12 patients with non-malignant testicular disease (Figure 1). The differences between these groups were not significant. Stratified for clinical stage the CS1 teratoma patients (n=16) had a median relative miR-375-3p expression of 5,071.3 (IQR=15,954.6). The CS2 (n=3) and CS3 (n=2) patients had a median expression of 4,359.7 and 13,861.7, respectively (Figure 2). Again, these differences were not significant.
The discriminative power of miR-375-3p as a serum marker for teratoma was assessed with ROC analysis by comparing the 21 teratoma patients with the 24 patients without teratoma (patients with other GCTs and patients with non-malignant testicular disease grouped together). The area under the curve (AUC) was 0.524, which was not significantly different from an AUC of 0.5, the area of chance results (Figure 3).
Discussion
The hypothesis that serum levels of miR-375-3p might be a valuable biomarker of teratoma as forwarded by Shen et al. (8) is not supported by the present study. In particular, the median serum level of miR-375-3p found in teratoma patients was not different from the median levels found in other GCT patients (those without teratoma) and healthy males, respectively. Moreover, if one assumed that the miR was associated with teratomatous tumours then higher expression rates in serum would have been expected in patients with large and bulky tumours than in those with small tumours. However, as shown herein, bulky teratomatous tumours (clinical stages 2-3) did not express significantly higher serum levels than patients with clinical stage 1. Accordingly, the sensitivity and specificity of serum miR-375-3p levels to detect teratoma are very low as shown in the ROC analysis that revealed an AUC of only 0.524, which is not significantly different from null findings with an AUC of 0.5. All in all, according to the present findings, miR-375-3p levels are probably not capable of discriminating teratoma from other pathologies.
Our results seem contradictory to the results of Shen and colleagues (8), especially since a correlation between intra-tumor and serum levels has been shown for miR-375-3p and other miRs (13, 14). However, the reason for the low discriminative ability of miR-375-3p as documented in our study was not the lack of expression in teratoma serum but rather the equally high expression in serum of other GCT patients and controls. Modified expression of miR-375-3p is known in other cancer types like esophageal squamous cell carcinoma and osteosarcoma, where a downregulation of that miR is indicative for poor prognosis (13, 15).
A serum biomarker sensitive and specific for teratoma would be particularly valuable in the assessment of residual tumour masses after chemotherapy of advanced nonseminomatous GCT. Currently, guide-lines recommend surgical resection of any residual mass that is larger than 1 cm (1). However, the histological evaluation of surgical specimens of these cases revealed that in approximately 40-50% the residual masses consisted of necrosis or fibrosis only, while 30-40% had teratoma and only 10-20% had viable residual cancer (16, 17). By retrospective analysis it becomes clear that 50% of these major surgical procedures are being performed without any clear benefit for the patient because only necrosis is excised. A recent study showed that all of the patients with viable cancer in the resected specimen had elevated levels of miR-371a-3p preoperatively (18). Unfortunately, it is currently not possible to differentiate those with teratoma from those with necrosis/fibrosis prior to surgery. Therefore, residual masses with negative miR-371a-3p levels after chemotherapy remain indeterminate because they may have either teratoma or necrosis. Clinically, teratoma does definitely require surgical excision while necrosis/fibrosis could be left untreated. Thus, no clear therapeutic decision regarding surgery can be based on the miR-371a-3p test in that setting. A great deal of enthusiasm evolved among clinicians caring for GCT patients when the hypothesis of miR-375 being informative for teratoma was forwarded. The results of the present study, however, probably disprove that hypothesis.
Clinical data of serum from the analyzed patients.

Boxplots of the relative miR-375-3p serum expression. Expression in serum of n=12 patients with non-malignant testicular disease (control), n=12 patients with testicular germ cell tumours (GCT) other than teratoma, and n=21 patients with teratoma was compared. The y-axis is plotted in a logarithmic scale.
The present study is, of course, not without limitations. The small sample size of only 21 patients with teratoma does leave the possibility of chance results. On the other hand, GCT as such is a rare disease and the subgroup of pure teratoma is even rarer. Therefore, the sample size of n=21 appears at least acceptable for the purpose of this study particularly in light of the clear-cut results documented herein. Also, the retrospective study design with the use of serum samples from a serum bank may induce chance effects. Teratoma may comprise of various histological features such as cartilage or bone structures, muscular tissue or gland structures and other histological formations (19). We did not perform a histological subclassification of our patients. So, it is at least conceivable that for some particular subtypes of teratoma the miR-375-3p may indeed be an appropriate marker.
In conclusion, the miR-375-3p does not qualify for a serum biomarker to distinguish teratoma from other GCTs and from controls. Therefore, an informative biomarker of teratoma is still missing. However, we have only very recently started to understand that serum levels of miRs may serve as disease markers (20, 21). Currently, more than 2000 miRs have been identified in the human body with an ever-growing number.
In the future, large scale micro-array studies may possibly reveal novel markers that may also be sensitive for teratoma. A possible candidate being a part of the micro array would be the microRNA-301, which is expressed in differentiated tissues like teratoma (22). An additional option for classification between different GCT subtypes is gene expression profiling to find specific gene signatures for teratoma (23).

Boxplots of the miR-375-3p serum expression in teratoma patients with different clinical stages (CS). Expression was compared between n=16 patients with CS1, n=3 patients with CS2, and n=2 CS3 patients. The y-axis is plotted in a logarithmic scale.
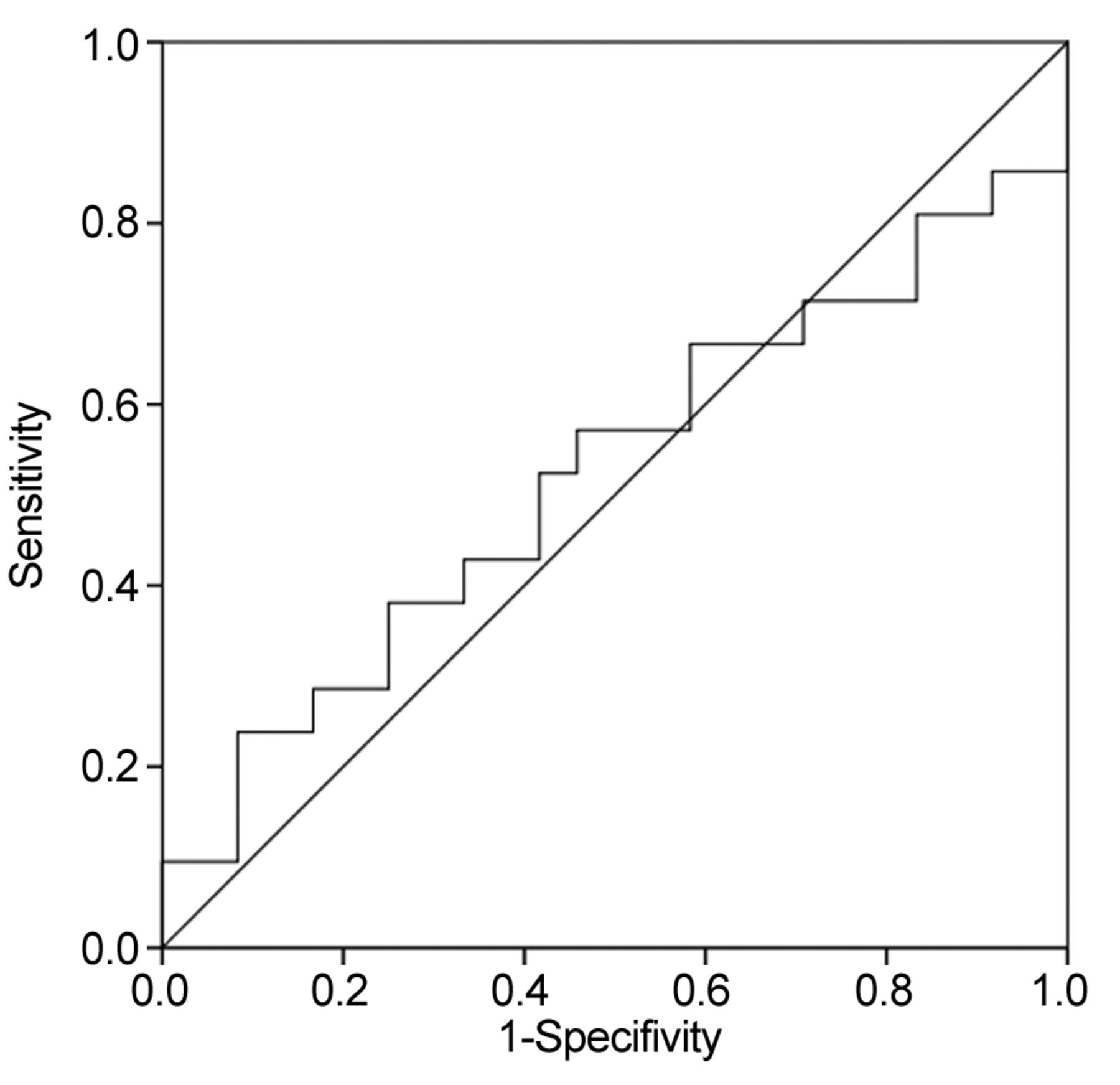
ROC curve representing the ability of serum miR-375-3p to discriminate between teratoma (n=21) and other conditions (n=24). The AUC is 0.524.
Acknowledgements
The Authors gratefully acknowledge the technical assistance of the laboratory staffs of the University of Bremen and Asklepios Klinik Altona, Hamburg.
Footnotes
Authors' Contributions
G.B., A.R., K.P.D. designed the study; K.P.D., C.M. patient enrolment, G.B., A.R., F.G. executed the experiments, G.B., A.R., K.P.D., F.G. analysis and interpretation of the data; A.R., F.G. statistical analysis; G.B., A.R., K.P.D., F.G., C.M. drafting of manuscript. All authors critically revised and finally approved the manuscript.
This article is freely accessible online.
Conflicts of Interest
KPD and GB each possess 12.9% ownership shares of miRdetect GmbH, Bremen, a start-up company aiming to develop a commercially available test for measuring miRs in serum. miRdetect holds a patent for the measurement of miR in body fluids at the limit of detection. AR is an employee of miRdetect GmbH, Bremen since the beginning of 2019. All other authors declare no competing interests towards this report.
Funding
The present study received support from Wilhelm Sander Stiftung, München (No, 2014.178.2). The sponsor had no role in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
- Received September 5, 2019.
- Revision received October 5, 2019.
- Accepted November 5, 2019.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}
{kind=link}
{kind=link}