


Abstract
Background/Aim: Prognostic factors like the CRP-to-albumin ratio (CAR) represent potential predictors for survival of pancreatic cancer patients. We aimed to investigate the prognostic strength of the CAR for overall survival of patients with pancreatic cancer undergoing pancreatic resection. Patients and Methods: Data from a total of 202 patients with pancreatic adenocarcinoma who had undergone curative pancreatic resection were subjected to a retrospective review. Overall survival was calculated according to the Kaplan–Meier method, and multivariate Cox regression analysis was used for calculating the prognostic strength of CAR. Results: CAR was an independent prognostic factor of overall survival in univariate and multivariate Cox regression analysis. Elevated CAR was associated with a higher median value of Charlson Index, higher Union for International Cancer Control (UICC) classification and increased carcinoembryonic antigen (CEA) levels. Conclusion: CAR is a useful prognostic factor for the prediction of overall survival for patients undergoing pancreatic surgery. The impact of CAR in individual risk assessment should be evaluated in further studies.
Pancreatic cancer represents three to four percent of all malignant tumors, but is responsible for approximately 6% of all cancer-related deaths in Austria. Every year, around 1,500 individuals are diagnosed with pancreatic cancer in Austria (1); pancreatic ductal adenocarcinoma (PDAC) presents in general at a median age of 70 years (2). One of the factors that contributes to this high mortality rate is the fact that most cases are detected in an advanced tumor stage. The factors that contribute to genesis of pancreatic cancer are heredity, lifestyle, smoking, alcohol usage, obesity, diabetes, chronic pancreatitis, and increased use of industrial chemical substances (3-5). Inflammatory processes have been shown to be key mediators of the development and progression of pancreatic cancer (6-8). Furthermore, there is novel evidence that intracellular accumulation in perisinusoidal cells in the liver can lead to activation of carcinogenic development in genetically predisposed individuals (8). Systemic inflammatory reactions play an important role in carcinogenesis and tumor progression (9).
CAR (CRP-to-albumin ratio) is related to tumor-free survival and the overall outcome of cancer patients (10, 11), but its role in patients with pancreatic ductal adenocarcinoma (PDA) undergoing pancreatic resection has been investigated only in a few reports (12, 13). At this point, there is no inflammation-based score predicting outcome in patients with PDAC after surgical resection.
Our main goal was to determine if CAR could represent a useful prognostic factor for the outcome of patients diagnosed with PDAC.
Patients and Methods
This retrospective study was conducted as a single-center-analysis at the division of general surgery of the Medical University of Graz. All data from patients with resectable PDA that underwent pancreatic surgery between January 2000 and December 2016 at our department were included (202 patients). This study included only the patients with diagnosed PDAC. Patients who died within thirty days after tumor resection as well as patients with missing data were excluded from the study (84 patients). Patient selection is shown in Figure 1. TNM categories were taken from the American Joint Committee on Cancer (AJCC) tumor/node/metastasis (TNM) classification and staging system for pancreatic cancer (Eighth Edition 2017). Outcome variables were collected from the patient's medical history and the Austrian national cancer registry.
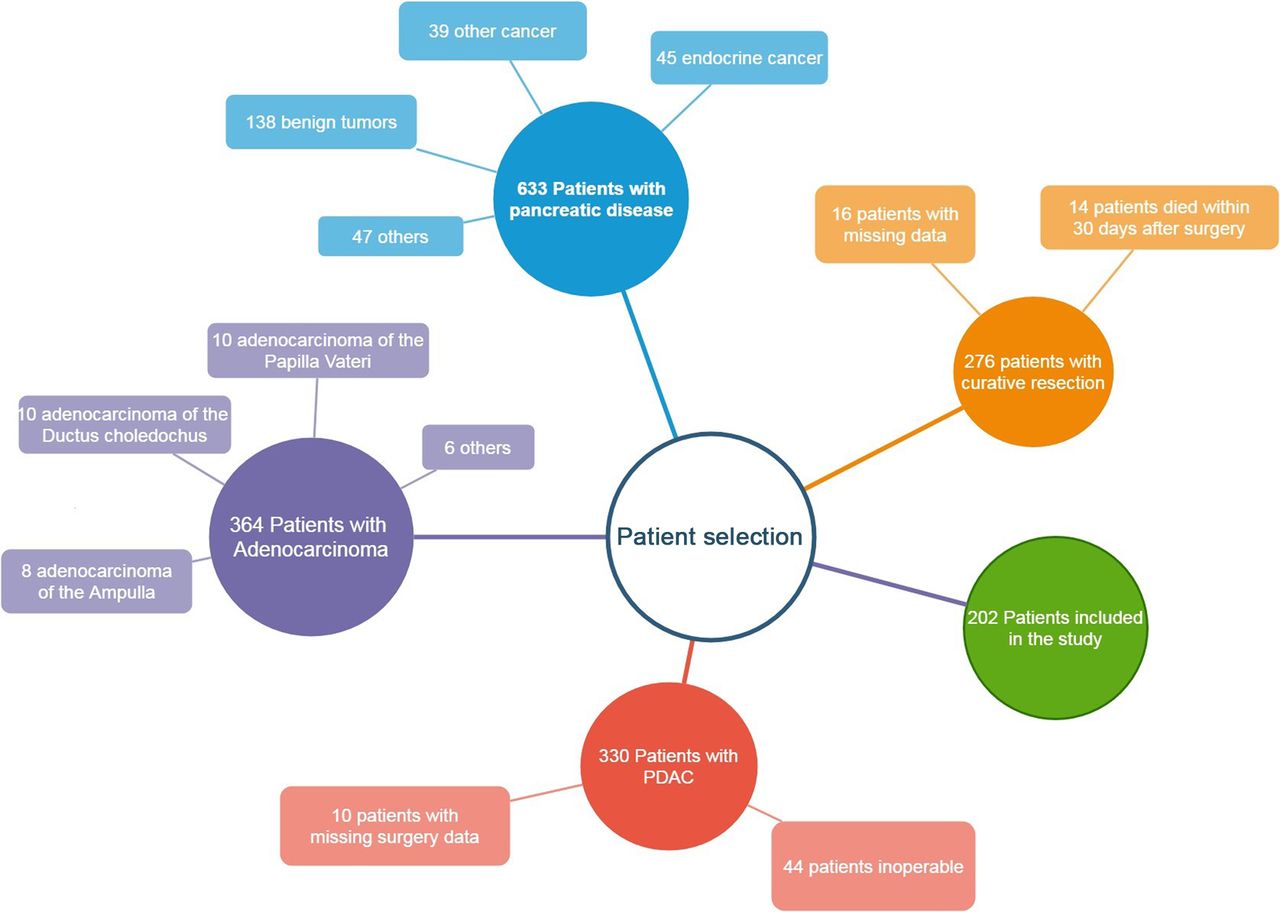
Selection of patients in the study.
The patient collective was categorized by different factors, including ASA category (14) and the Charlson comorbidity index (15).
Data collection. Patient data were retrospectively obtained from the digital clinical database “Medocs”. The data were anonymized and collected in an excel spreadsheet. The following clinical and pathological parameters were obtained: Baseline variables, such as preoperative symptoms, risk factors and comorbidities, preoperative laboratory values, peri-, intra- and postoperative data, histopathologic data as well as follow-up details. The study protocol was approved by the local ethics committee (25-303 ex 12/13).
Statistics. Statistical analysis was performed with SPSS 240 for windows (IBM Inc. Somers, USA). For categorical data, chi square test was conducted, while for numeric data t-test or Mann-Whitney U test were performed as appropriate. Univariate and multivariate analysis was performed using COX regression analysis to assess the influence of the different clinical-pathological parameters on overall survival. A two-sided p<0.05 was considered as statistically significant.
Overall survival as well as tumor-free survival were calculated according to the Kaplan–Meier method.
Results
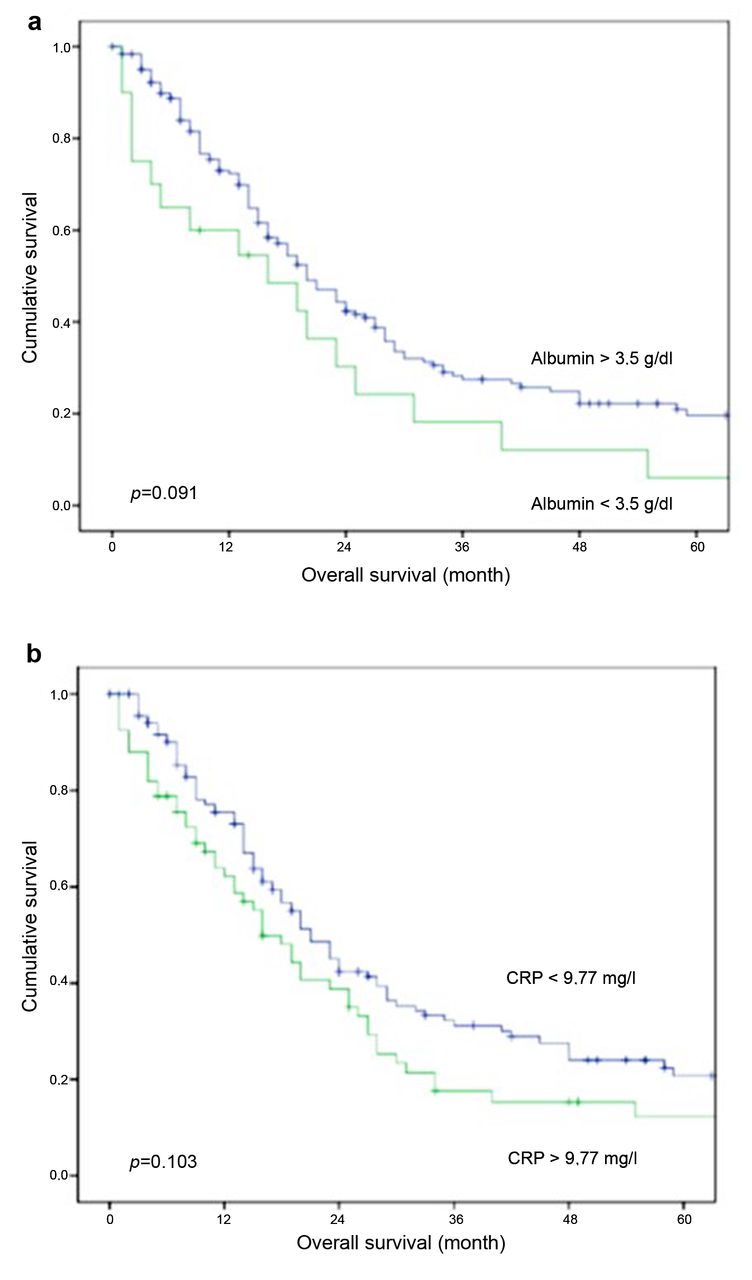
The cut-off value for the CAR for this patient collective was 0.0003. Figure 2 shows the Kaplan–Meier curve for patients with a CAR <0.0003 (blue, 143 patients) vs. patients with a CAR >0.0003 (green, 59 patients). In Figure 3 the Kaplan–Meier curves for increased serum CRP and hypoalbuminemia are shown. The cut-off value of 9.77 mg/l for CRP was obtained with ROC analysis. Compared to CAR, the two factors alone did not show a significant influence on patient's collective overall survival (CRP- p=0.103, albumin p=0.091 for p<0.05).
The mortality figure (Figure 4) shows a significant difference between patients with a CAR<0.0003 and patients with a CAR>0.0003. The one-year survival of patients with a CAR< 0.0003 was 67% while patients with CAR>0.0003 had one-year survival of 56%. The five-year survival of patients with CAR <0.0003 ratio was 7% and that of patients with a CAR >0.0003 was 3%. As shown in Table I, patients with a CAR >0.003 have a significantly shorter overall survival time (15.3 months) compared to patients with a CAR <0.0003 (21.2 months, p=0.021). It was also shown, that patients with a CAR >0.0003 have longer in-hospital stay than patients with a CAR <0.0003 (p=0.019). There was no difference between the two groups regarding age, follow-up time, carbohydrate antigen (CA) 19-9 or CEA.

Cumulative survival in patients with a CAR >0.0003 (green) vs. patients with a CAR <0.0003 (blue). Overall survival time (p=0.032) was significantly lower in patients who had higher CAR.
The occurrence of preoperative symptoms- jaundice and pancreatitis- correlated with a CAR >0.0003. Age>70, female sex, Charlson Index>2, the incidence of morbidity after surgery (operation-related complications), a CA 19-9>37 kIU/l, a higher grading, or distant metastasis were not correlated with CAR >0.0003 (Table II). Table III shows the results of univariate analysis of factors influencing overall survival; metastasis, lymph node involvement and CAR >0.0003 were associated with overall survival. There was no significant difference for serum albumin levels, CRP levels, age, age>70, Sex, R-category, grading, Charlson index, the occurrence of preoperative symptoms, CEA levels or CA 19-9 levels.
Table IV shows the multivariate analysis of M category, higher grading, CAR >0.0003 and the presence of preoperative pancreatitis. It was shown that CAR >0.0003, grading, M category and preoperative pancreatitis were associated with overall survival in multivariate analysis.
Discussion
Although pancreatic cancer represents a non-frequent tumor type comprising around four percent of all cancer cases, it is associated with low long-term survival. Up to now, complete surgical resection of the pancreatic tumor still represents the only curative therapeutic approach, but numerous patients are still diagnosed at a non-resectable tumor stage. After surgical resection, the five-year tumor-free survival is reportedly only 25% (2, 5, 7).
In most cases of pancreatic cancer, one of the most commonly used diagnostic tests for detection, resectability criteria, prognosis and response to therapy of PDA patients are serum levels of CA19-9. Sensitivity of CA19-9 serum levels is low because of false positive results, for example in the presence of biliary stasis. However, it still remains one of the most common prognostic indicators in patients suffering from PDAC (5).
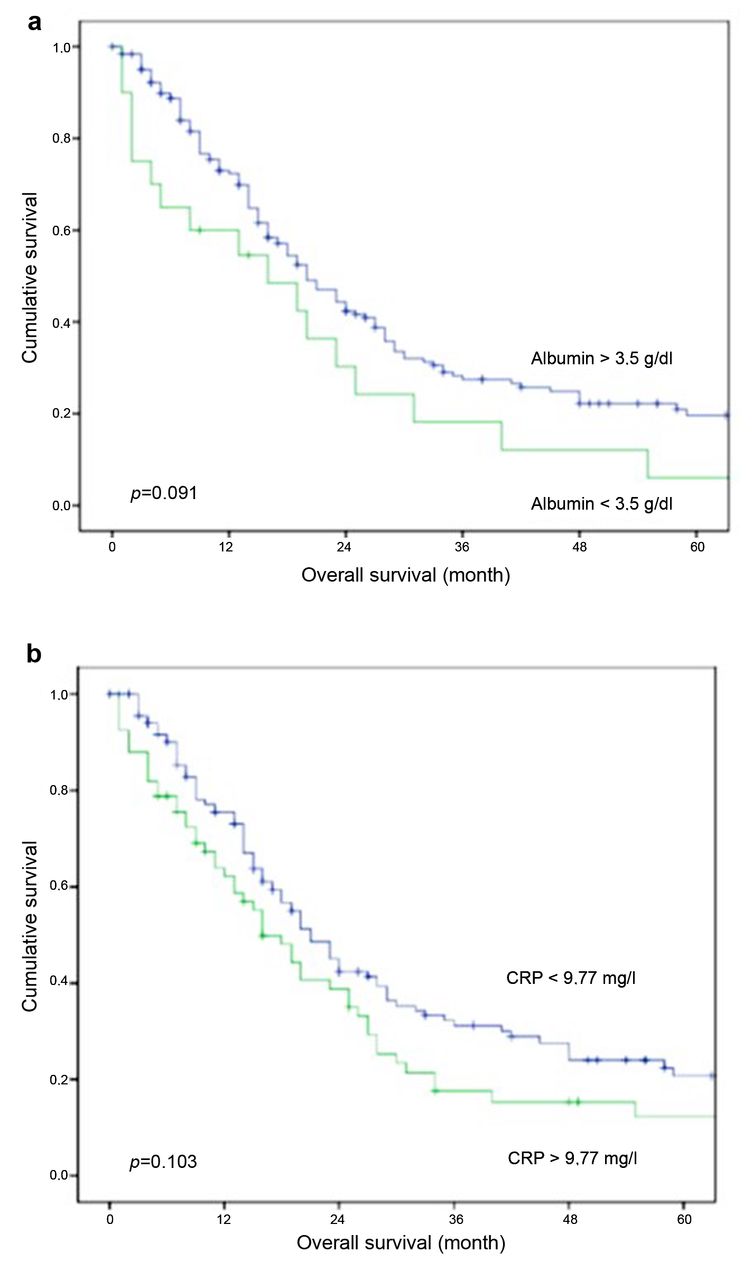
Cumulative survival a) for patients with a serum albumin <3.5 g/dl (green) vs. patients with a serum albumin >3.5 g/dl (blue), p=0.091 b) for patients with a serum CRP >10 (green) vs. patients with a serum CRP <9.77 mg/l, p=0.103. It is shown that the combination of the factors and not each factor alone, shows influence on follow-up time.

Mortality of patients with CAR <0.0003 vs. patients with CAR >0.0003.
We assessed the prognostic value of CAR in patients who had undergone pancreatic resection. CRP is synthesized by hepatocytes and its production is stimulated by pro-inflammatory cytokines, especially interleukin 6. Research states that inflammatory processes within the tumor activate systematic inflammatory pathways which are detectable and could be related to tumor prognosis and outcome (13, 16-27). The CAR has been described as a strong predictive factor for overall survival of other tumor types, such as intrahepatic cholangiocarcinoma, liver, lung and gastric cancer (10, 18, 22, 23). For advanced pancreatic cancer, statistical analysis (17) revealed that the optimal cut-off value for CAR was 0.54; patients with a CAR >0.54 showed an overall shorter survival time (5.0 vs. 2.9 month; p=0.002), which is in line with the results of found by Wu et al. (19).
For patients who underwent curative pancreatic resection, Haruki et al. (12) has proposed an optimal cut-off value of 0.03. Patients with a CAR >0.03 showed a shorter disease-free survival and a decreased survival time in our study population. Compared to Wu et al. (19) and Haruki et al. (12) this cut-off value seems small, but with the correct conversion factor from mg/l (CRP) to g/dl (albumin) and an average CRP of 15.8 mg/dl, the CAR values were comparable. According to Wu et al. and Haruki et al., we could demonstrate that patients with a higher CAR had significantly lower median survival time (21.2 vs. 15.3 months; p=0.021).
Ikuta et al. (13) have reported greater difference in median overall survival time in patients with higher and lower CAR (17.0 months vs. 30.2 months; p=0.01). They also reported that the CAR correlates with poor outcome in cox regression analysis.
Univariate analysis of clinical and pathological parameters in patients with CAR >0.0003 vs. patients with CAR <0.0003.
Univariate analysis (Chi-square test) of clinical and pathological parameters in patients with CAR <0.0003 or CAR >0.0003.
Kaplan–Meier analysis of our cohort, indicated that CRP and albumin alone were not associated with worse outcome (a: p=0.091, b: p=0.103). According to this, serum levels of CRP alone did not correlate with overall survival in univariate Cox regression analysis. Further research is warranted to confirm the hypothesis that CAR is superior to CRP serum levels alone in patients risk stratification. We could show that a CAR>0.0003 was associated with a longer in-hospital stay (11.3 vs. 15.7 days; p=0.019), a higher UICC stage, a Charlson Index >2 and presence of preoperative symptoms, especially jaundice, weight loss and preoperative pancreatitis which are clinical surrogate parameters for advanced disease. Nevertheless, age, gender, tumor stage, tumor localization or CA 19-9 levels were not correlated with elevated CAR levels in uni- and multivariate analysis. In our study, CAR was shown to be statistically significant in both univariate and multivariate analysis. Multivariate analysis showed that patients with a CAR>0.0003, metastasis, preoperative pancreatitis and a higher grade had a poor overall survival.
Univariate analysis of different parameters related to overall survival.
Multivariate analysis (cox regression analysis) of parameters which were significantly correlated with the overall survival time in univariate analysis.
There are limitations and strengths to this study. It holds the known disadvantages of a retrospective single center analysis; nevertheless, our results show a clear association between CAR levels and long-term outcome after pancreatic cancer surgery in our patient cohort.
CAR is an easily available independent predictive factor for survival in patients undergoing curative pancreatic surgery. More extensive research with prospective randomized design is warranted to evaluate the prognostic value of CAR and its optimal cut-off point in patients undergoing pancreatic cancer surgery.
Footnotes
Authors' Contributions
K.P, M.H-J and M.K, J.V conceived and designed the study; K.P., M.H-J, M.K performed the study; W.V and K.P, V.J, M.H-J, M.K. recruited patients, collected and processed samples; and V.J. and W.V. contributed reagents/materials/analysis tools; and V.J, M.K. and K.P. wrote the article. All Authors declare they significantly participated in creation of the study. All Authors read and approved the final article.
This article is freely accessible online.
Conflicts of Interest
The Authors do not have any conflicts of interest to declare regarding this study.
- Received July 23, 2019.
- Revision received September 11, 2019.
- Accepted September 13, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}
{kind=link}
{kind=link}
{kind=link}