


Abstract
Background/Aim: Parathyroidectomy has beneficial effects on all-cause and cardiovascular mortality in patients with uncontrolled hyperparathyroidism. B-Type natriuretic peptide (BNP) correlates with the severity of heart failure. We aimed to investigate whether parathyroidectomy modulates the BNP levels in dialysis patients. Patients and Methods: Patients who underwent surgical intervention for hyperparathyroidism were included. The serum BNP levels were determined before parathyroidectomy and during follow-up. Results: The preoperative and postoperative BNP levels were 499±561 and 453±442 pg/ml, respectively (p=0.82). The baseline BNP level was positively correlated with weakness and headache, but not biochemical parameters. In multivariate analysis, age (odds ratio=0.837) and preoperative symptom score (odds ratio=0.935) were independent predictors for the postoperative decline in BNP levels Conclusion: The serum BNP levels may increase or decrease after parathyroidectomy. Younger age and lower symptom burden are associated with decline in BNP levels.
Secondary hyperparathyroidism develops in patients with chronic kidney disease because of vitamin D deficiency, hypocalcemia, and phosphate retention. Uncontrolled hyperparathyroidism leads to mineral and bone disorder and increased patient mortality (1). For those with secondary hyperparathyroidism refractory to medical treatment, parathyroidectomy has consistently been associated with better survival and improves health-related quality of life (2).
Parathyroid hormone (PTH) has a direct hypertrophic action on cardiomyocytes and can trigger oxidative stress (3). Recently, we demonstrated that serum PTH levels are positively associated with inflammatory markers (4). Furthermore, using the neutrophil–to–lymphocyte ratio as a surrogate marker of inflammation, parathyroidectomy is associated with a decrease in systemic inflammation (5). Of note is the fact that there is a positive association between inflammatory markers and left atrial enlargement among dialysis patients (6). These observations are further supported by the experimental evidence that nephrectomy-induced uremia or high PTH infusion was associated with myocardial hypertrophy and fibrosis, while parathyroidectomy prevented the development of these disorders (7). This may, at least partially, explain the basis of beneficial effects of parathyroidectomy on cardiovascular mortality.
B-Type natriuretic peptide (BNP) is secreted as a pre-pro-hormone from the cardiac ventricles after volume or pressure overload. ProBNP is then further cleaved into the biologically active BNP and the biologically inert N-terminal proBNP. There is a large body of literature that concludes that the level of BNP correlates well with the severity of heart failure (8). However, the impact of parathyroidectomy on the BNP level remains unknown. Thus, the aim of our study was to investigate whether parathyroidectomy modulates the BNP level among dialysis patients with hyperparathyroidism. We also attempted to identify the factors related to change in BNP level.
Patients and Methods
This observational study was conducted in accordance with the Declaration of Helsinki and has been approved by the Institutional Review Board of MacKay Memorial Hospital (18MMHIS131). The study participants were patients with end-stage renal disease on maintenance hemodialysis who were referred for surgical intervention of documented secondary hyperparathyroidism. As per the guidelines of Kidney Disease: Improving Global Outcomes 2017 Clinical Practice Guideline Update (9), intact PTH levels of dialysis patients were managed to keep in the range of approximately two to nine times the upper normal limit. Patients were treated with phosphate binders, vitamin D analogs, and with/without calcimimetics to avoid the progression of PTH levels outside of this range. The indication for parathyroidectomy was severe hyperparathyroidism which did not respond to medical therapy (10).
The patients' hemoglobin, albumin-corrected calcium, phosphate, total alkaline phosphatase, and PTH levels were regularly monitored before surgery and during follow-up. Considering that a small proportion of dialysis patients in Taiwan were taking aluminum-containing phosphate binders, serum aluminum levels were routinely measured in our practice (11). Bone mineral density at the lumbar spine and hip was determined using dual-energy X-ray absorptiometry. Subjective symptoms of patients were evaluated using the Taiwan Chinese version of the parathyroidectomy assessment of symptoms (PAS) questionnaire as previously described (12). The PAS questionnaire consisted of 13 symptoms. The severity of each symptom was measured on a 100-point visual analog scale, and the PAS score was calculated as the sum of all 13 items.
Patients underwent subtotal parathyroidectomy or total parathyroidectomy with or without autotransplantation. After surgery, the serum calcium level was closely monitored. Oral and intravenous calcium with or without oral vitamin D was administered and titrated against the serum calcium level (13). Patients were discharged from the hospital when their serum calcium level was stabilized and the patient was free of symptoms. Phosphate binders were discontinued postoperatively.
In this study, serum BNP concentrations were measured in EDTA-anticoagulated whole blood or plasma specimens using a fluorescence immunoassay (Quidel Triage BNP Test; Quidel Corporation, San Diego, CA, USA) with a coefficient of variation of 10.0%. To characterize the impact of parathyroidectomy on BNP level, the BNP concentration was determined before parathyroidectomy and during follow-up.
Results are expressed as mean±standard deviation or percentages. Given the skewed distribution of most measures, the Wilcoxon signed-rank test and the Mann-Whitney U-test were used for comparisons of continuous variables between paired and unpaired groups, respectively. The nonparametric Spearman rank correlation was used to assess associations. A multivariate regression analysis was carried out to identify independent predictors for the postoperative decline in BNP levels. Variables with p-values below 0.20 in the univariate analysis were included in the multivariable logistic regression analysis. Testing for the goodness of fit was assessed using the Hosmer-Lemeshow test (14). Statistical significance was set at p<0.05. All statistical analyses were performed using Stata 14.0 for Windows (StataCorp, College Station, TX, USA).
Results
Twenty patients who underwent parathyroidectomy from 2016 to 2017 were included in the study for analysis. All patients had been undergoing hemodialysis over a mean period of 10.8±5.2 years. The mean age of our cohort was 59±11 years, 50% of whom were females. Table I shows the baseline characteristics of the patients.
Patient demographics of the study cohort.
Biochemical profile before and after parathyroidectomy in dialysis patients.
Before parathyroidectomy, the mean PTH level of the study cohort was 1,284±261 pg/ml. Serum aluminum levels were generally low. The mean preoperative BNP level was 499±561 pg/ml (median=253 pg/ml; range=39-1,990 pg/ml). Interestingly, the preoperative BNP level was not associated with age, sex, body mass index, the duration of dialysis, or bone mineral density. Nonetheless, the baseline BNP level was positively correlated with the symptoms' ‘weakness’ (Spearman's rho=0.583, p=0.014) and ‘headache’ (Spearman's rho=0.562, p=0.019), but not the overall PAS score (p=0.25). In addition, the preoperative BNP level was not associated with hemoglobin, calcium-phosphate product, alkaline phosphatase, or PTH levels.
Following parathyroidectomy, as expected, calcium, phosphate, alkaline phosphatase, and PTH levels significantly decreased (Table II). The hemoglobin level modestly increased (p=0.018). Consistent with our recent report (5), we observed a significant decrease in the neutrophil-to-lymphocyte ratio during follow-up (p=0.028).
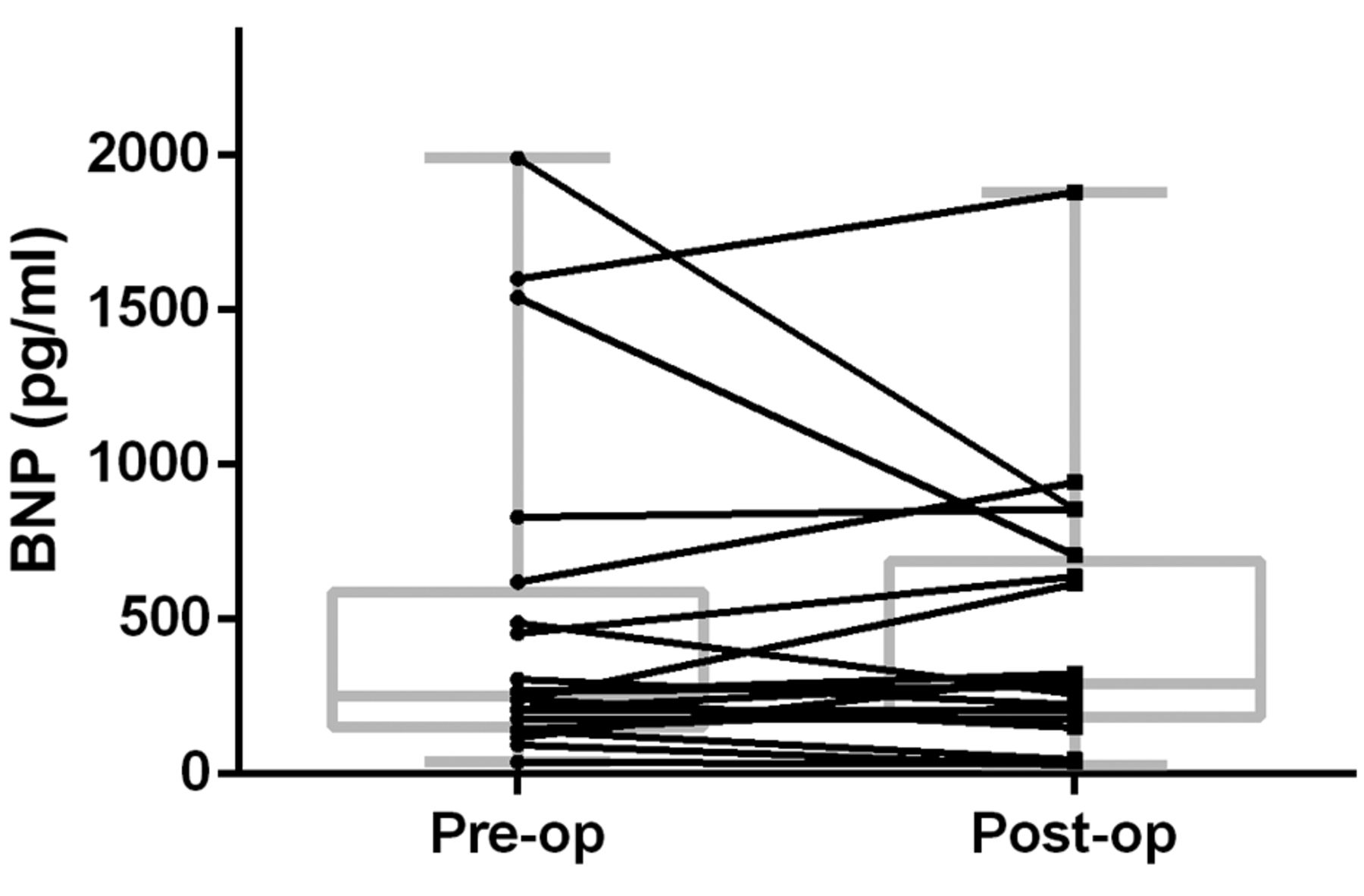
Scatter plot and box plot of serum levels of B-type natriuretic peptide (BNP) before (Pre-op) and after (Post-op) parathyroidectomy.
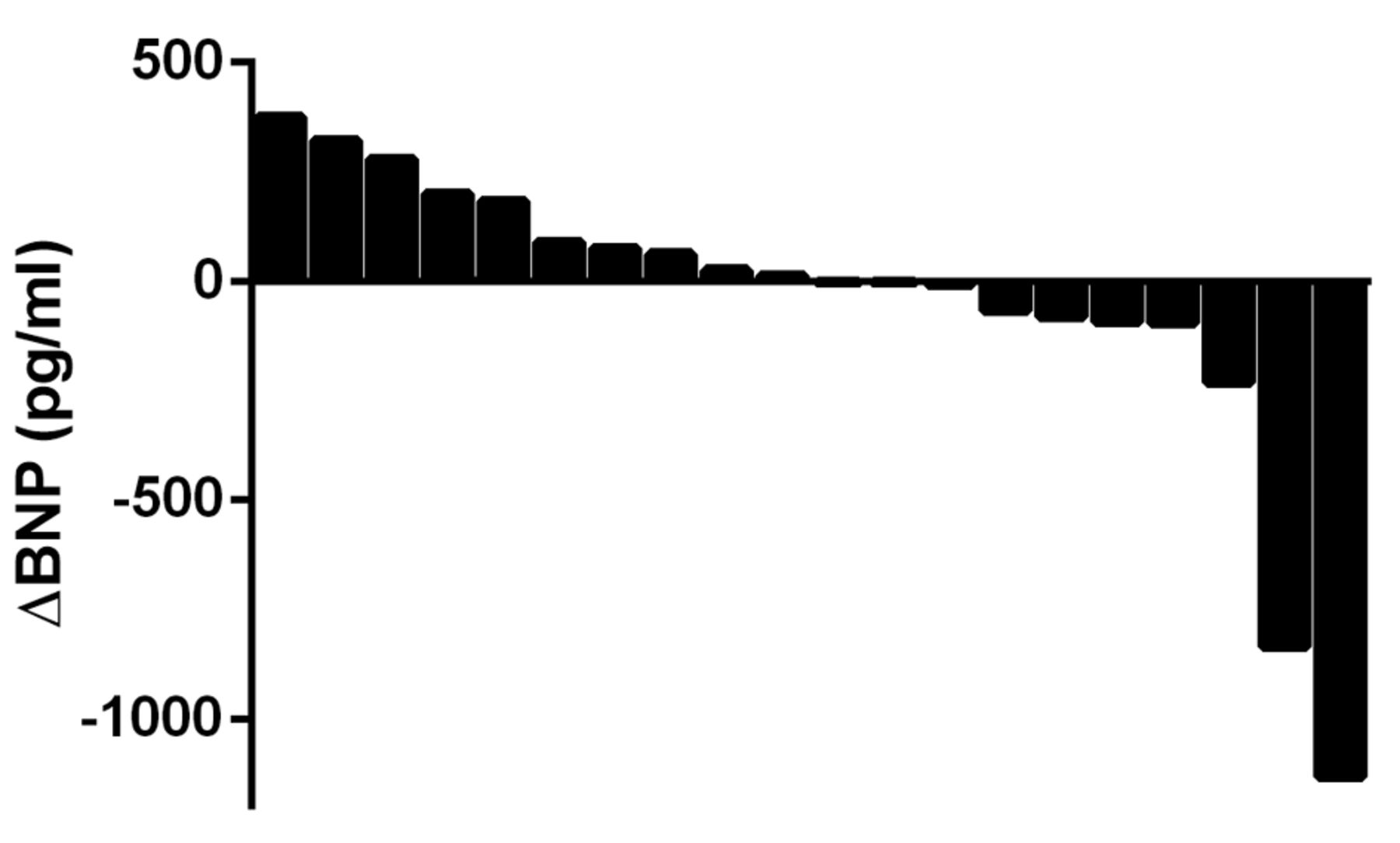
Waterfall plot of the change in serum B-type natriuretic peptide (BNP) level in patients undergoing parathyroidectomy.
The mean BNP level after surgery was 453±442 pg/ml (median=292 pg/ml; range=29-1,880 pg/ml). As shown in Figure 1, the overall BNP level did not significantly change during follow-up (p=0.82). Interestingly, there was a wide variation in the change of BNP level following parathyroidectomy (Figure 2). The mean change in serum BNP level was +9.2% (range=−69.5-170.3%). It is noteworthy that the BNP change following parathyroidectomy was positively correlated with patient age (Spearman's rho=0.495, p=0.026), as illustrated in Figure 3. The BNP change was not associated with sex, body mass index, the duration of dialysis, or other biochemical parameters.
There were seven (35%) patients who had a BNP decline of more than 20% from the baseline value. A multivariate regression analysis indicated that younger age (odds ratio=0.837) and lower preoperative PAS symptom score (odds ratio=0.935) were independent predictors for postoperative decline in BNP level (Table III). The model demonstrates a statistically good fit (Hosmer–Lemeshow goodness-of-fit test p=0.73).

Scatter plot of the percentage change in serum B-type natriuretic peptide (BNP) and patient age in patients undergoing parathyroidectomy.
Discussion
Patients with end-stage renal disease have a high prevalence of cardiac structural and functional abnormalities which are closely associated with age and PTH level (15). In addition, the PTH level is positively associated with myocardial hypertrophy and negatively associated with cardiac systolic and diastolic function (16). A number of studies have shown that parathyroidectomy has beneficial effects on all-cause and cardiovascular mortality in dialysis patients with secondary hyperparathyroidism (2). Specifically, parathyroidectomy improved left ventricular hypertrophy by a significant reduction in left ventricular mass index (17). Japanese researchers demonstrated that the left ventricular ejection fraction was significantly improved after parathyroidectomy in patients with dilated cardiomyopathy caused by secondary hyperparathyroidism (18). Nonetheless, limited data are available concerning the impact of parathyroidectomy on the BNP level.
In hemodialysis patients, the serum BNP levels were determined according to age, left ventricular ejection fraction, and left atrial diameter (19). Notably, the BNP level and its dynamics are strong predictors of all-cause and cardiovascular mortality, and cardiovascular events (19, 20). However, the utility of BNP-guided treatment remains controversial. A recent review suggested that BNP-guided treatment may reduce heart failure admission, but it is uncertain whether BNP-guided treatment is helpful in reducing all-cause mortality or heart failure mortality (21). Despite the limitation on therapy guidance, the BNP level might be exploited as a helpful biochemical marker to assess the heart function in dialysis patients.
Univariate and multivariate logistic regression analysis of variables associated with the decline in serum B-type natriuretic peptide levels following parathyroidectomy.
Very few studies have addressed the effects of parathyroidectomy on BNP level and have had conflicting results. There was a case report on a woman with remarkable improvement in left ventricular contraction after parathyroidectomy (22). Along with the decrease in PTH level, the patient's BNP level dropped from 5,790 to 1,250 pg/ml at 6 months after the operation. On the contrary, a study from Brazil revealed that serum N-terminal proBNP levels significantly increased after parathyroidectomy in spite of improving clinical status (23). The authors proposed that postoperative hypocalcemia might be associated with myocardial dysfunction. In this context, the results of our study confirmed that the magnitude and direction of the change in BNP levels varied substantially. However, we did not find any association between the BNP change and serum calcium level or other biochemical parameters.
The most notable finding of this study was that patient age plays an important role in the effect of parathyroidectomy on the BNP level. Age per se is an independent factor associated with all-cause and cardiovascular mortality in hemodialysis patients (24). For dialysis patients, parathyroid surgery under general anesthesia is not a minor procedure, and the operation is associated with significant morbidity in the immediate postoperative period (25). Large registry studies have shown that although parathyroidectomy is beneficial in long-term survival, it was associated with higher short-term mortality among dialysis patients (26, 27). Importantly, the in-hospital mortality rate was significantly higher in patients with heart failure (28). Therefore, it is imperative to monitor the postoperative electrolyte profile of the patients and tailor appropriate calcium supplementation under close surveillance.
It is possible that the aging process aggravates surgical stress in these dialysis patients, thus resulting in the paradoxical elevation in BNP levels after surgery. An alternative explanation is that aging indeed potentiates hyperparathyroidism-associated complications. Heart failure is a major age-associated cardiac pathology. Calcification of the aortic valve leaflets in old age may impair their movement, obstruct left ventricular outflow, and promote the development of heart failure (29). Vascular and soft tissue calcification is a well-known consequence of uncontrolled hyperparathyroidism. It has been suggested that parathyroidectomy should not be delayed when medical treatment fails because the complications might be irreversible (30). This possibility is also supported by the negative association between BNP decline and preoperative PAS scores. A higher symptom score may reflect a higher severity of hyperparathyroidism, which renders the cardiac function more resistant to surgical intervention.
We recognize some of the limitations of our study. The number of patients was small; statistical power was therefore limited. In addition, the follow-up BNP levels were determined at a single time point. Therefore, a more sophisticated analysis of the dynamics in BNP change was not possible in this study. We did not perform cardiac functional studies in parallel. It is unknown whether the change in BNP level might be translated into more clinically meaningful outcome measures. We believe, however, that this study provides interesting insights into the interaction between hyperparathyroidism, aging, and surgical intervention.
In conclusion, the serum BNP levels may increase or decrease after parathyroidectomy for secondary hyperparathyroidism in dialysis patients. Younger age and lower symptom burden are independent predictors of postoperative decline in the BNP level.
Acknowledgements
This work was supported by research grants from the Ministry of Science and Technology of Taiwan (MOST-106-2314-B-715-008-MY3) and Mackay Medical College (1071B24).
Footnotes
This article is freely accessible online.
Conflicts of Interest
The Authors have no conflicts of interest to declare.
- Received June 22, 2019.
- Revision received July 9, 2019.
- Accepted July 15, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.