


Abstract
Background/Aim: The benefits of gastrectomy for elderly gastric cancer (GC) patients remain unknown. The aim of this study was to evaluate the validity of gastrectomy. Patients and Methods: Patients who had R0 or R1 resection and diagnosed as pathological Stage I-III GC were enrolled in this study. Patients were classified according to age: Elderly group (≥80 years old), non-Elderly group (70-79 years old), Standard group (≤69 years old). Results: As the age raised, the number of comorbidities increased and patients had a worse physical status. Operative procedure and postoperative complications of the Elderly group were similar to that of the non-Elderly group. The overall survival was similar in pathological Stages I and III between the Elderly and non-Elderly groups, while the Stage II Elderly group had shorter overall survival. Also, the Elderly group did not undergo adjuvant chemotherapy compared to other groups. Conclusion: Gastrectomy can be performed safely in elderly patients following gastrectomy, survival of elderly patients was similar to non-elderly patients. Therefore, gastrectomy is an acceptable treatment for elderly patients in good condition.
The incidence of Gatric cancer has declined over the past decades (1); however, it is still one of the most common cancers worldwide (2). Gastrectomy is the main treatment for gastric cancer, but it might associate with severe postoperative gastrointestinal symptoms. Previous reports have shown that postoperative morbidity leads to poor prognosis, especially in elderly patients (3, 4).
Aging is accompanied by a decline in the function of critical organs (5, 6). Postoperative morbidity and mortality increases as the age increases. Moreover, elderly patients often have several comorbidities at the time of diagnosis that sometimes affect survival (7, 8). Therefore, it is difficult to predict surgical risk, since physical status varies greatly among elderly individuals.
The rate of gastrectomy in the elderly is increasing (9). Previous articles have shown that gastrectomy can be performed safely in elderly patients as in non-elderly patients (10, 11). However, following gastrectomy, pneumonia often develops leading to death of elderly patients (12). Also, elderly patients are likely to develop malnutrition (13). Therefore, it is still unclear whether gastrectomy improves the overall survival of elderly patients. The aim of this study was to evaluate whether gastrectomy is beneficial for elderly gastric cancer patients.
Patients and Methods
Study design. A single institutional retrospective cohort study was performed at the Kita-Harima Medical Center Hospital from January 2014 to December 2017. All patients who had R0 or R1 resection and diagnosed as pathological Stage I-III were enrolled into this study. Since younger patients tend to have less comorbidities and a better physical status, those under 70 years were considered as standard controls. We defined those over 80 years old as the Elderly group and those between 70-79 years old as the non-Elderly group.
Clinical characteristics, surgical outcomes, pathological findings and follow-up data were extracted from medical records. Physical status was assessed based on the following factors: age, gender, American Society of Anesthesiologists (ASA) score, Charlson comorbidity index (CCI), body mass index (BMI), and modified Glasgow Prognostic score (mGPS). Tumor status was diagnosed according to the Japanese Gastric Cancer Association classification system (14). Operative complications were graded according to the Clavien-Dindo classification and complications higher than grade II were defined as post-operative complications (15). The study design was approved by the ethics review board at Kita-Harima Medical Center and conforms to the provisions of the 1995 Declaration of Helsinki.
Patient characteristics.
Statistical analysis. The difference between two groups was analyzed by using the Fisher's exact test or Chi-square test and Student's T test or Mann–Whitney U-test. Cumulative survival rate was calculated by the Kaplan–Meier method, and survival curves were compared using the log-rank test. In all analyses, a p<0.05 was accepted as statistically significant. Descriptive statistics were obtained using the SPSS 24.0 for Windows (SPSS Inc., Chicago, IL, USA).
Results
One hundred ninety-five patients were enrolled into this study. Among them, 78 patients (40.0%) were under 70 years old, 78 patients (40.0%) were aged between 70-79 years old, and 39 patients (20.0%) were over 80 years old.
The patients' characteristics are listed in Table I. ASA score ≥ 2 was significantly more frequently observed as the age raised (p<0.001). Also, albumin levels decreased and C-reactive protein (CRP) levels increased with age (p<0.001 and p=0.017, respectively). Moreover, higher mGPS was more frequently observed with increasing age (p=0.024). Estimated glomerular filtration rate (eGFR) decreased with age (p=0.002), despite the absence of difference in creatinine levels. CCI increased with age (p=0.003). There was no significant difference in other factors.
The surgical outcomes are listed in Table II. The operation time did not differ between groups (p=0.159). Blood loss was more often observed at older ages (p=0.021). There were no differences in laparoscopic surgery rate, operative procedure, lymph node dissection, and R0 resection rate. Moreover, there were no differences in leakage, pancreatic fistula, and respiratory complications. The Elderly group had a tendency to have a longer length of hospital stay than other groups; however, the difference was not significant.
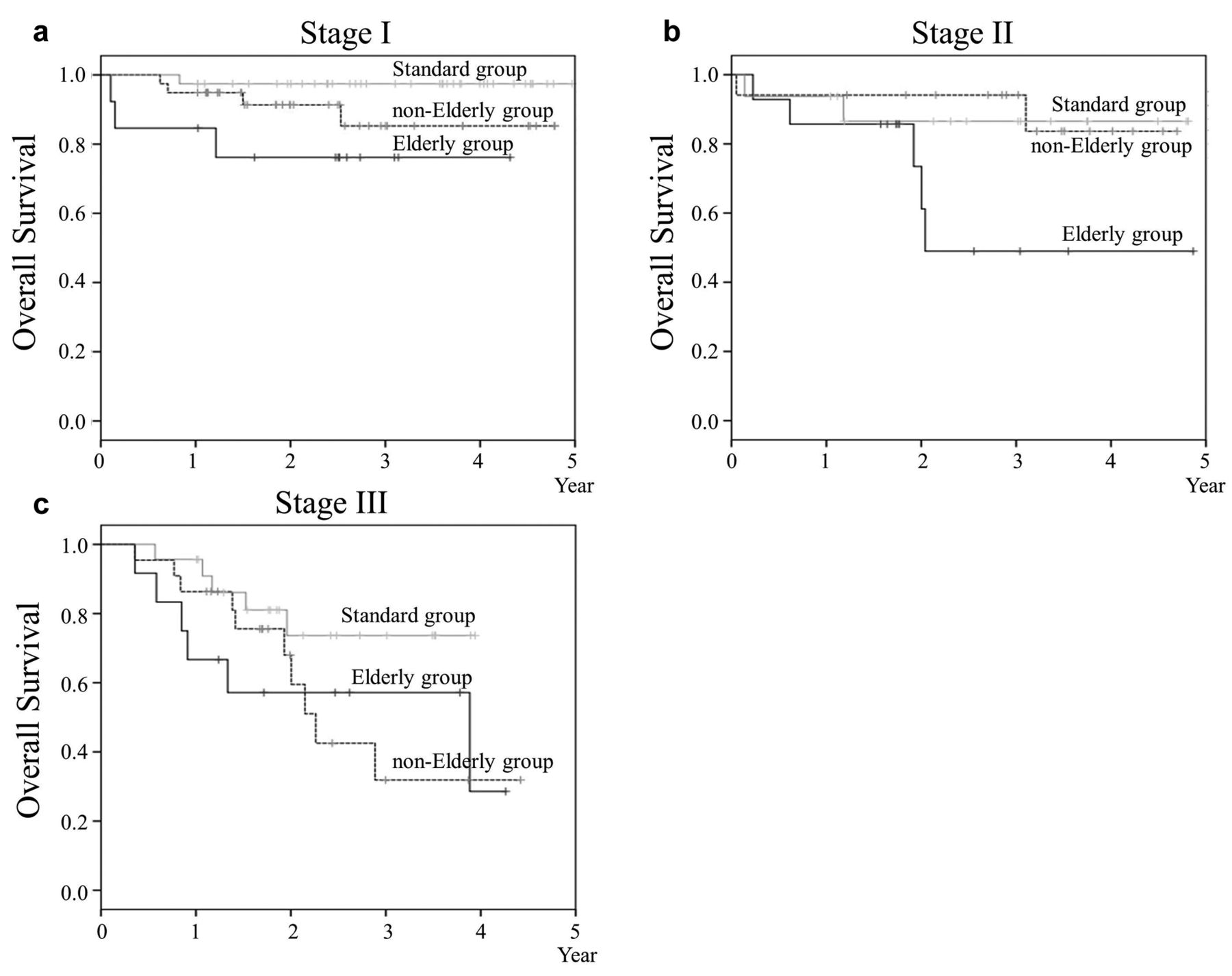
Overall survival (OS) and Cancer specific survival (CSS) of each pathological Stage are shown in Figures 1 and 2. The standard group had the longest overall survival in either Stage. For the OS of pathological Stage I, the Elderly group had the worst survival rate compared to other groups. However, the survival rate between Elderly group and non-Elderly group was not significantly different (p=0.237). Moreover, none of the patients died of cancer in pathological Stage I in either group. Regarding OS in pathological Stage II, the Elderly group had a lower survival rate compared to standard and non-Elderly groups (p=0.113 and p=0.038, respectively). On the other hand, the OS was similar between standard and non-Elderly groups. Similar result was observed for CSS in pathological Stage II. Regarding the OS and CSS of pathological Stage III, survival was similar between Elderly and non-Elderly groups. Among patients who were diagnosed as pathological Stage II or III, the patients who had adjuvant chemotherapy decreased with age (p<0.001, Table III). A similar trend was observed in pathological Stage II and III.
Discussion
Our results showed that gastrectomy can be performed safely in elderly without increasing the postoperative complications. Also, the survival rate in pathological I and III was similar between Elderly and non-Elderly groups. There are previous studies that have compared elderly and non-elderly; however, these studies classified the patients only into two groups (10, 11, 16). Since, younger patients have less comorbidities and longer expectancy than elderly, fine classification of patients is needed to compare the surgical short- and long-term outcomes, as in our study.
Postoperative outcomes.
Numbers of patients who had adjuvant chemotherapy in pathological Stage II and III.
The JCOG0703 study in which the majority of the patients were pathological Stage I, has shown that no patients had recurrent disease and the 5-year OS and RFS were both 98.2% (17). Although, in that study the median age was 59 years old, a similar result was obtained in the current study: no patients had recurrent disease in pathological Stage I. Also, there was no difference in OS, RFS, and CSS between Elderly and non-Elderly groups in pathological Stage III. This might be due to reduced effectiveness of S-1 in pathological Stage III, in contrast to a clear survival benefit in pathological Stage II (18, 19). Also, in that study, the benefit of S-1 was more significant in younger age than in older age. Therefore, the benefit of S-1 may be limited to patients over 80 years old in pathological Stage III.
Despite the fact that survival was similar between Elderly and non-Elderly groups in pathological stage I and III, the Elderly group had worse survival in pathological Stage II than the non-Elderly group. One possible reason might be the low rate of adjuvant chemotherapy. Patients tend to refuse adjuvant chemotherapy with increasing age. Also, we tend not to recommend adjuvant chemotherapy, since the effectiveness of performing adjuvant chemotherapy in elderly patients is unknown and aging itself is a risk factor for poor compliance with adjuvant chemotherapy (20). Therefore, a randomized control study is being carried out by the Japan Clinical Oncology Group to clarify whether adjuvant chemotherapy contributes to improvement of RFS in patients with pathological Stage II/III gastric cancer (21).
There are several limitations to this study. First, this is a retrospective cohort study conducted in a single institution and the sample size was small. Also, since our institution was founded in October 2013, the observation time was quite short which might have contributed to an overestimation of our results. Second, the patients were classified according to the pathological Stage not the clinical stage. Third, the survival of elderly was compared with that of non-elderly patients, since no data were available for the elderly patients not having gastrectomy. However, Endo et al. have shown that gastrectomy improved survival compared to best supportive care for patients above 85 years old (22). Last, there was a tendency to operate elderly patients in good condition.
In conclusion, gastrectomy in elderly patients over 80 years old can be performed safely and survival rate was similar to those of 70-79 years old. Therefore, performing gastrectomy is beneficial for elderly patients in good conditions.

Overall survival of each pathological stage. (a) Elderly group had the worst survival compared to other groups in pathological Stage I; however, the difference was not statistically significant. (b) Elderly group had a lower survival compared to other groups in pathological Stage II. (c) The survival was similar between Elderly and non-Elderly groups in pathological Stage III.
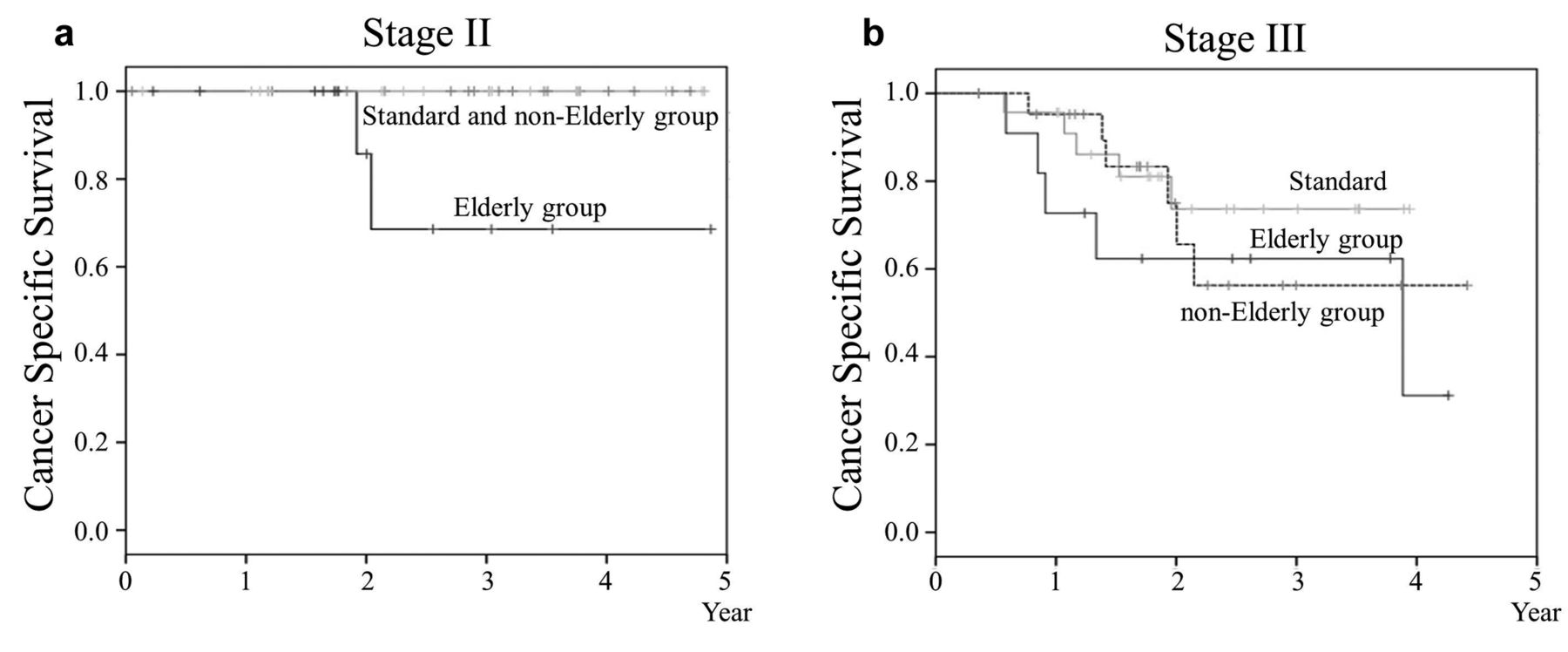
Cancer-specific survival of each pathological stage. (a) The Elderly group had a lower survival compared to other groups in pathological Stage II. (b) The survival was similar between Elderly and non-Elderly groups in pathological Stage III.
Footnotes
Authors' Contributions
YO and KM conceived the study. SO, RF, and KA collected the data. YO, YM, and KK performed the data analysis. YO wrote the manuscript and SO and DK revised the manuscript. All Authors performed the operation. All Authors approved the final version of the article.
This article is freely accessible online.
Conflicts of Interest
The Authors have no conflicts of interest to declare.
- Received March 20, 2019.
- Revision received April 23, 2019.
- Accepted April 24, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}
{kind=link}