


Abstract
Background/Aim: The aim of this retrospective cohort study was to investigate the association between renal dysfunction (RD) and the development of oral mucositis (OM) in patients undergoing concurrent chemoradiotherapy (CCRT) for pharyngeal cancer including radiation to the oral cavity. Patients and Methods: Of 130 patients diagnosed as having pharyngeal cancer who received CCRT at the Okayama University Hospital Head and Neck Cancer Center, 44 were finally selected. Results: During the observation period, 24 (54.5%) patients experienced severe OM (grade 3). The Cox proportional hazards regression model demonstrated that RD (hazard ratio(HR)=2.45, 95% confidence interval(CI)=1.067-6.116, p=0.035) and nasopharynx/oropharynx as center of the irradiated area (HR=2.56, 95% CI=1.072-5.604, p=0.034) were significantly associated with the incidence of severe OM (grade 3). Conclusion: In patients with pharyngeal cancer treated with CCRT including radiation to the oral cavity, RD at baseline can be a risk factor for developing severe OM.
In Japan in 2009, the number of patients with head and neck cancer (HNC) was estimated to be about 19,000, and approximately 3,300 patients died due to HNC (1). In order to reduce mortality, concurrent chemoradiotherapy (CCRT), which was found to be superior to radiotherapy with respect to progression-free survival, has been widely adopted as the standard non-surgical approach in HNC (2-4). However, since CCRT for HNC often uses a platinum-based regimen (5), CCRT induces side-effects including mucositis, xerostomia, oropharyngeal candidiasis, and neurosensory disorders (mucosal pain and taste dysfunction) (6). In particular, oral mucositis (OM) clearly has an adverse impact on patients' quality of life because of pain, i.e. difficulty in eating, swallowing and talking (7,8). Furthermore, severe OM interrupts the cancer treatment course, induces weight loss, and increases the treatment cost (9-12). Thus, the control of OM in cancer treatment is very important.
The risk factors for developing OM during cancer treatment are not fully understood. Risk factors have been attributed to both the therapy regimen and patient characteristics (13). However, even though diagnosis and treatment may be similar, patients are not at equal risk of mucositis (14). Patient-related risk factors can be complex, including systemic conditions.
Among systemic conditions, renal dysfunction (RD) is one of the basic conditions that should be carefully considered in patients with cancer, and drug dosage adjustments are often necessary in CCRT. Although RD affects the metabolism of anticancer agents (15), the association between RD and OM development during cancer treatment such as CCRT remains unclear. Thus, we hypothesized that RD is a risk factor for developing OM in CCRT. The aim of this study was to investigate the association between RD and OM in patients undergoing CCRT for pharyngeal cancer including radiation to the oral cavity. Because the area irradiated in patients with pharyngeal cancer often includes the oral cavity, the inclusion criteria of this study were pharyngeal cancer and treatment with CCRT.
Patients and Methods
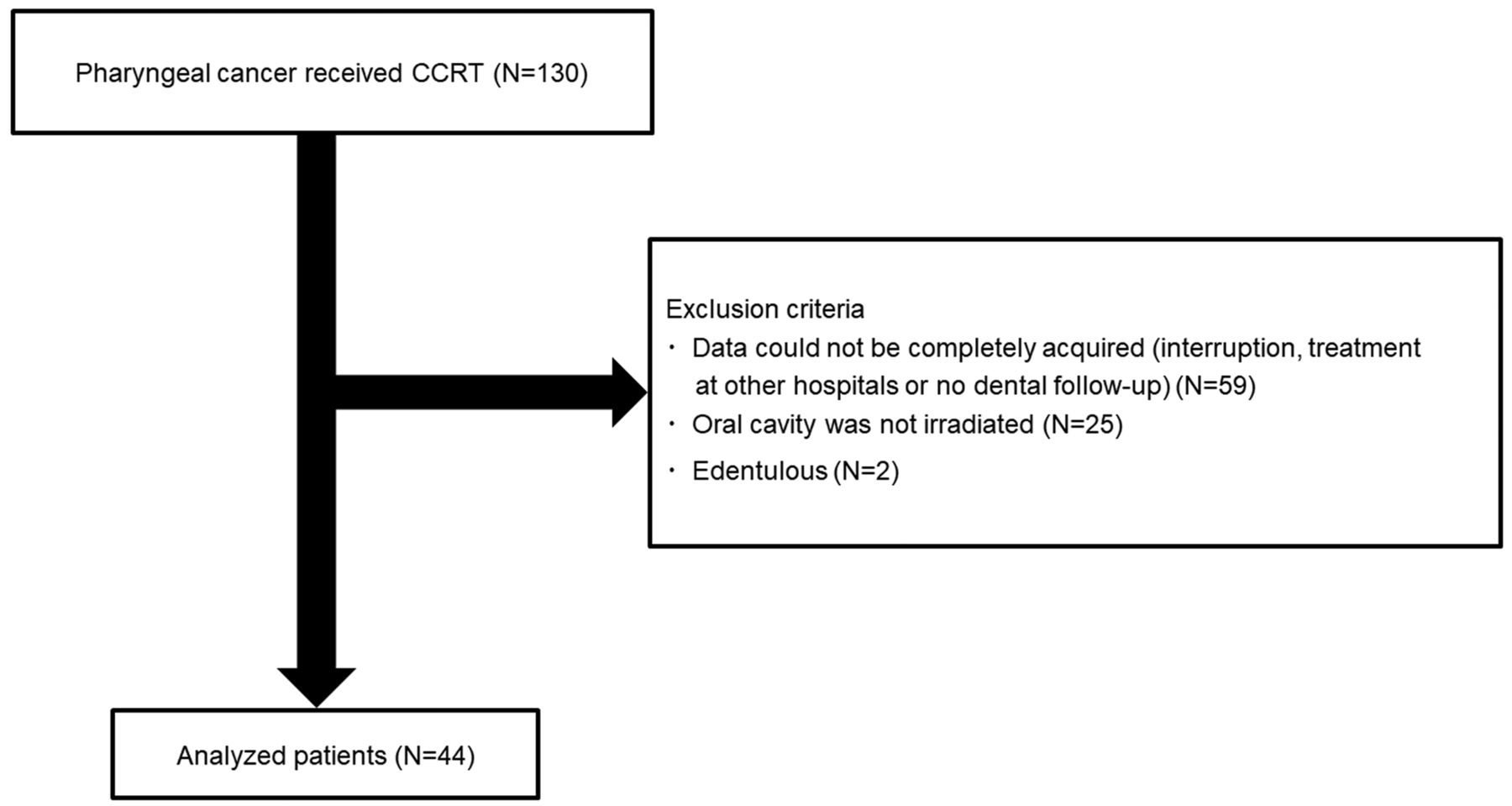
Study design and population. This was a retrospective cohort study. A total of 130 patients were diagnosed as having pharyngeal cancer at the Okayama University Hospital Head and Neck Cancer Center (Okayama, Japan) and received CCRT between April, 2013 and March, 2017. Exclusion criteria were as follows: complete data not acquired (59 patients); irradiated area did not include the oral cavity (25 patients); or edentulous patients (two patients). As a result, data from 44 patients were analyzed (Figure 1).
This study was approved by the Ethics Committee of the Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences and the Okayama University Hospital (no. 1802-018). Informed consent was obtained from each participant.
General and oral conditions. The data for the general and oral conditions were collected from medical and dental records. These items were age, sex, body weight, smoking habit, drinking habit, medical history, radiation dose, anticancer agent menu, cancer stage (International Classification of Diseases for Oncology ICD-10 version 2015) (16), primary cancer site, center site of the irradiated area, incipient or recurrent cancer, number of teeth present, possible oral factors causing injury to the oral mucosa, nutrition by gastrogavage/nasoenteric, xerostomia, and amount of anti-inflammatory gargle agent used. Factors causing injury to the oral mucosa, such as malalignment and remaining tooth roots, were diagnosed by a dentist prior to cancer therapy. Furthermore, serum markers, including white blood cell (WBC) count, serum albumin, serum creatinine, aspartate aminotransferase (AST), alanine aminotransferase (ALT), and C-reactive protein (CRP), were also evaluated. The serum WBC count was determined by the electrical resistance method using an automatic analyzer (BAYER ADVIA2120; Bayer Ltd., Osaka, Japan). The serum Alb level was measured by the modified bromocresol purple method using an automatic analyzer (JEOL BM 8040 and BM 2250; Jeol Ltd., Tokyo, Japan). The serum creatinine level was measured by enzymatic methods using an automatic analyzer (JEOL BM 8040 and JCA-BM 6050; Jeol Ltd.). The serum CRP concentration was measured using the latex agglutination method using an automatic analyzer (JEOL BM 8040 and BM 2250; Jeol Ltd.).
The serum creatinine level (SCr) was converted to creatinine clearance (Ccr) in males by the Cockcroft-Gault equation (17,18), as follows:

For females, Ccr values thus calculated were multiplied by 0.85. Based on previous studies (19-23), a Ccr cut-off of 60 ml/min was used. Ccr of 60 mI/min or less was defined as moderate/severe RD, and Ccr of 60 mI/min or more was defined as normal/mild RD.
The scale for OM was according to the Common Terminology Criteria for Adverse Events ver. 3.0 (2006) (24) as follows: 0, None; 1, erythema of the mucosa; 2, patchy ulcerations or pseudomembranes; 3, confluent ulcerations or pseudomembranes, bleeding with minor trauma; 4, tissue necrosis, significant spontaneous bleeding, life-threatening consequences; and 5, death. Treatment plans were determined by standard protocols according to the tumor stage and physical condition of the patient.
Statistical analysis. The patients were divided into two groups according to OM: grade 0-2 (N=20) and grade 3 (N=24); there were no patients with grade 4 or 5 during the study period. The Mann–Whitney U-test and chi-squared test were used to assess significant differences in clinical variables between the two groups. The cumulative incidence of overall OM was estimated using the Kaplan–Meier method, and differences were tested using the log-rank test. The follow-up period lasted until a CCRT dose of 60 Gy was reached.
Backward stepwise regression procedures for the Cox proportional hazards model were used to determine significant prognostic factors. The variable reduction method (likelihood ratio) was adopted for the Cox proportional hazards model, and the remaining factors were re-evaluated using the forced-input method. In the Cox proportional hazards model, the following candidate variables were adjusted for covariates: Smoking habit, drinking habit, incipient cancer, cancer stage, toxicity of anticancer drug agents, number of teeth present, factor causing injury to the oral mucosa, WBC count, serum albumin concentration, center of the irradiated area, and renal dysfunction. Anticancer agents were divided into two categories according to toxicity, either liver or kidney. Values of p<0.05 were considered significant. All analyses were performed using SPSS 15.0 J for Windows (IBM Japan, Tokyo, Japan).
Results
Table I shows the comparisons of baseline variables and events in CCRT between the two OM groups, grade 0-2 and grade 3. There were no significant differences in the variables between the two groups, except for Ccr, which was significantly lower in the latter group.
Table II shows the distribution of OM during the CCRT period in the normal/mild RD and the moderate/severe RD groups. There were no significant differences in the distribution of severity between the two groups.
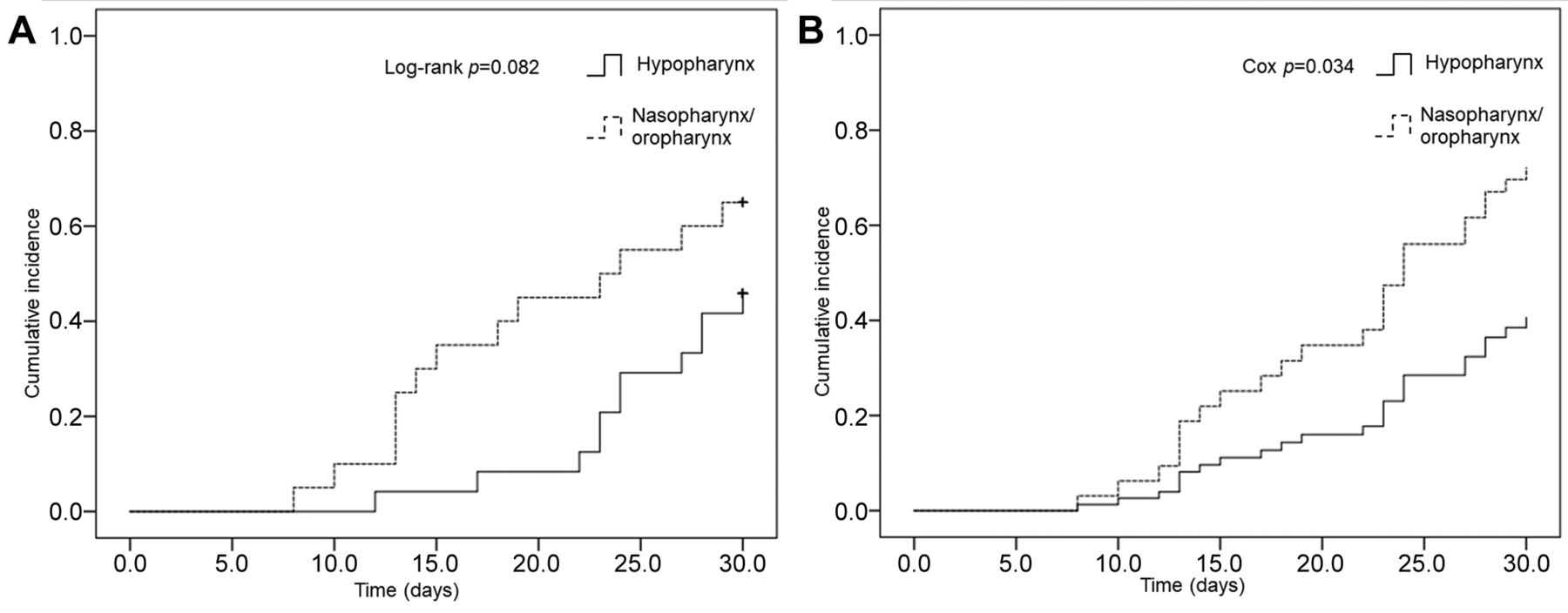
The Cox proportional hazards regression model demonstrated that the nasopharynx/oropharynx as the site of the irradiated area and RD were significantly associated with the incidence of severe OM (grade 3) (Table III). Figure 2 shows the association between RD and the overall incidence of severe OM for non-adjusted and adjusted cases. Figure 3 shows the association between the site of the irradiated area (hypopharynx vs. nasopharynx/oropharynx) and the overall incidence of severe OM for non-adjusted and adjusted cases.
Discussion
As well as type of CCRT, a variety of factors including age, nutritional status, type of malignancy, pretreatment oral condition, oral care during treatment, and pretreatment neutrophil counts can be associated with the development of OM in patients with HNC (25, 26). However, the details of the mechanism of OM development are completely unknown, and its control during CCRT remains challenging. To the best of our knowledge, this is the first longitudinal study to investigate the association between OM and RD during CCRT. The present study showed that the relative high-risk factors for severe OM (grade 3) were the nasopharynx/oropharynx as site of irradiation and RD (Table III). This may provide a new insight into OM and predict developing OM during CCRT by focusing on RD.
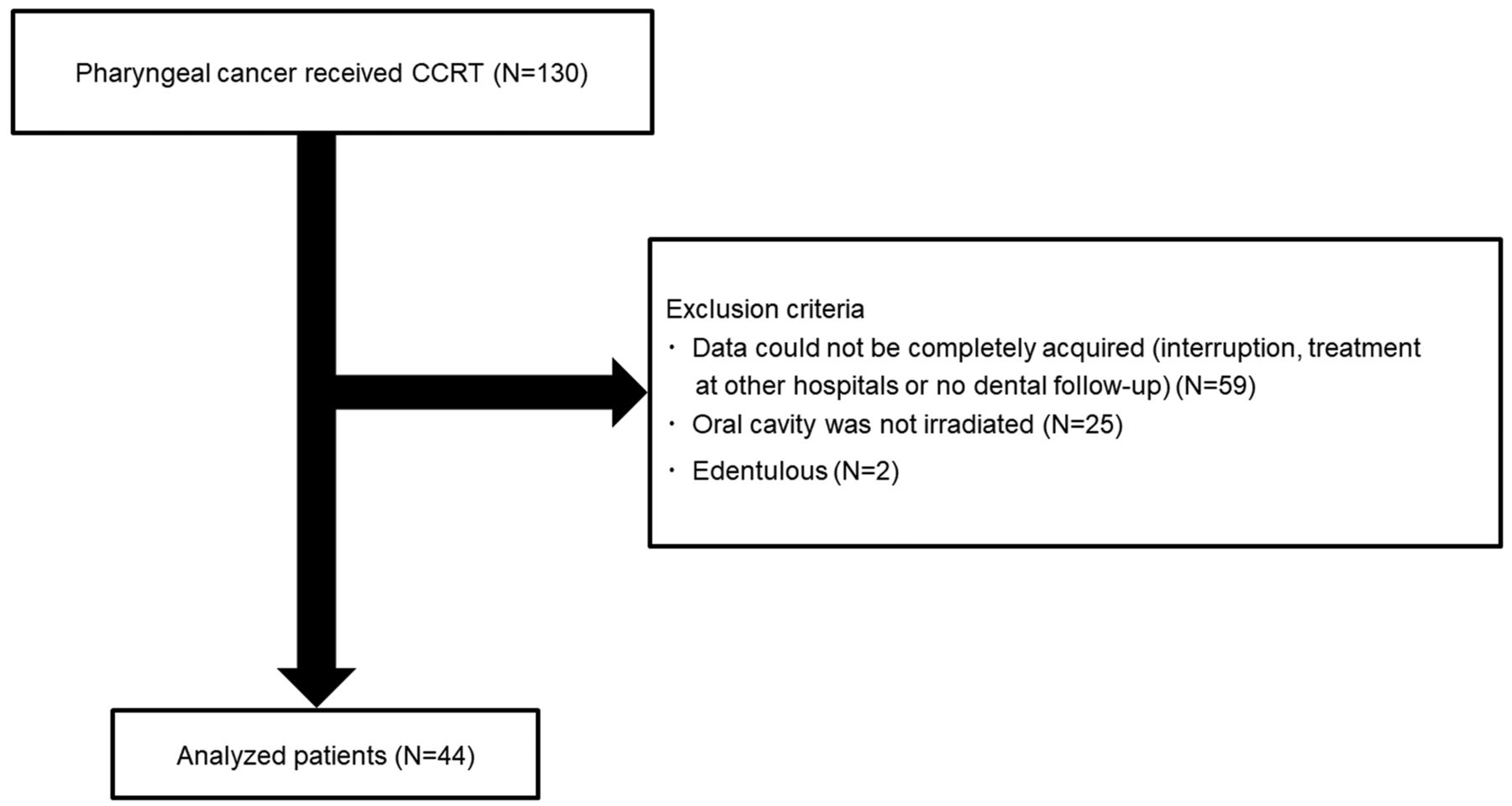
Flowchart of the study. CCRT: Concurrent chemoradiotherapy.
It was found that RD was a possible risk factor for severe OM (Table III). Since impaired renal function is associated with decreased renal clearance of drugs, it can lead to high incidences and severities of adverse events in patients taking anticancer agents (22). In CCRT, anticancer agents or molecular target drugs, including cisplatin, carboplatin, methotrexate, tegafur, and cetuximab, are widely used. One of the major side-effects of these anticancer agents is RD (14). Therefore, prescription of anticancer agents should be carefully considered in order to prevent severe OM in patients with HNC during CCRT in accordance with the estimated Ccr.
When the center of the irradiated area was the nasopharynx/oropharynx, the risk of severe OM was significantly higher than when it was the hypopharynx (Table III, Figure 3). The radiation dose is gradually attenuated from the center of the target lesion to the neighboring area (27). Since the center of the irradiated area was closer to the oral cavity when the site was the nasopharynx/oropharynx rather than the hypopharynx, it may be reasonable that severe OM developed in cases with the center site being the nasopharynx/oropharynx.
Because of intense pain, patients with grade 3-4 mucositis require feeding tubes, total parenteral nutrition, and opioid analgesics (12, 28). Therefore, clinicians should pay attention to nutritional support, oral decontamination, palliation of dry mouth, management of oral bleeding, and therapeutic interventions during the management of OM in patients treated with CCRT (29). In the present study, all patients received continuous oral hygiene care by nurses, dentists, or dental hygienists. When patients have RD and the center site of the irradiated area is the nasopharynx/oropharynx, clinicians should understand the high risk of severe OM before CCRT. Furthermore, more appropriate management of OM is needed in the future.
CCRT is one of the most commonly used cancer treatments, in which severe OM develops at a high rate. CCRT can more easily induce severe OM than radiotherapy alone. Furthermore, the risk of severe OM in radiotherapy without covering the oral cavity, such as intensity-modulated radiation therapy, may be similar to that of chemotherapy alone (27). Since the goal was to investigate more critically the risk of OM in CCRT, CCRT cases in which the irradiated area did not cover the oral cavity were excluded.
Relationships between grade of oral mucositis and other factors.
Relationship between renal dysfunction (RD) and oral mucositis (OM).

Association between renal dysfunction and overall incidence of oral mucositis (grade 3) for non-adjusted (A) and adjusted (B) cases (adjusted for covariates shown in Table III). Moderate/severe renal function: Creatinine clearance (Ccr) <60 mI/min; normal/mild renal dysfunction: Ccr≥60 mI/min.

Association between the center site of the irradiated area (hypopharynx vs. nasopharynx/oropharynx) and the overall incidence of oral mucositis (grade 3) for non-adjusted (A) and adjusted (B) cases (adjusted for covariates shown in Table III).
Cox proportional hazards model examining prognostic factors.
A previous study reported that the overall incidence of OM in CCRT was 80% (30). For severe OM (>grade 2), the incidence was about 45% in patients receiving CCRT (10, 25, 26). In the present study, the overall OM incidence was 95.5%, and severe OM was observed in 54.5% of patients (Table II). On the other hand, in patients receiving a typical course of RT (6-7 weeks), OM appears as erythema of the oral mucosa in the first 2-3 weeks of RT. In the present study, OM appeared 2-3 weeks after the start of CCRT (data not shown). Thus, the prevalence and timing of developing OM in this study were similar to other studies.
The present study had certain limitations. Firstly, all patients were recruited from the Okayama University Hospital. This may limit the application of our findings to the general population. Secondly, the number of patients was small. Further studies with a larger number of patients are required. Thirdly, this was a retrospective cohort study. Prospective cohort or intervention studies may confirm this relationship. Finally, aIthough there was adjustment for potential confounders, there may be further confounders including oral microflora or genetic factors, and the detailed mechanism relating RD and OM remains unknown.
In conclusion, this retrospective study showed that RD at baseline and nasopharynx/oropharynx as the center of the irradiated area were associated with a high risk of severe OM in patients with pharyngeal cancer those with CCRT including irradiation to the oral cavity.
Footnotes
This article is freely accessible online.
Conflicts of Interest
The Authors declare they have no competing interests in regard to this study.
- Received August 26, 2018.
- Revision received September 21, 2018.
- Accepted September 28, 2018.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.