


Abstract
Background/Aim: The number of elderly patients diagnosed with hepatocellular carcinoma (HCC) has been increasing. But there is no proper management based on age stratification in elderly patients. Therefore, we evaluated the clinical characteristics and outcomes of elderly HCC patients more than 75 years old in South Korea. Patients and Methods: Five hundred and fifty elderly patients with HCC were enrolled and divided into the oldest-old (age ≥85 years), middle-old (age between 80 and 85 years), and young-old groups (age between 75 and 80 years). Results: Fifty-one, 153, and 346 patients were included in the oldest-old (mean age: 87 years), middle-old (mean age: 82 years), and young-old groups (mean age: 77 years), respectively. There was a significantly lower rate of alcohol-related and hepatitis B virus-related diseases in the oldest-old group than in the other groups, whereas there was no significant difference in other characteristics. With increasing age, conservative treatment was predominantly performed. Transarterial chemoembolization was the main modality of active treatment in all groups. In multivariate analysis, the performance score, model for end-stage liver disease score, modified Union for International Cancer Control staging, Barcelona Clinic Liver Cancer staging, presence of portal vein tumor thrombosis, ruptured HCC, and active treatment were risk factors of overall survival. Conclusion: When the therapeutic approach is used in elderly patients with HCC, the patient's performance status, liver function, and stage of cancer should be considered, and its use should not be restricted to those of advanced age.
Hepatocellular carcinoma (HCC) is the fifth most common cancer worldwide and the second leading cause of cancer-related death (1, 2). The risk of developing HCC is well-known to be age-dependent (3, 4). Since an increase in the longevity of the general population is expected, there will be an increase in the number of elderly or even extreme elderly patients diagnosed with HCC.
The concept of “elderly” has become more difficult to define. The definition of elderly differs mostly because the life expectancy varies in different geographical areas (5). Most developed countries have accepted the chronological age of 65 years as the definition of an “elderly” person (6). However, many clinical studies about HCC define elderly patients as those aged 70 years or older (7-13). In South Korea, the average life expectancy is among the longest in the world. According to a report by Statistics Korea in 2015, the average life expectancy reached about 82.2 years (79.0 years for men and 85.6 years for women) (14). Moreover, the number of elderly patients with HCC was expected to increase gradually because of the following epidemiological reasons: i) The increasing incidence of liver cirrhosis is not associated with viral hepatitis or alcoholic steatohepatitis, which requires more time to develop into HCC (15); ii) antiviral agents have an effect on viral hepatitis and delay the natural course of the disease (16); and iii) hepatitis C due to infection generally occurs in adulthood.
Clinicians have difficulty in managing elderly patients with HCC because they have more comorbidities and are diagnosed as having advanced stage HCC compared to younger patients. In recent literature, there are no significant differences between elderly and younger patients' clinical outcomes after management of HCC (7, 8, 10-12, 17-19). Because previous large cohort studies showed that patients diagnosed as having HCC were aged between 70 and 75 years (7-13), there is an increasing need for tailored management based on age stratification in extreme elderly patients who have life expectancies less than 5 years. Therefore, it is important to evaluate the therapeutic safety in and long-term clinical outcomes of extreme elderly patients (age ≥75 years) with HCC.
In the present study, we compared the clinical characteristics and outcomes, including overall survival (OS), and treatment efficacy and safety, of elderly patients aged more than 75 years in South Korea.
Materials and Methods
Ethics statement. The study protocol was approved by the institutional review board of Chonnam National University Hospital (approval number: CNUH-2018-107). The need for informed consent requirement was waived because the patient data were de-identified.
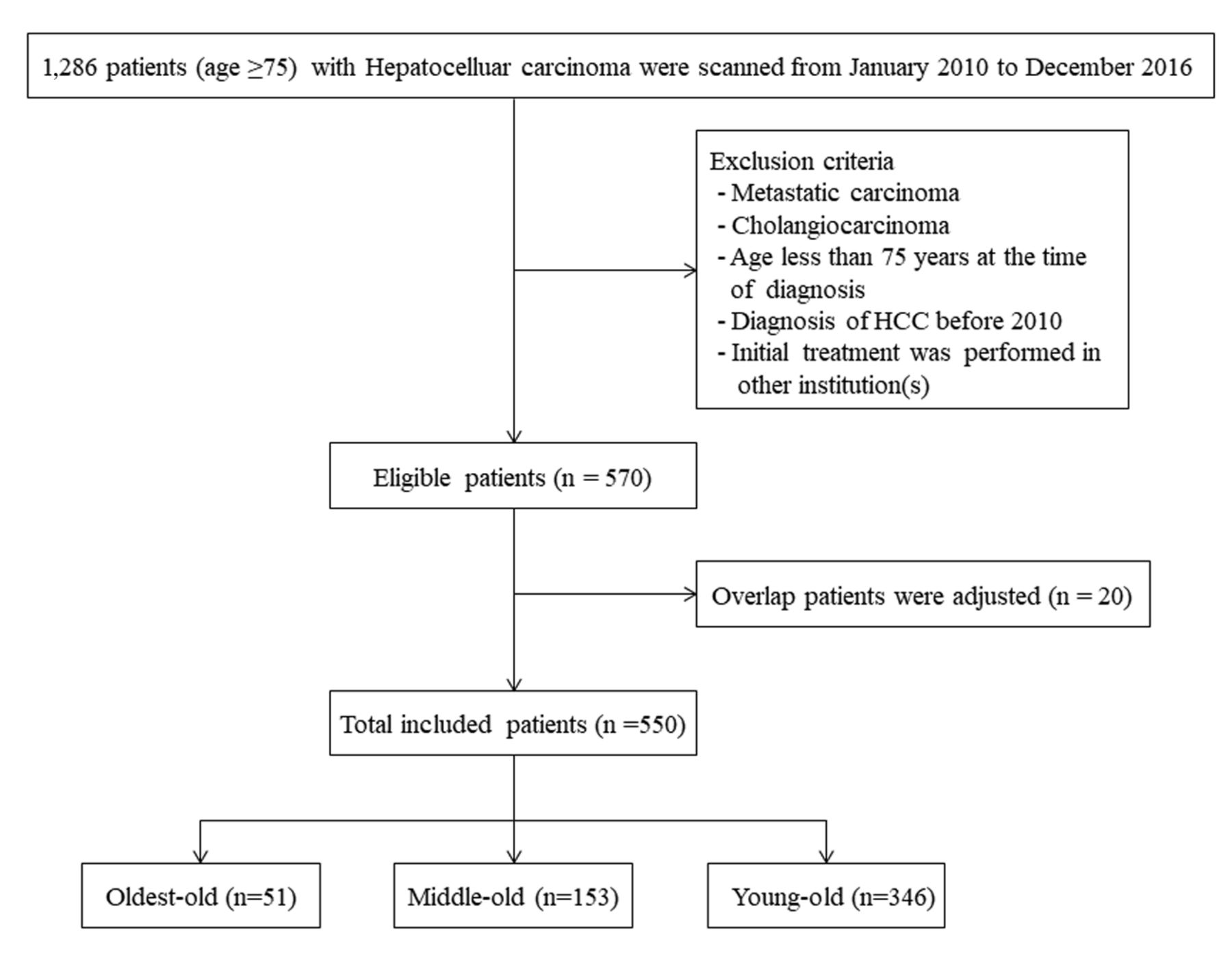
Study patients. We retrospectively analyzed 1,286 patients (age ≥75 years) who were diagnosed as having HCC in Chonnam National University Hospital of Gwangju, South Korea from January 2010 to December 2016. Seven hundred sixteen patients were excluded because of the following reasons: 1) the presence of metastatic carcinoma; 2) presence of cholangiocarcinoma; 3) age <75 years at the time of diagnosis; 4) diagnosis of HCC before 2010; and 5) the initial treatment was performed in other institution(s). The enrolled patients were divided into 3 groups according to other published studies: age ≥85 years (oldest-old group), age between 80 and 85 years (middle-old group), and age between 75 and 80 years (young-old group) (20, 21). All patients were followed until the occurrence of death, loss of follow-up, or end of follow-up (December 31, 2017). Information regarding death was collected by reviewing hospital medical records and entered into the Korean Statistical Information Service (KOSIS; http://kosis.kr).
The diagnosis of HCC was made based on the guidelines proposed by the Korea Liver Cancer Study Group (22).
Data collection and analysis. Data were collected to evaluate patients' clinical characteristics. Data recorded for each patient included age, sex, body mass index (BMI), comorbidities, the presence of the hepatitis B surface antigen (HBsAg), presence of the hepatitis C virus (HCV) antibody, presence of cirrhosis, alpha-fetoprotein (AFP) values, protein induced by vitamin K absence-II (PIVKA-II) values, presence of HCC rupture, size and number of tumors, presence of portal vein tumor thrombosis (PVTT), performance status according to the Eastern Cooperative Oncology Group, initial therapy, and OS. Levels of AFP and PIVKA-II were measured at the time of the diagnosis of HCC and divided into two categories: ≤200 IU/ml and >200 IU/ml; and ≤40 mAU/ml and >40 mAU/ml, respectively. The Child-Turcotte-Pugh (CTP) score and Model for End-Stage Liver Disease (MELD) score were used to evaluate liver function. The stage of HCC was assessed using the modified Union for International Cancer Control (mUICC) staging system and the Barcelona Clinic Liver Cancer (BCLC) staging system. If the patient was untreated, the initial treatment modality was regarded as conservative therapy. Treatment-related morbidity was defined as any complication within 30 days of treatment, and treatment-related mortality was defined as death from a complication within 30 days of treatment. Infection, which is a treatment-related complication, was defined as a positive blood/ascites/urine culture and concomitant patient symptom. Disease-free survival was defined as the interval during and after treatment in which a patient remained alive and the disease did not progress. Survival, including cause of death, was investigated by examining the final medical record and/or KOSIS. A survival census was performed on December 31, 2017.
Statistical analysis. Continuous data are expressed as a mean±standard deviation, and discrete variables as absolute and relative frequencies. One-way analysis of variance was used to determine whether there were any significant differences between the means of three independent groups. The chi-square test used 2×2 or 2×3 contingency tables for categorical data; the Fisher's exact test was used for cases with few expected frequencies (<5). Survival analysis was calculated from the time of cancer diagnosis to death with values censored at the date of the last follow-up, and these data were expressed as median and 95% confidence interval (CI). Survival analysis was performed using the Kaplan–Meier method and compared by the log-rank test. To assess the potential prognostic factors, univariate and multivariate analyses were performed using the Cox proportional hazard model. Variables associated with survival in the univariate analysis (p≤0.10) were entered into the Cox multivariate stepwise regression model to identify independent prognostic factors. The adjusted relative risk (hazard ratio) and 95%CI were calculated for each independent predictive factor. A two-tailed p-value <0.05 was considered statistically significant. All statistical analyses were performed using the SPSS 20.0 statistical package (SPSS Inc., Chicago, IL, USA).
Results
Figure 1 outlines the patient flow through the study. Of 550 enrolled patients, 51 (9.3%) were aged more than 85 years, 153 (27.8%) were aged between 80 and 85 years, and 346 (62.9%) were aged between 75 and 80 years.
Patients' baseline characteristics. Patients' demographic and clinical characteristics are summarized in Table I. There were 51 patients in the oldest-old group (mean age=87.6 years), 153 in the middle-old group (mean age=81.9 years), and 346 in the young-old group (mean age=77.1 years). The percentage of female patients was increased with age, but there was no significant difference between the groups. The etiology of liver disease showed some differences between the groups. Alcohol-related and hepatitis B virus (HBV)-related HCC, as determined by HBsAg positivity, was significantly decreased with age. Yet, there was no significant difference in the percentage of HCV-related HCC between the groups. There was a significant difference in the percentage of other etiologies between the groups. In addition, there was no significant difference in the percentage of diabetes mellitus (DM) and resolved HBV infection between the groups, as determined by HBsAg negativity and hepatitis B core antibody positivity with or without anti-HBs antibodies. However, compared to the other etiologies, obesity was significantly different between the groups. There was no significant difference between the groups with regard to BMI, underlying comorbid diseases, the presence of cirrhosis, liver function, presence of PVTT, rupture of HCC, and HCC stage. Active treatment had a statistically negative correlation with increasing age (oldest-old group: 35.3% versus middle-old group: 53.6% vs. young-old group: 65.3%, p<0.001).
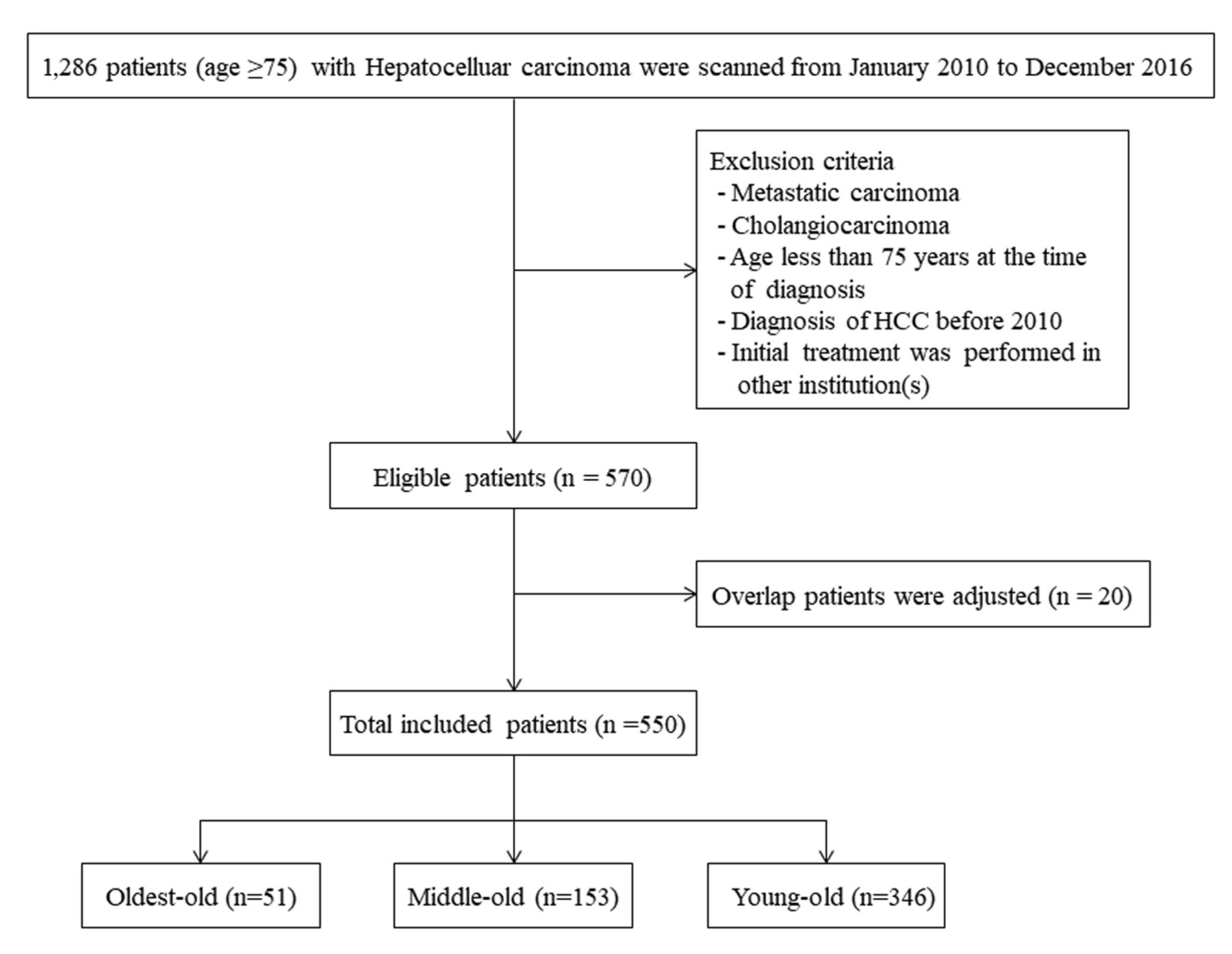
Flow chart of enrolled patients.
Comparison of treatment modalities. Table II shows the treatment modalities used in all 3 groups. Overall, 59.3% of patients underwent active treatment regardless of age. With increasing age, conservative treatment was predominant (oldest-old group: 62.7% vs. middle-old group: 40.5% vs. young-old group: 29.2%, p<0.001). Transarterial chemoembolization (TACE) was the main modality of treatment in all age groups, and it was applied at significantly different rates between the groups (oldest-old group: 21.6% vs. middle-old group: 34.6% vs. young-old group: 41.6%, p=0.014). The percentage of patients receiving, surgical resection, radiofrequency ablation (RFA), sorafenib, and radiotherapy was not significantly different between the groups (Table II).
Characteristics of patients who underwent active treatment. Table III shows the characteristics of patients who underwent active treatment in each age group. There was no significant difference in baseline liver function and HCC stage in the active treatment groups according to age. The consecutive second treatment (defined as switching the modality of treatment) was not significantly different between the groups. The treatment-related adverse events were not significantly different between the groups. The most common adverse event was post-TACE syndrome. Disease-free survival was not significantly different between the groups. The duration of hospital stay, need for intensive-care unit (ICU) care, and occurrence of infection were not significantly different between the groups. A serious adverse event related to treatment was reported in only 1 case in the middle-age group (Table IV).
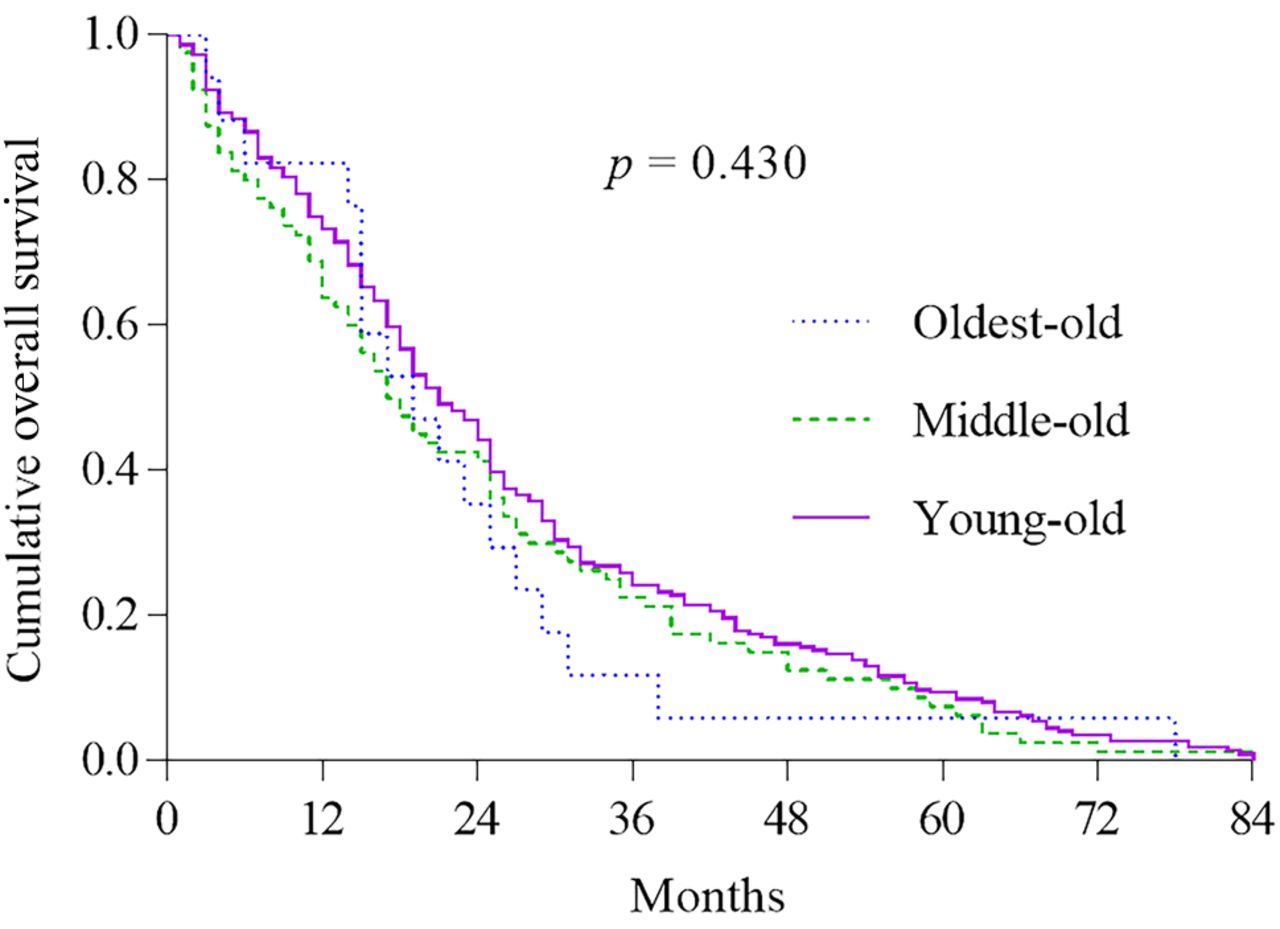
Comparison of overall survival between the groups. The mean durations of OS of patients receiving conservative/active treatment were 6.5/38.5 months in the oldest-old group, 11.8/41.5 months in the middle-old group, and 14.8/45.8 months in the young-old group (p=0.430) (Table III). There was a significant difference in OS depending on the active treatment used in all groups (Figures 2 and 3A-C).
A subgroup analysis was performed to exclude the possible effect of the tumor stage or active treatment on OS. OS between the active treatment group and conservative group was compared according to the mUICC stage and BCLC stage (Table V). To perform the subgroup analysis, the 3 groups were divided into 2 groups using different cutoff values for age: extreme elderly group (n=51, ≥85 years) and non-extreme elderly group (n=499, aged between 75 and 85 years). There were significant differences in OS between the active-treatment group and conservative group based on mUICC stages II and III, but there was no significant difference between the groups for mUICC stages IV-A and IV-B. Similarly, there was a significant difference in the OS between the active treatment group and conservative group based on BCLC stages B and C, but there was no significant difference in BCLC stage A in the extreme elderly group and BCLC stage D in the non-extreme elderly group (Table V).
Demographics and clinical characteristics of enrolled patients.
Factors related to survival. In the univariate Cox regression analysis, the variables associated with survival were age, BMI, the CTP score, MELD score, PIVKA-II level, tumor size, number of tumors, the presence of PVTT, rupture of HCC, modified UICC stage, BCLC stage, performance score, and active treatment. In the multivariate analysis, age (≥85 years), the MELD score, presence of PVTT, rupture of HCC, modified UICC stage, BCLC stage, performance score, and active treatment were significantly associated with OS in all groups (Table VI).
Discussion
In the present study, clinical characteristics and outcomes of extreme elderly patients with HCC were comprehensively assessed. The strength of our study was that it evaluated long-term follow-up data regarding patients' cause of death or overall survival for a large number of cases. Our study findings suggest that when using the therapeutic approach in elderly patients with HCC, the patient's performance status, liver function, and stage of cancer should be considered, and its use should not be restricted to those of advanced age. In contrast, conservative treatment should be considered in patients with advanced HCC (mUICC stage IV), those aged ≥85 years, and patients with poor liver function.
Treatment modalities of enrolled patients according to age group.
Characteristics of patients were underwent active treatment according to age groups.
In previous studies, elderly patients with HCC were more likely to be women (9, 23), and infected by HCV rather than HBV (24). However, extreme elderly patients with HCC in our study had a significantly lower rate of HBV infection and alcohol-related etiology, whereas the percentage of HCV and women showed a linear correlation without statistical significance. These findings might be explained by the following: 1) Our cohort had one of the highest seroprevalences of HCV, and affected patients were of advanced aged and had advanced severity of liver disease; thus, many individuals could not reach their expected life span because they had liver-related diseases, including but not limited to variceal bleeding, ascites or HCC (25). 2) Additionally, only patients with HCC aged more than 75 years were evaluated so the age difference was only 5 years between the groups.
In addition, our study showed that another etiology of HCC was the most common in the 80 years or older group. The subgroup analysis of other etiology of HCC showed no statistically significant difference in DM and resolved HBV infection. Moreover, the prevalence of obesity and DM was higher in the oldest-old group than in the middle-old group. This finding is likely associated with the increasing incidence of HCC related to non-alcoholic fatty liver disease (NAFLD) in elderly patients. Obesity and DM have been reported to be risk factors for HCC in large cohort and experimental studies (26, 27). The increased risk of HCC being associated with obesity and DM is probably due to the increased prevalence of NAFLD and the potential of the premalignant HCC condition to be related to obesity and DM (28).
Adverse events related to treatment.
Overall survival between active treatment group and conservative group according to the HCC staging.
In many studies, elderly patients with HCC were more likely to have a pauci-nodular HCC, less advanced fibrosis, and more preserved liver function (7, 29, 30). However, some studies reported no statistical difference between elderly and younger patients, and the tumor stage was not different in our patient groups (31-33). Conversely, our data did not show a difference in the number of tumors and fibrosis in terms of radiologic imaging or laboratory findings. Collier et al. and Dohmen et al. did not demonstrate any difference in results of liver function tests and the CTP score across age cutoffs of 65 or 70 years (31, 34). Our data also showed no significant difference in hepatic reserve function in terms of the CTP score and MELD score.
In general, elderly patients have a significantly higher percentage of comorbid diseases than younger patients do, and this could have affected patients' outcomes (7, 11, 18). However, most elderly patients with HCC aged over 80 years died of an HCC-related cause, and there were no significant differences in the percentage of liver-related deaths and deaths related to other causes between elderly and younger patients (18). Our study showed that elderly patients with HCC had more comorbidities, which is consistent with the result of a previous study (18). Although the prevalence of liver-related death was not assessed because of our retrospective study design, there was no significant difference in OS according to underlying comorbidities by age.

Cumulative overall survival between oldest-old (≥85 years), middle-old (between 85 and 80 years) and young-old (between 80 and 75 years) in HCC patient with active treatment. HCC: Hepatocellular carcinoma.
Regarding the initial treatment in our study, the oldest-old group received exclusively conservative treatment in 62.7% of the cases compared to only 40.5% and 29.2% in the middle-old group and young-old group, respectively. Similar to our study, previous studies reported that elderly patients with HCC were more likely to receive conservative treatment than were younger patients (31-33). Additionally, our patients received fewer curative treatments, such as surgical resection or RFA. These findings indicate that compared to younger patients, elderly patients received fewer aggressive or risky types of treatments, although there were no differences with respect to the prognosis of HCC treated with active treatment.
Consistent with other studies, (8-12, 32) no statistical difference was found in treatment-related adverse events and disease-free survival between the active treatment groups by age. Furthermore, there was no significant difference in the duration of hospital stay and need for ICU care. The most common adverse event was post-TACE syndrome, and treatment-related mortality occurred in only 1 case. The other types of complications did not increase with age. Our results suggest that active treatment is efficacious and safe in elderly patients with HCC.
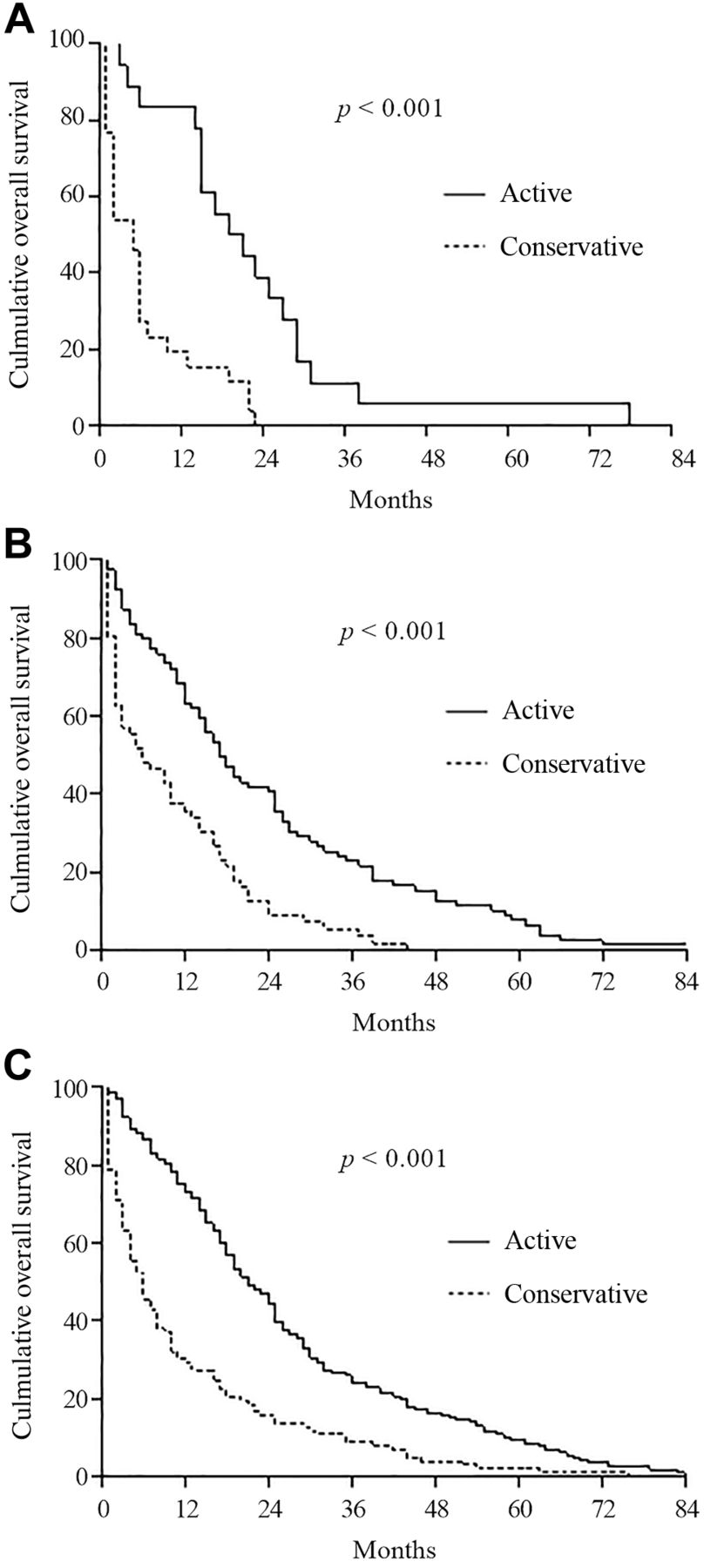
Cumulative overall survival between active treatment and conservative treatment by age groups. A: oldest-old group (≥85 years); B: Middle-old group (between 85 and 80 years); C: Young-old group (between 80 and 75 years).
Our results showed a significant difference in OS between the groups, and similar results were obtained in the subgroup analysis of the intermediate stages of cancer. This finding was consistent with findings of other recent reports (8, 13, 17), but they mostly studied patients aged 70 years or older (7, 10, 11, 18, 19). Hori et al. reported that OS was shorter for elderly patients (aged 75 years or older) than for younger patients. However, the OS of the elderly group, after excluding patients with supportive care alone, was similar to that of the younger group (17). Therefore, active treatment should be considered in patients with intermediate-stage HCC who have preserved liver function.
Univariate and multivariate analysis for mortality in all HCC patients.
In addition, the subgroup analysis of OS showed no statistical difference between the active-treatment group and conservative group, as stratified by BCLC stage A in the oldest-old group. We presumed that these patients who did not receive curative treatments because of their age or the presence of comorbidities despite having an early stage of HCC are more likely to die of cirrhotic complications or diseases other than progression of liver cancer.
Our multivariate analysis identified age (≥85 years), the MELD score, mUICC stage, BCLC stage, presence of PVTT, rupture of HCC, performance score, and active treatment as significant independent prognostic factors of OS. In contrast to a previous report (29, 30, 33-37), advanced age was one of the factors contributing to poor prognosis in patients with HCC, but this was similar to the finding of one recent report (13). Suda et al. highlighted that aging was not a poor prognostic factor affecting OS of patients with HCC when the survival benefit was evaluated based on the percent survival to life expectancy (a ratio of the survival days to the expected residual life length). Therefore, the therapeutic approach should not be restricted because of patient's age (13).
This study had several limitations. First, it was a retrospective, single-center study. Thus, the possibility of unintended selection bias could not be excluded. Second, we only analyzed the initial treatment outcomes, although many patients were treated with various and multiple treatment modalities during the follow-up period. Therefore, it was difficult to evaluate the effects of all the therapies on prognosis in this cohort. More prospective studies are needed to confirm our findings.
In conclusion, our data support that the treatment strategy of HCC does not differ between elderly patients including extreme elderly patients and younger patients. Hence, clinicians should determine the optimal treatment strategies based on the patients' performance status, hepatic reserve capacity, and tumor stage, regardless of their age and comorbidities.
Acknowledgements
This work was supported by Grants (CRI 1809-1 and CRI 17027-1) from the Chonnam National University Hospital Biomedical Research Institute.
Footnotes
This article is freely accessible online.
Conflicts of Interest
There are no conflicts of interest regarding this study.
- Received September 20, 2018.
- Revision received October 8, 2018.
- Accepted October 9, 2018.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}
{kind=link}
{kind=link}