


Abstract
Background/Aim: Idiopathic pulmonary fibrosis IPF is a type of interstitial lung disease (ILD) with poor prognosis. Lung cancer (LC) is a frequent complication in IPF, where all therapeutic options are potential triggers for acute exacerbation of IPF. Patients and Methods: Patients with 2-deoxy-2-fluoro-D-glucose-positron emission tomography/computer tomography (FDG-PET/CT) results before lobectomy for LC with and without (n=10 each) signs of ILD in initial imaging and after-care CT were retrospectively analyzed. FDG uptake was calculated as the maximum standardized uptake value (SUVmax) in the lung periphery divided by the SUVmax of the mediastinal blood pool (rSUVmax). Regional increase of fibrosis and ground-glass features in lobe-based CT analysis was used as standard reference. Results: Patients with LC with ILD presented a significantly higher rSUVmax of 0.57 compared to patients without ILD with rSUVmax 0.47 (p<0.001). Conclusion: rSUVmax seems to be a valuable imaging surrogate in predicting patients with LC with increased risk for progressive ILD associated with thoracic surgery.
Interstitial lung diseases (ILD) are associated with an increased mortality (1-3). Idiopathic pulmonary fibrosis (IPF), in particular, has an increasing incidence, and can be classified as a life-threatening condition, associated with a median survival of 3-4 years, comparable to that of patients suffering from malignant diseases (4). As reported in a study evaluating more than 9,000 patients with IPF in the US, comorbidities in IPF are frequent and associated with an increased mortality (4, 5). Moreover, an increased risk for the development of lung cancer (LC) was shown in a recent study evaluating comorbidities of more than 5,000 patients with IPF in Japan, with a prevalence of 3.7% for those hospitalized with IPF (6). Similarly, an increased incidence of LC has been highlighted in patients with IPF in two studies from the UK (7, 8).
Due to the increased risk for LC in patients with ILD, therapeutic stratifications are often difficult (9). In clinical routine, high-resolution computed tomography (HRCT) is essential for the diagnosis of ILD, including IPF (10). The role of 2-deoxy-2-[18F]fluoro-D-glucose positron-emission tomography/CT (18F-FDG-PET/CT) in ILD has not been elucidated. Nevertheless, several studies have documented an increased FDG uptake in patients with IPF undergoing PET/CT (10-13). In particular, the observed increase of standardized uptake value (SUVmax) has been shown to be useful for the prediction of functional improvement under drug treatment (13). Interestingly, an increased FDG uptake was not only found in areas of destroyed lung architecture, but also in areas of the lung with normal morphological appearance (10). Moreover, an increased retention index value (RI-SUV) in dual-time-point 18F-FDG-PET was described as an independent prognostic factor for shorter progression-free survival (12).
18F-FDG-PET/CT serves as a routine staging methodology in patients with LC (14). Since surgery for LC is an established risk factor for exacerbation of pre-existing IPF (15-19), associated with significant disease progression and a high mortality, individual risk assessment might be improved if 18F-FDG-PET/CT could also help to predict this dreadful complication. In order to further exhaust the clinical information derived from routinely performed pre-operative 18F-FDG-PET/CT examinations in patients with LC, the impact of FDG uptake in peripheral lung parenchyma on the progression of pre-existing ILD was evaluated. The hypothesis of this study was that increased FDG uptake in peripheral lung tissue in PET/CT might be used as an imaging surrogate for the differentiation between patients with surgery-triggered progression of pre-existing ILD, and patients that do not have an increased risk for ILD.
Materials and Methods
Study design and patients. Patient selection was performed using a database of more than 200 patients suffering from non-small cell LC with available pre-operative 18F-FDG-PET/CT as well as postoperative CT. Patients with prior radiation or chemotherapy were excluded from the analysis, as well as patients with preoperative CT scans with severe artefacts due to metal implants or breathing artefacts. Finally, 20 patients (50% male; median age=67 years, range=55-85 years) were analyzed retrospectively using a single-center design, and two groups were formed and compared: one group with 10 consecutive patients with pre-existing and progressive ILD by postoperative imaging (ILD group), and a second group with 10 patients with no signs of ILD in initial and follow-up imaging (control group).
Regional radiological signs for ILD as visually detectable at initial and follow-up CT were used as gold standard. All 18F-FDG-PET/CT examinations were performed according to the clinical schedule within 2 weeks prior to surgery. FDG uptake was measured once prior to surgery in the preoperative 18F-FDG-PET/CT examination in all patients. Absence and presence of ILD was quantified accordingly in pre-and postoperative follow-up CT examinations. Up to three postoperative CT scans were reviewed per patient, covering a time frame after surgery of a median of 408 (range=159-716) days in the ILD group and 320 (range=81-1159) days in the control group. The study was approved by the Institutional Review Board (080/2006) and conducted according to the guidelines of the Institutional Review Board and to good clinical practice according to the ethical principles that have their origin in the Declaration of Helsinki. In this retrospective analysis, the requirement for informed consent was waived by the Institutional Review Board.
Imaging procedures. 18F-FDG-PET/CT: 18F-FDG-PET/CT examinations were performed as part of preoperative staging according to clinical routine using a Biograph 6 PET/CT Scanner (Siemens, Erlangen, Germany). Imaging sequences and protocols were described earlier in detail (20, 21): after fasting for at least 6 hours (blood glucose level below 150 mg/dl), 4 MBq/kg body weight of 18F-FDG were administered intravenously 60±5 minutes before the FDG-PET/CT scan. The following examination protocols and reconstruction parameters were applied: slice thickness/reconstruction increment of 5.0/2.5 mm, standard soft-tissue reconstruction kernel B30 and B70 high-resolution. Static emission scans (eight bed positions, 4 minutes each) from the vertex to the proximal legs were performed with correction for dead time, scatter and decay. Non-enhanced low-dose CT was acquired for reasons of attenuation correction. For iterative image reconstructions, ordered subset expectation maximization (OSEM) algorithm was applied (four iterations, eight subsets and Gaussian filtering), resulting in an in-plane spatial resolution of 5 mm at full-width half-maximum. In cases where no preoperative CT was available, fibrotic remodeling was examined on the basis of non-enhanced CT scans that accompanied the preoperative 18F-FDG-PET/CT scan. CT parameters were adjusted according to patient's weight (120 keV, 40-150 mAs) using a section width of 5 mm and pitch of 0.8°.
Pre-and post-operative CT: According to clinical routine, eight out of 20 patients underwent initial CT for preoperative staging as inspiratory CT, which was technically identical to the scans that were performed postoperatively. In another 12 patients, initial quantification of fibrotic lung disease was performed using the CT component of the above mentioned 18F-FDG-PET/CT examination in respiratory center position, since other CT scans were outdated, impeded by artefacts, or performed with very thick sections. Preoperative CT scan was taken at a median of 24 (range=0-49) days prior surgery. The distribution of the above-mentioned issues was identical in both groups. Concerning postoperative follow-up assessments of ILD, all examinations were performed as part of routinely performed oncological aftercare as contrast-enhanced CT examinations using an AS64 CT scanner (Siemens) with a biphasic intravenous injection of 40 ml at 2 ml/s contrast agent (Ultravist 300; Bayer Vital, Leverkusen, Germany) followed by a second bolus of 60 ml at 2 ml/s after 40 s with 30 ml of saline flush covering from below the adrenal glands through the lung apices. CT data sets were reconstructed at a slice thickness of 3.0 mm using a 2.5-mm increment with an I30 standard soft-tissue kernel and an I70 high-resolution kernel.
Image analysis and quantification. As described earlier (22), quantification of SUVmax was examined in reconstructed non-contrast-enhanced CT and PET images that were displayed on a dedicated workstation equipped with Syngo software (Siemens). Clinical image interpretation was carried out by one Board-approved nuclear medicine physician and one Board-approved radiologist (23-25). Both readers were blinded to clinical information. For the analysis of the PET component, a semi-automatic spherical volume of interest (VOI) was drawn on each of the six lung lobes with lingula serving as the left equivalent to the middle lobe. When necessary, borders of each VOI were adjusted manually in all three dimensions in order to exclude the adjacent chest wall, tumor tissue or surrounding vessels. Moreover, a VOI in the descending aorta was drawn to measure SUVmax of the blood pool (BP). FDG uptake was evaluated using the parameter SUVmax calculated 60 minutes after tracer injection. The relative SUVmax (rSUVmax) was calculated as the SUVmax in the lung periphery divided by the SUVmax of the mediastinal BP, which was measured in the ascending aorta.
The amount of ILD was estimated visually as the percentage of tissue within the respective lobe affected by fibrosis and ground-glass attenuation, according to a recent publication (26). According to the underlying disease and ongoing treatment, the change in follow-up CT was only available for non-resected (n=21), non-irradiated (n=2), nor otherwise affected lobes (i.e. compression atelectasis due to effusion, n=2).

Initial 2-deoxy-2-[18F]fluoro-D-glucose-positron- emission tomography/computer tomography (18F-FDG-PET/CT), initial and follow-up CT. A: Patient with interstitial lung disease (ILD; ILD group). B: Patient with no signs of ILD (control group). I: 18F-FDG-PET/CT with multi-intensity projection of PET (red line indicating slices for axial images). II: Fused axial PET/CT, orange circle indicates region of interest (ROI) for maximum standardized uptake value (SUVmax) measurement. III: Axial views of PET, orange circle indicates ROI for SUVmax measurement. IV: Axial views of initial CT as part of integrated 18F-FDG-PET/CT. V: Axial views of postoperative contrast-enhanced follow-up CT.
Statistical analysis. Statistical analysis was based on a lobe-based analysis using SigmaPlot (Systat Software GmbH, Erkrath, North Rhine-Westphalia, Germany). Median and quartile values for SUVmax with 95% confidence interval were calculated and illustrated in box-and-whisker plots using the results for fibrotic progression from follow-up CT examinations as standard of reference.
For comparison of uptake values, the non-parametric Wilcoxon signed-rank test for two paired samples was used. The significance level used was p≤0.05 (two-tailed). Sensitivities and specificities of all measured markers were investigated using receiver operating characteristic (ROC) analysis and the area under the ROC curve (AUC).
Results
FDG uptake in preoperative 18F-FDG-PET/CT. For the semi-automated analysis of FDG uptake of peripheral lung parenchyma in the fused images of 18F-FDG-PET, less than 10 minutes of additional reading time was necessary for each patient (Figure 1). Semi-automated quantification of fibrotic remodeling in the CT component of integrated 18F-FDG-PET/CT or CT resulted in an extra reading time of not more than 10 minutes for each patient.
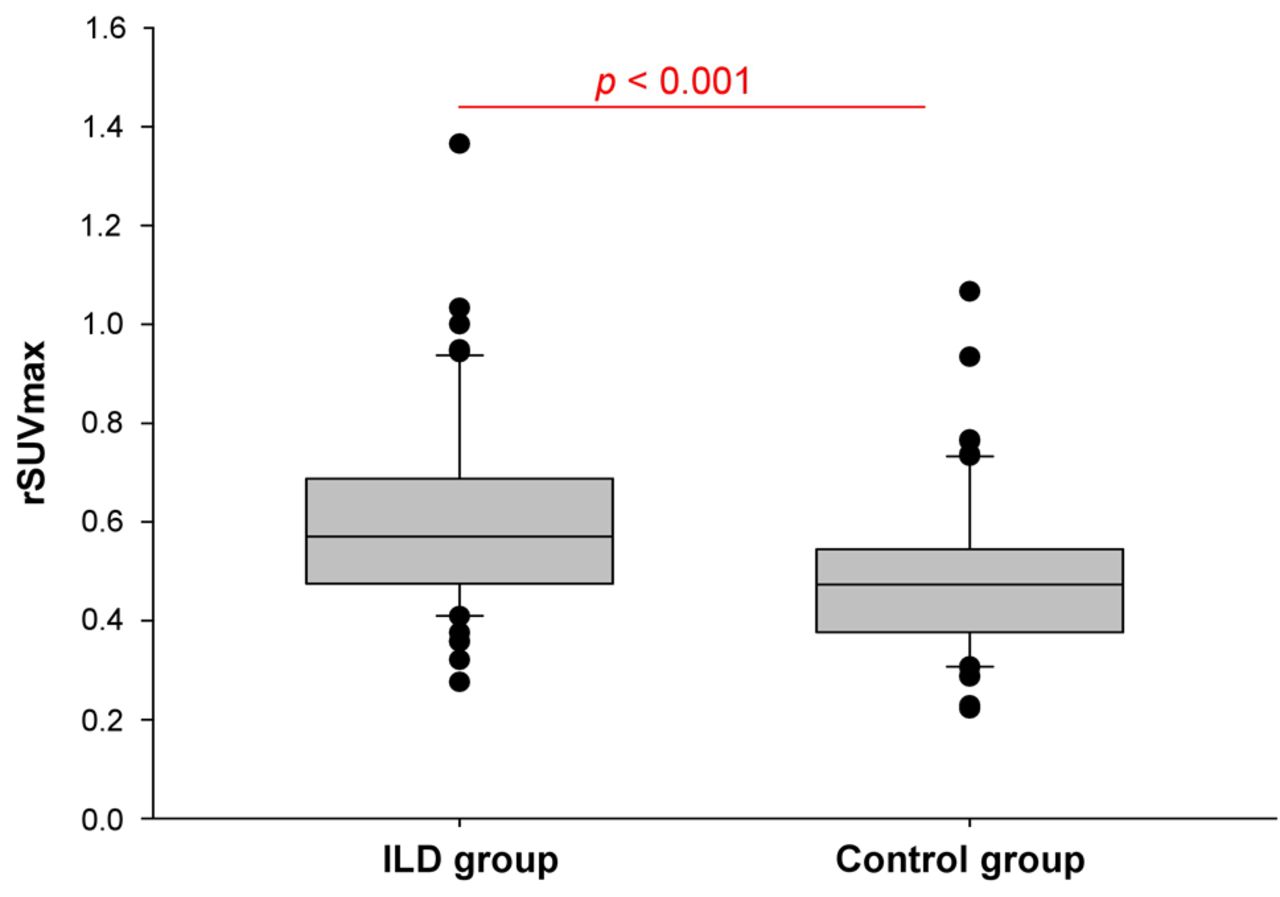
Regarding FDG uptake, rSUVmax in peripheral lung parenchyma was significantly higher in the VOIs of patients suffering from ILD compared to the control group. In detail, patients with ILD presented a median rSUVmax of 0.57 (0.27-1.38) compared to a 0.47 (0.22-1.07) in the control group (p<0.001; Figure 2). Concerning the analysis of absolute SUVmax, patients with ILD presented a median SUVmax of 1.15 (0.47-2.47) compared to 1.00 (0.55-2.01) of the control group, which was not statistically significantly different (p=0.19).
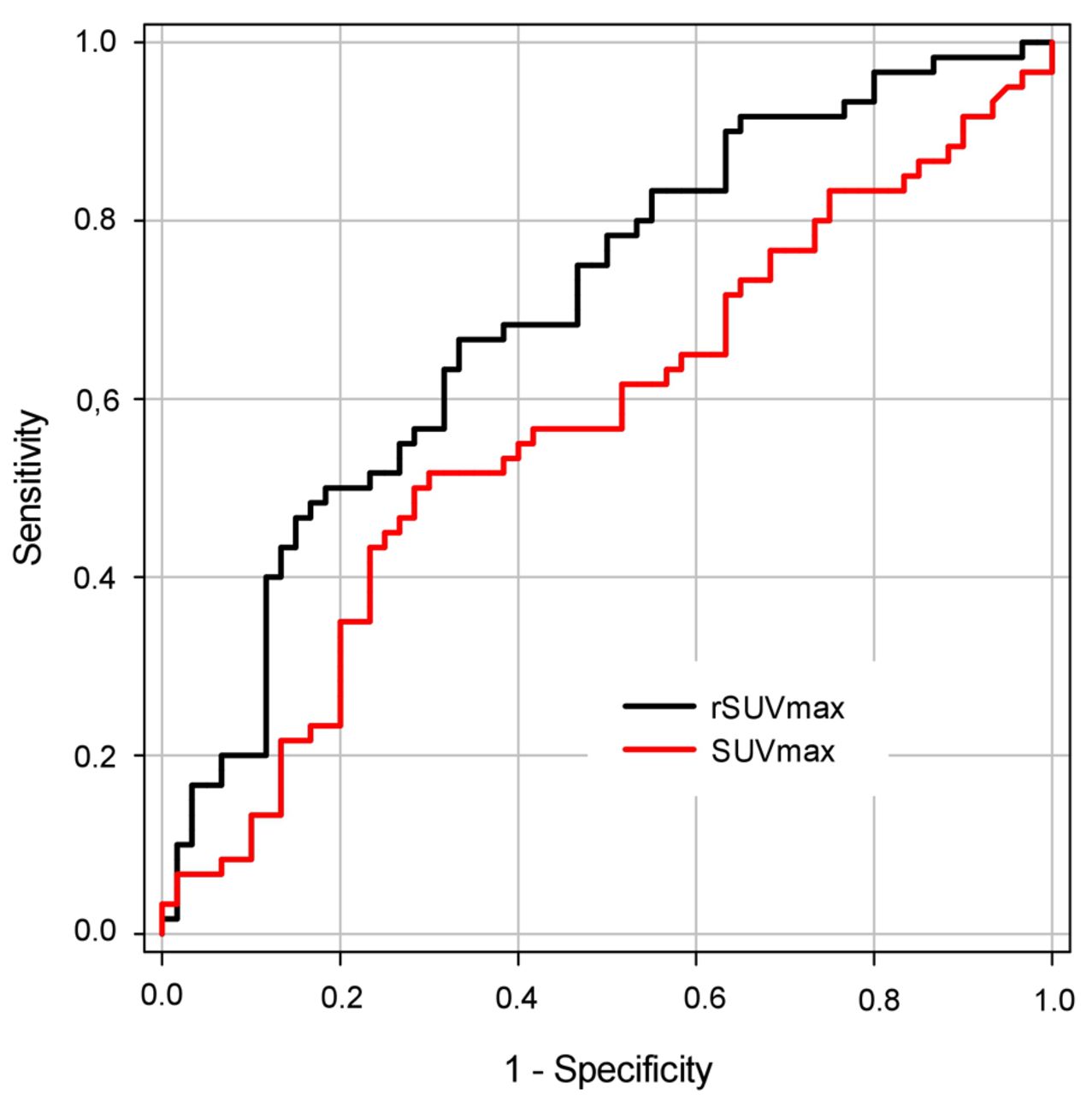
ROC analyses and AUC. In order to compare the impact of SUVmax and rSUVmax for the prediction of progressive ILD, the correlation between SUVmax, rSUVmax, and the gold standard (regional radiological signs for ILD by CT) were performed using receiver operating characteristic (ROC) and area under the curve (AUC) analyses. For ROC analyses, the calculated AUC for rSUVmax was 0.70 (95% confidence interval=0.61-0.79), while that for SUVmax was 0.57 (95% confidence interval=0.47-0.67; Figure 3), indicating that there is a stronger correlation between the parameter rSUVmax and the above-mentioned gold standard (regional radiological signs for ILD by CT), compared to the correlation between SUVmax and the gold standard.

Box plots of relative maximum standardized uptake value (rSUVmax) in peripheral lung tissue in patients with interstitial lung disease ILD and the control group without ILD. values for the lobe-based parameter rSUVmax was significantly higher in patients with ILD compared to the control group (p<0.001). Lines indicate median values, boxes indicate the values between the upper and the lower quartile, whiskers indicate 95% confidence interval, and dots indicate outliers.
Discussion
Comparing FDG uptake in patients with LC between patients in the ILD group and those in the control group, we found significantly higher values for SUVmax in patients with ILD, confirming the hypothesis of this study that an increased FDG uptake in peripheral lung tissue can be used as an imaging surrogate for the differentiation between patients with surgery-triggered progression of pre-existing ILD and those that do not have an increased risk for ILD. ROC analyses revealed a higher correlation between rSUVmax and the presence of ILD as compared to the gold standard SUVmax.
In clinical routine, the introduction of a threshold value for the differentiation between patients with and without ILD could potentially help to identify those patients that have an increased risk for the onset or progression of ILD. This information could help to identify patients with increased risk for progressive ILD after lung surgery, thereby influencing clinical decision-making for therapy stratification, especially in those patients with impaired lung function. In particular, patients at high risk for ILD could potentially benefit more when stratified to a non-invasive therapeutic procedure, since surgery is known to be a trigger for the exacerbation of ILD, such as IPF (15-19). If necessary, patients at high risk for progressive ILD might be treated with additional medication in order to prevent further progression of ILD, even in cases lacking or showing few signs of ILD in CT (27). In a second step, it would be of interest to compare overall survival of patients with LC at high risk for progression of pre-existing ILD that undergo non-surgical therapy with those treated with surgical therapy in order to ensure that high-risk patients have benefits when stratified for non-invasive care. Importantly, the acquisition of this information does not significantly affect the workload of the department, since patients with LC are routinely managed with 18F-FDG-PET/CT, and semi-automated SUVmax and rSUVmax measurements in the lung periphery can be derived within less than 10 minutes for each patient, as stated in the present study.

Area under the curve (AUC) analysis for maximum standardized uptake value (SUVmax) and relative maximum standardized uptake value (rSUVmax). Receiver operating characteristic analysis comparing the SUVmax and rSUVmax in patients with and without interstitial lung disease gave an AUC for rSUVmax of 0.70 (95% confidence interval=0.61-0.79), and 0.57 (95% confidence interval=0.47-0.67) for SUVmax.
Results from the present pilot study are supportive of findings published in previous articles that demonstrated increased FDG uptake in the lung parenchyma of patients with IPF (10-13). As stated by Win et al., 18F-FDG-PET seems to have an even higher sensitivity for the detection of early pulmonary diseases in IPF as compared to HRCT (10). Nevertheless, the underlying pathogenesis of IPF (28-31), as well as the pathophysiological process that is responsible for the increased FDG uptake even in lung areas with normal HRCT signs are not yet understood (10). According to these authors, the presence of diffusely increased pulmonary SUVmax implies that increased FDG uptake is not predominantly caused by the colonization of infiltrates following infection due to dilated airways (10). Nevertheless, 18F-FDG-PET has been introduced as a surrogate endpoint for clinical trials evaluating the therapeutic benefit of newly introduced drugs against IPF (10). In diseases other than IPF, 18F-FDG-PET/CT is already used as an imaging surrogate for therapy response, as for example in patients suffering from lymphoma, when using the well-established Deauville score (32-38).
Our study has some limitations. One is its retrospective design with the relatively small number of 20 patients included in this pilot study. Secondly, in some patients lacking preoperative inspiratory CT, ILD was quantified using low-dose CT accompanying the PET scan. These CT scans were performed in respiratory center position, which weakens the CT-based diagnosis of ILD. In order to address this limitation, an identical number of patients also lacking initial inspiratory CT were included in the ILD and the control groups. In addition, postoperative CT scans were performed as part of oncological aftercare using contrast agent, which is not the clinical standard for the interpretation of interstitial lung diseases when performing dedicated CT scans for ILD imaging. In addition, in larger prospective studies, the clinical impact of SUVmax-and rSUVmax-based ILD analysis on overall survival could be compared, especially when stratifying high-risk patients for non-surgical treatment, and those with lower or moderate risk for surgery.
In conclusion, patients with LC scheduled for surgical treatment with pre-existing ILD presented significantly higher rSUVmax in 18F-FDG-PET/CT compared to patients of the control group, leading to us to propose rSUVmax as a valuable imaging surrogate for the detection of progressive ILD in postoperative follow-up. Since surgery is a possible trigger for the exacerbation of IPF, the identification of patients with increased rSUVmax could lead to their stratification as being at high risk for progressive ILD, and to their potential exclusion from surgical resection, or administration of supportive medication when available. Nevertheless, the introduction of dedicated rSUVmax-based thresholds for the differentiation of high-risk patients from those with lower or moderate risk should be performed in prospective studies with larger numbers of patients.
Footnotes
This article is freely accessible online.
- Received June 11, 2018.
- Revision received June 25, 2018.
- Accepted June 28, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.